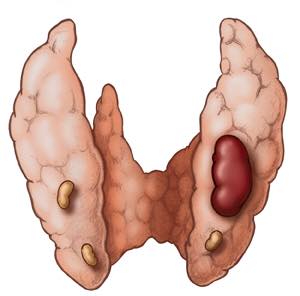
- Primary Hyperparathyroidism is suffered by patients who present with:
- Elevated calcium serum levels and excessively high levels of parathyroid hormone (PTH):
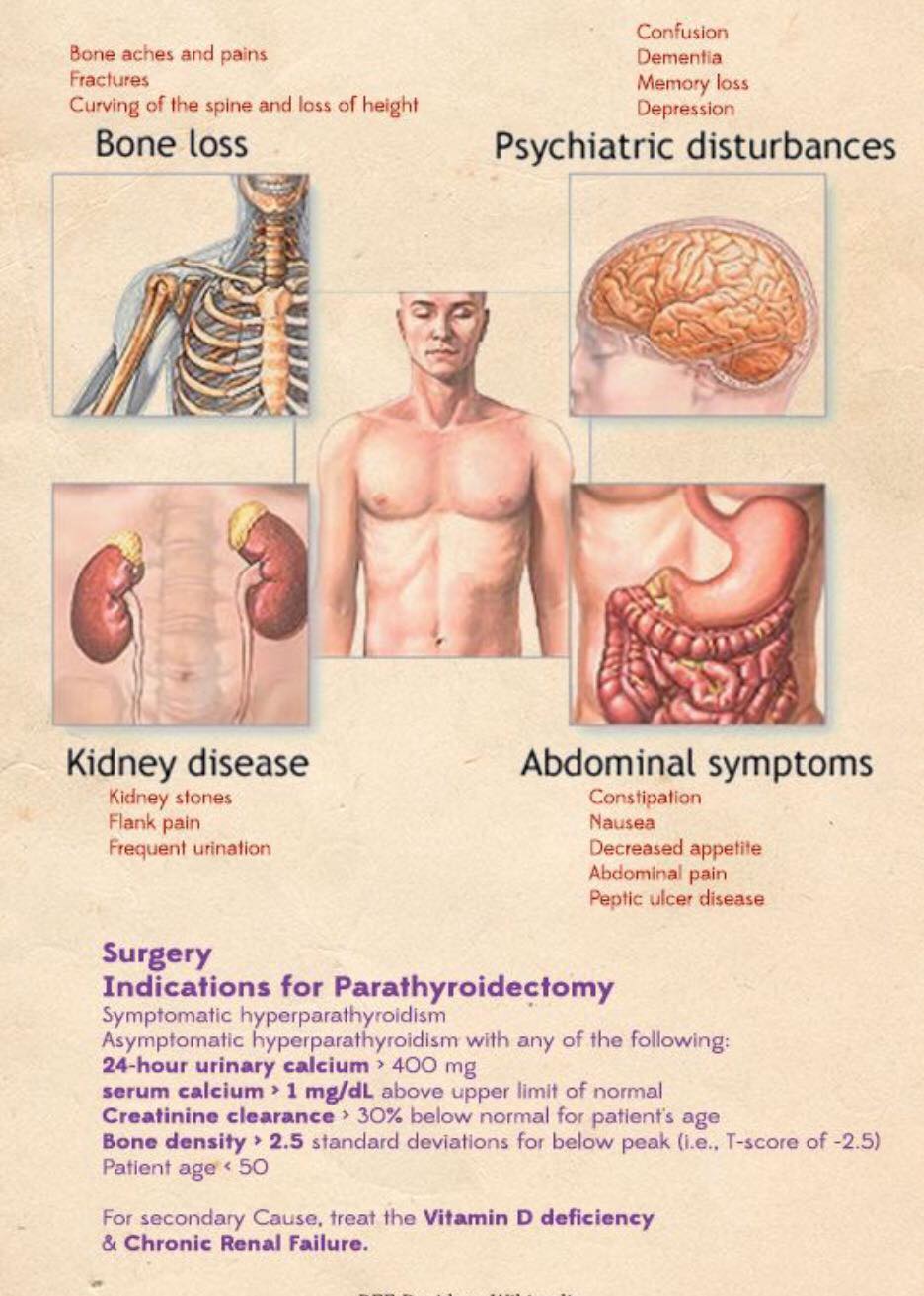
- Other characteristics are usually associated with it:
- But are not necessary for diagnosis
- In recent years, an alternative approach to parathyroidectomy has been developed:
- Traditional surgery is performed under general anesthesia, and makes it possible to explore all the parathyroid glands
- By contrast, minimally invasive surgery:
- Is used in uniglandular disease with preoperative location of the hyper functioning gland responsible for hyperparathyroidism:
- Today I can perform a bilateral exploration through a 2 cm incision without any difficulty
- The SPECT-Tc 99 sestamibi, 4D CT scan with parathyroid protocol, and PET- CT scan are currently the most valuable techniques to locate the gland or glands that are hyper functioning prior to surgery:
- This approach makes it possible to perform the surgery under local nerve blockade in very select cases when general anesthesia is contraindicated due to the medical co morbidities of the patient
- Several studies have concluded that a minimally invasive approach to primary hyperparathyroidism is equivalent to bilateral exploration when intraoperative parathyroid hormone (IOPTH) monitoring is used:
- With the technique that I employ I can perform a bilateral neck exploration through a 2 cm incision decreasing the chance of not curing the patient
- Some resolution criteria have been defined to make sure during the surgery that the gland responsible for the disease has been correctly resected:
- These are the current criteria:
- Rome criteria:
- They require a greater than 50% drop from the highest pre-excision PTH level, and / or PTH level within the reference range 20 minutes post excision, and / or a PTH level 7.5 ng/dL lower than the 10 minutes post excision level
- Halle criteria:
- They require the IOPT to fall within the low normal range (less than 35 ng/dL) within 15 minutes from removing all hyper functioning parathyroid glands
- Vienna criteria:
- They require taking a baseline pre-incision PTH sample before neck manipulation
- A PTH drop greater than 50% from the baseline PTH level at 10 minutes from gland resection indicates a successful operation
- Miami criteria:
- But the most widely accepted guideline is the Miami criterion
- Which is a 50% decline from the highest pre-incision or pre-excision IOPTH level obtained 10 minutes after excision of the hyper-secreting parathyroid gland:
- It is important to know that PTH has a half-life of 5 minutes to confirm the complete excision of the diseased tissue
- Preoperative PTH must be measured
- To meet the Miami criterion, a PTH level measurement should be taken 5 minutes from gland excision:
- PTH levels decrease by more than 50% once the gland has been successfully removed

Rodrigo Arrangoiz MS, MD, FACS cirujano de tumores de cabeza y cuello / cirugia endocrina es experto en el manejo del hiperp
Dr. Rodrigo Arrangoiz is a board-certified surgical oncologist who subspecializes in breast cancer and head and neck cancer. Dr. Arrangoiz earned his medical degree at the Anahuac University Medical School in Mexico City, Mexico and graduated Suma Cum Laude. He completed his internship and residency in general surgery at Michigan State University, where he was named chief resident during his fifth year of residency. Dr. Arrangoiz also completed a complex surgical oncology, head and neck fellowship at the Fox Chase Cancer Center in Philadelphia and at the same time he undertook a master’s in science (Clinical Research for Health Care Professionals) at Drexel University in Philadelphia. Dr. Arrangoiz also participated in a two-year global online fellowship in head and neck surgery and oncology through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center.
Dr. Arrangoiz has participated in multiple courses and academic congresses as a lecturer and guest professor and has also participated in several publications on topics related to his specialty that include oral cavity cancer, hyperparathyroidism, thyroid cancer, breast cancer, endocrine tumors, squamous cell carcinoma of the head and neck, and more. He is board certified by the American Board of Surgery, the Mexican Board of General Surgery and the Mexican Board of Oncology.
He is a member of various medical associations such as the American College of Surgeons, American Thyroid Association, American Head and Neck Society, American Medical Association, American Society of Clinical Oncology, Association of Academic Surgeons, Society of Surgical Oncology, The Society of Surgery of the Alimentary Tract, Society of American Gastrointestinal Endoscopic Surgeons, and the American Society of Breast Surgeons, among others.
Specialty:
Head and Neck Surgery
Thyroid and Parathyroid Surgery
Breast Surgery
Complex Surgical Oncology
Areas of Clinical Interest:
Malignant thyroid disease (papillary, follicular, medullary, anaplastic thyroid cancer, thyroid lymphoma, and metastatic disease to the thyroid gland) benign thyroid diseases (goiter, multinodular goiter, substernal goiter, hyperthyroidism), hyperparathyroidism / hypercalcemia, benign and malignant breast diseases, head and neck surgery and head and neck canc
 https://m.youtube.com/watch?v=AgvQmtz1gnA&time_continue=127
https://m.youtube.com/watch?v=AgvQmtz1gnA&time_continue=127
#Arrangoiz #ParathyroidSurgeon #ParathyroidExpert #Hyperparathyroidism #PrimaryHyperparathyroidism #CancerSurgeon #EndocrineSurgery #Teacher #Surgeon #HeadandNeckSurgeon #SurgicalOncologist #ParathyroidAdenoma #Hypercalcemia #ElevatedCalciumLevels #Miami #MountSinaiMedicalCenter #MSMC #Mexico #Hialeah