- Ductal calcifications have a wide variety of presentations:
- Depending upon the underlying process that created them
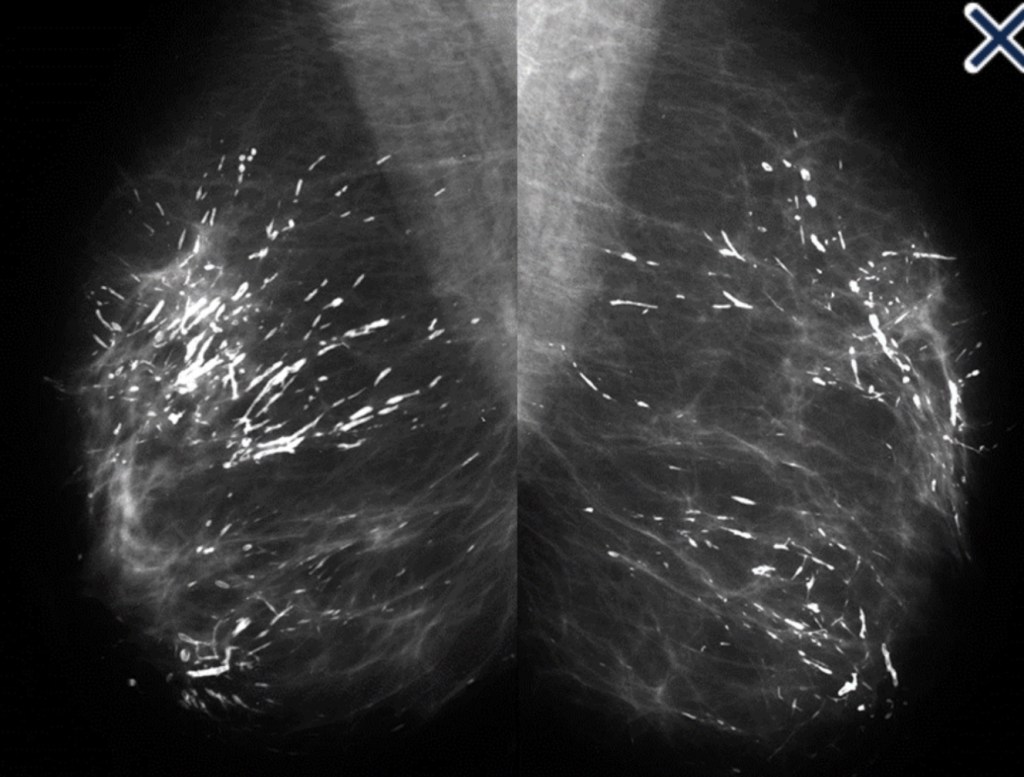
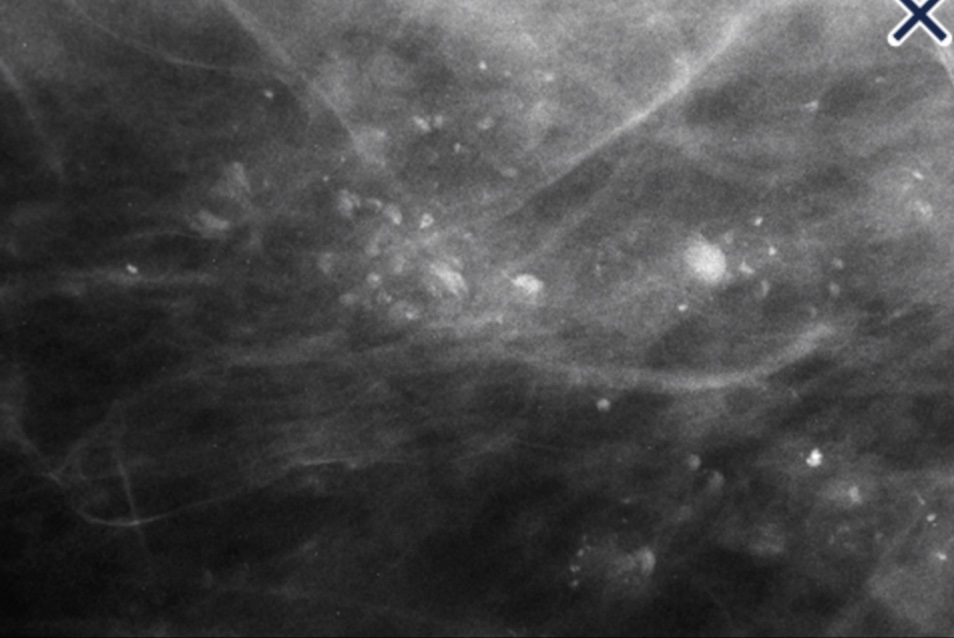
- When coarse rod-like ductal calcifications:
- Are diffuse, bilateral, and not confined to a single lobe:
- They can be confidently assumed to result from plasma cell mastitis:
- They do not require further evaluation or biopsy (Image)
- The process is called secretory disease:
- Because there is a stagnant, viscous fluid that eventually petrifies and results in the smooth contoured calcifications
- Some of them are branching and look like malignant casting type calcifications:
- But the key distinguishing feature:
- Is the diffuse, multilobe, bilateral nature of the process:
- Calcifications become much more worrisome when they are confined to a single lobe
- Is the diffuse, multilobe, bilateral nature of the process:
- But the key distinguishing feature:
- They can be confidently assumed to result from plasma cell mastitis:
- Are diffuse, bilateral, and not confined to a single lobe:

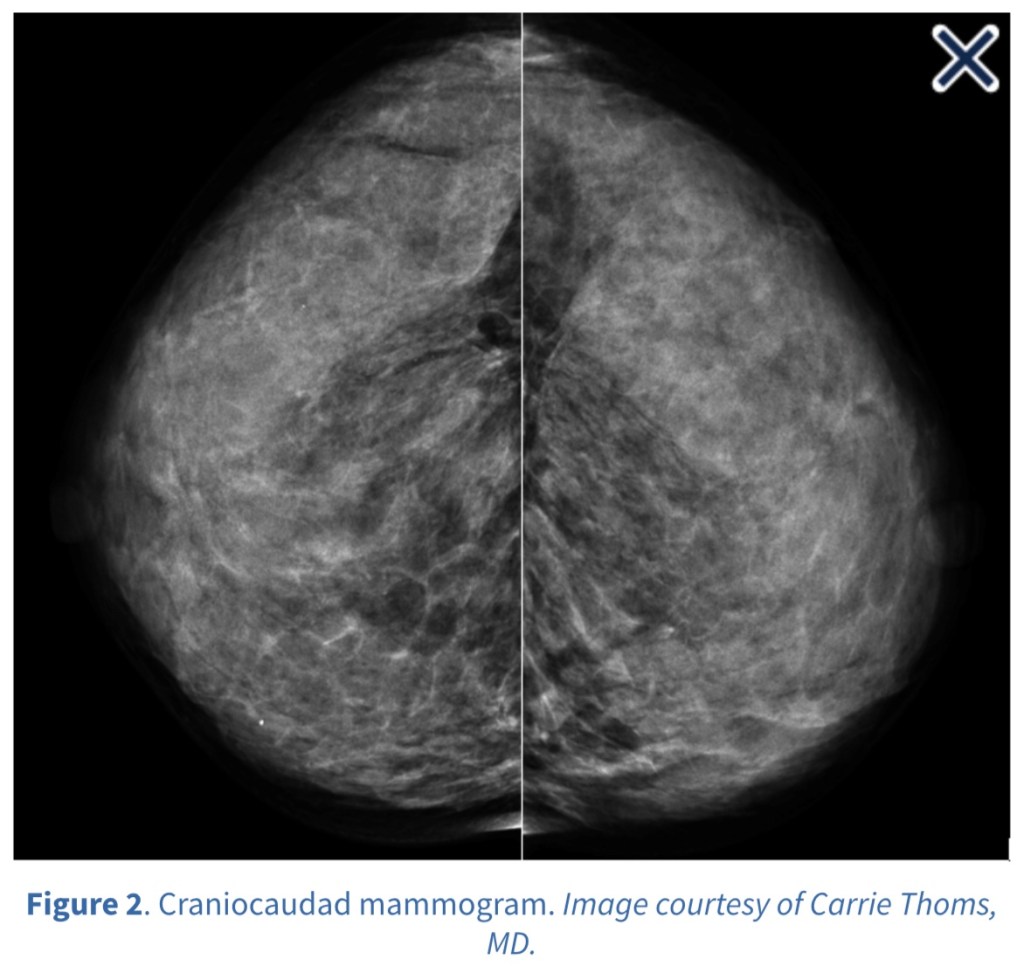
- The most frequent malignant, ductal “casting type” calcifications:
- Are fragmented, linear, and branching:
- They are the most reliable mammographic sign of malignancy (Image)
- The presence of fragmented and / or dotted casting type calcifications on the mammogram:
- Restricted to one lobe:
- Is a pathognomonic sign of a diffuse, grade 3 breast cancer subtype that originates in the major ducts and usually has a solid or micropapillary pattern:
- Traditionally, this subtype has been called “comedo carcinoma”:
- The cancer cells either produce a viscous, proteinaceous fluid which gradually concentrates and eventually calcifies, or they undergo necrosis (apoptosis) followed by calcification
- In both instances, the intraluminal pressure increases, distending the ducts considerably
- Traditionally, this subtype has been called “comedo carcinoma”:
- Is a pathognomonic sign of a diffuse, grade 3 breast cancer subtype that originates in the major ducts and usually has a solid or micropapillary pattern:
- Restricted to one lobe:
- Dotted casting type calcifications:
- Have been referred to as “snakeskin-like calcifications”:
- They accumulate in the fluid:
- Produced by either micropapillary or solid cancer cell growth patterns (Image)
- They accumulate in the fluid:
- Have been referred to as “snakeskin-like calcifications”:
- Are fragmented, linear, and branching:

- The tips of the micropapillary growths may become detached and eventually calcify, contributing to the intraluminal calcifications (Image).

- Occasionally, malignant ductal calcifications present in a manner that can be easily mistaken for a benign process:
- It occurs when fluid production:
- Rather than necrosis, dominates the picture
- The intraductal carcinoma can be grades 1, 2, or 3 and a micropapillary and / or cribriform architecture is present
- Tabár has done extensive work comparing the mammographic images with 3D subgross sections and whole mount histology slides in order to determine that the calcification occurs in large lakes of fluid that calcify, forming round or oval, discoid calcifications:
- He credits Stavros with suggesting the name “skipping stone” calcifications because they are reminiscent of stones that children skip across a pond (Images 5a, 5b, 6, and 7)
- It occurs when fluid production:

- A variation of this type of calcification occurs in grades 1 and 2 fluid-producing intraductal carcinomas when large psammoma body-like calcifications develop in the ducts in a pattern suggestive of a “string of pearls”

#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #BreastCancer #BreastImaging #MountSinaiMedicalCenter #MSMC #Miami #Mexico
 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Maestria en ciencias (Clinical research for healthprofessionals):
• Maestria en ciencias (Clinical research for healthprofessionals): • Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina