- Myth:
- Women with nipple / areolar lesions and nipple piercings should be discouraged from breastfeeding
- Science:
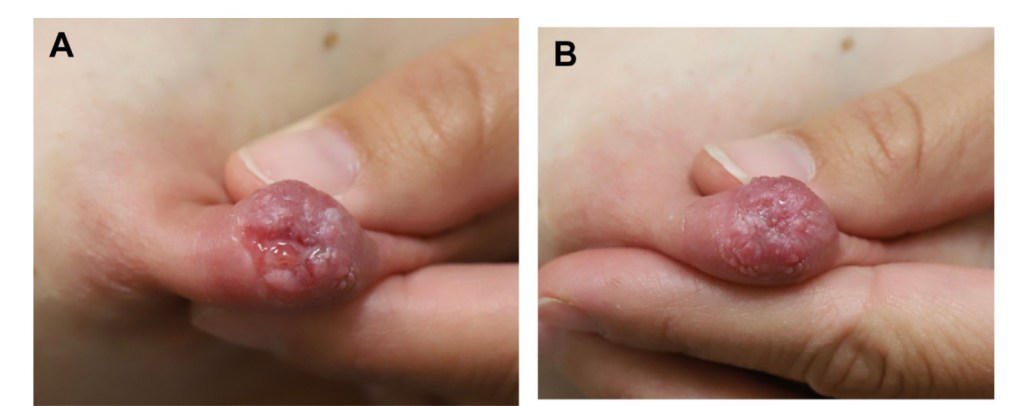
- Several lesions can occur on the nipple / areolar complex including:
- Nipple adenomas
- Skin tags
- Eczema
- Hyperkeratosis
- Patients with these conditions are often advised to avoid breastfeeding:
- Due to concerns about latch and milk extraction, as well as theoretic risks of an infant choking on a protruding lesion or suffering toxicity from medications used to treat dermatologic conditions
- Patients with nipple piercings may be advised to avoid breastfeeding altogether due to concerns about milk fistulae:
- Milk will indeed pass through the piercing sites (Figure):
- However, this does not negatively affect milk production or extraction, nor does it pose a risk to the mother’s health in any way
- Milk will indeed pass through the piercing sites (Figure):
- Several lesions can occur on the nipple / areolar complex including:
- Treatment:
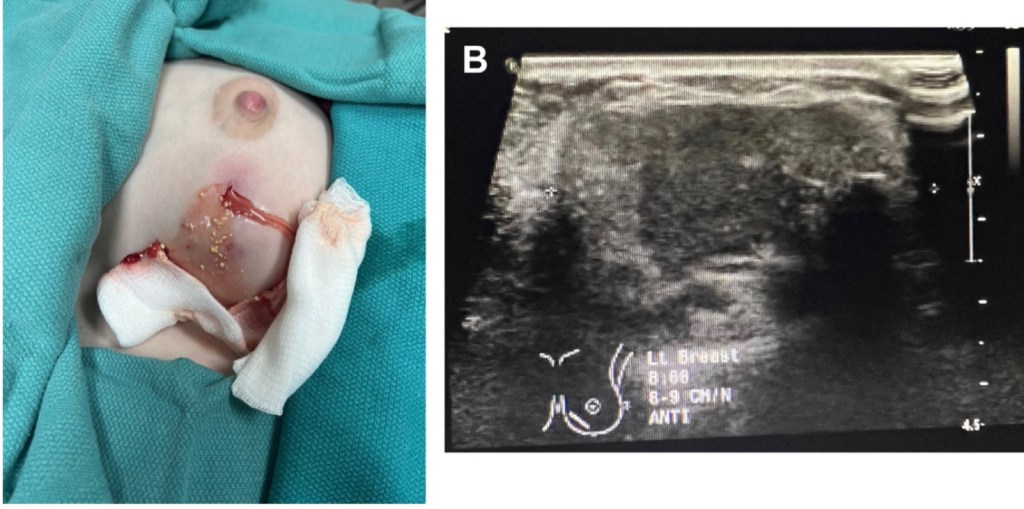
- Women with nipple / areolar lesions should be evaluated by a breastfeeding medicine physician prenatally
- These physicians may recommend removal of larger lesions if they are concerned about interference with latch or potential for tissue trauma
- Surgical excision can be performed under local anesthesia during pregnancy or lactation with minimal risk
- In most of the cases, prenatal evaluation of nipple / areolar lesions will consist of review of the lactational safety of medications and reassurance
- Topical steroids, keratolytic ointments, and most immunomodulators used for conditions such as eczema, psoriasis, and hyperkeratosis are safe in lactation, with the exception of methotrexate
- Nipple shields should not be recommended to cover nipple /areolar complex lesions, as there is no benefit to this practice and nipple shields are associated with decreased physiologic milk transfer and increased risk of microbiome disruption and mastitis
- Ideally, patients should remove nipple piercings during early pregnancy:
- As the nipple is expected to hypertrophy and can make later removal more difficult
- Nipple piercings are a choking hazard, and patients should not breastfeed with them
- When consenting for piercings, women should be counseled that the procedure may result in ductal trauma or scarring that could impair lactation

#Arrangoiz #Doctor #Surgeon #CancerSurgeon #BreastSurgeon #SurgicalOncologist #MountSinaiMedicalCenter #MSMC #Miami #Mexico #BreastCancer #MilkBlebs