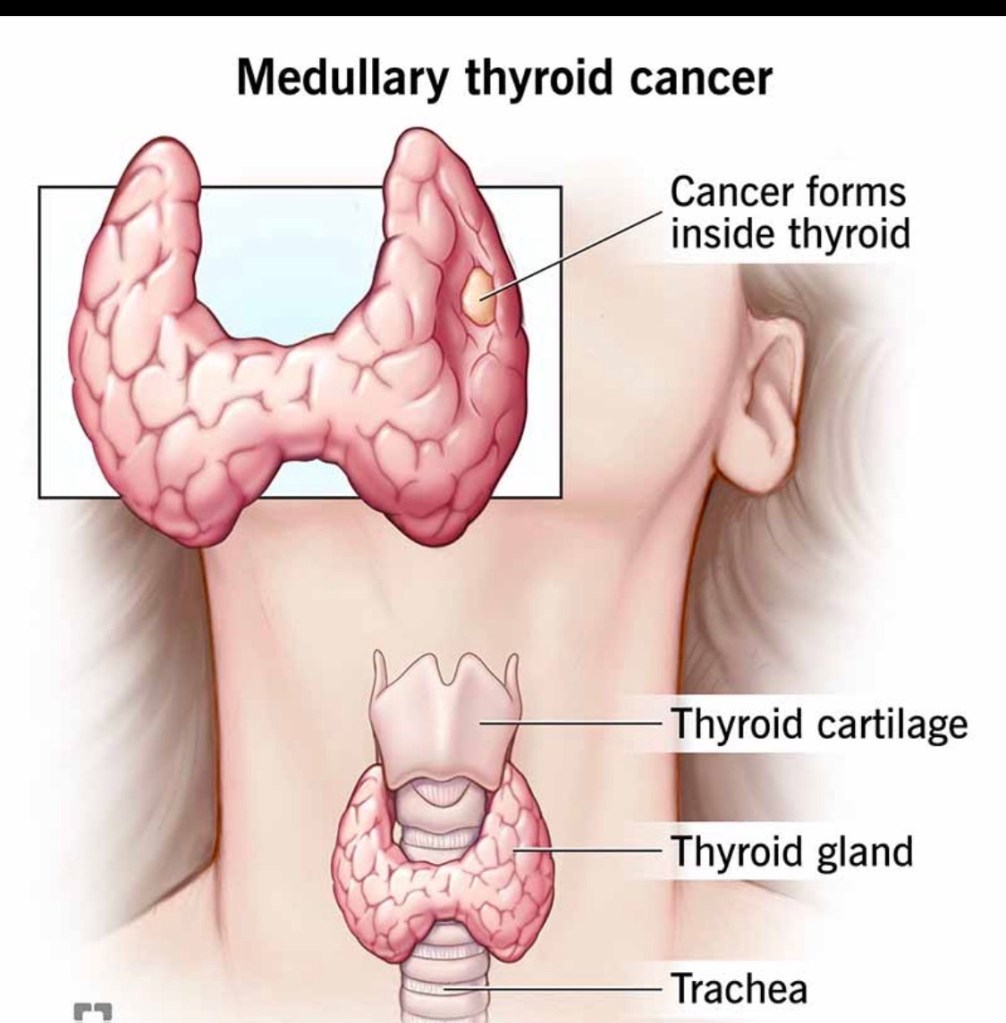
Medullary thyroid cancer (MTC) accounts for ~2–4% of all thyroid cancers and is biologically distinct from papillary and follicular thyroid cancers.
🧠 What makes MTC different?
Arises from parafollicular (C) cells, not follicular cells Produces calcitonin, a key tumor marker Does NOT respond to radioactive iodine Can be sporadic (~75%) or hereditary (~25%)
🧬 The genetic connection
Hereditary MTC is associated with RET mutations Seen in MEN2 syndromes (MEN2A, MEN2B, FMTC) All patients with MTC should undergo genetic testing, regardless of age or family history
🔍 How is MTC diagnosed?
Suspicious thyroid nodule on ultrasound Elevated serum calcitonin (often markedly high) Confirmed by FNA biopsy ± calcitonin washout Imaging to evaluate lymph node involvement
⚖️ How is MTC treated?
The cornerstone of treatment is surgery:
Total thyroidectomy Central neck lymph node dissection Lateral neck dissection when nodes are involved
➡️ Radioactive iodine has no role in MTC.
➡️ Targeted systemic therapies are used in advanced disease.
📈 Prognosis
Highly dependent on stage at diagnosis Early detection → excellent long-term outcomes Lymph node and distant spread worsen prognosis
🦋 Early recognition and expert surgical management are critical.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Medullary thyroid cancer is rare but requires prompt diagnosis, genetic evaluation, and expert surgical care.
📚 References
Wells SA et al. Revised ATA Guidelines for Medullary Thyroid Carcinoma. Thyroid Elisei R et al. Management of Medullary Thyroid Cancer. Lancet NCCN Guidelines: Thyroid Carcinoma
Hürthle cell carcinoma (HCC) is a distinct subtype of differentiated thyroid cancer, accounting for ~3–5% of cases. Although related to follicular tumors, it behaves differently and requires specific management considerations.
🧠 Key characteristics of Hürthle cell carcinoma
Composed of oncocytic (Hürthle) cells rich in mitochondria More common in older patients Less likely to spread to lymph nodes More likely to spread hematogenously (lungs, bone) in higher-risk disease Often less iodine-avid than papillary or follicular thyroid cancer
🔍 How is it diagnosed?
Ultrasound and FNA may suggest a Hürthle cell neoplasm Definitive diagnosis requires surgery, based on: Capsular invasion Vascular invasion
Thyroid lobectomy for small, minimally invasive tumors Total thyroidectomy for larger or invasive disease Radioactive iodine selectively (often less effective than in other subtypes) Close long-term surveillance
📈 Prognosis
Excellent outcomes for minimally invasive disease Prognosis worsens with: Extensive vascular invasion Large tumor size Distant metastases
🦋 Careful pathology review and individualized treatment are essential.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Hürthle cell carcinoma is uncommon but highly treatable when managed by an experienced thyroid team.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Lloyd RV et al. WHO Classification of Tumours of Endocrine Organs Ganly I et al. Hürthle cell carcinoma outcomes. J Clin Endocrinol Metab
Follicular thyroid cancer (FTC) accounts for ~10–15% of thyroid cancers. While less common than papillary thyroid cancer, it is still highly treatable, especially when diagnosed early.
🧠 Key characteristics of FTC
Tends to spread through the bloodstream rather than lymph nodes Can metastasize to lungs or bones (uncommon, usually in higher-risk disease) Often appears similar to benign nodules on ultrasound Diagnosis depends on capsular and/or vascular invasion, which cannot be confirmed by FNA alone
🔍 How is FTC diagnosed?
Ultrasound and FNA may suggest a follicular neoplasm Definitive diagnosis requires surgery and full histologic evaluation Pathology distinguishes: Minimally invasive FTC Widely invasive FTC
⚖️ How is follicular thyroid cancer treated?
Management is risk-adapted and may include:
Thyroid lobectomy for minimally invasive, low-risk tumors Total thyroidectomy for higher-risk disease Radioactive iodine selectively for tumors with vascular invasion or metastases Long-term surveillance with thyroglobulin and imaging
📈 Prognosis
Excellent outcomes for minimally invasive FTC Prognosis depends on: Degree of vascular invasion Tumor size Patient age
🦋 Early, appropriate management leads to very high cure rates.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Follicular thyroid cancer often requires surgery for diagnosis, but when managed correctly, outcomes are excellent.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Lloyd RV et al. WHO Classification of Tumours of Endocrine Organs. Tuttle RM et al. Risk-adapted management of differentiated thyroid cancer. Lancet Diabetes Endocrinol
Papillary thyroid cancer (PTC) accounts for ~80–85% of all thyroid cancers. It is also the subtype with the best overall prognosis.
🧠 Key characteristics of PTC
Typically slow-growing Often diagnosed at an early stage May spread to neck lymph nodes, especially in younger patients Even with lymph node involvement, long-term survival remains excellent
🔍 How is PTC usually detected?
Incidentally on high-resolution ultrasound Confirmed with ultrasound-guided FNA biopsy Often small tumors (≤2 cm) at diagnosis
⚖️ How is papillary thyroid cancer treated?
Treatment is risk-adapted and may include:
Active surveillance for selected very low-risk tumors Thyroid lobectomy for low-risk disease Total thyroidectomy for higher-risk cases Selective lymph node surgery when indicated Radioactive iodine only for patients who truly benefit
➡️ Not all patients need the same treatment.
📈 Prognosis
10-year survival >95% Many patients live normal lifespans Focus is increasingly on quality of life, not just cure
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Papillary thyroid cancer is common, highly treatable, and often requires less aggressive treatment than patients expect.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Tuttle RM et al. Risk-adapted management of papillary thyroid cancer. Lancet Diabetes Endocrinol SEER Cancer Statistics Review
Radioactive Iodine (RAI) for Thyroid Cancer – Who Really Needs It in 2026?
Radioactive iodine (RAI, I-131) is used after thyroid surgery in selected cases of differentiated thyroid cancer (papillary and follicular). Its goals are:
to destroy tiny remnants of thyroid tissue (“remnant ablation”), to reduce the risk of recurrence (“adjuvant therapy”), or to treat known persistent or metastatic disease.
Over the last decade, we’ve learned that many low-risk patients do just as well without RAI, so we now use it much more selectively.
1. When is RAI usually recommended?
Most societies (ATA, ETA, NCCN, SNMMI/EANM) and recent data support using RAI mainly for intermediate- and high-risk disease.
RAI is typically recommended when:
High-risk disease (ATA high risk) Gross extrathyroidal extension Large primary tumors Extensive nodal disease (multiple or large metastatic nodes) Distant metastases (lung, bone, etc.) Selected intermediate-risk disease Microscopic extrathyroidal extension Multiple involved lymph nodes Aggressive histologic variants Here, RAI is considered and individualized based on age, tumor biology, thyroglobulin, and patient preferences. Persistent or recurrent disease Elevated or rising thyroglobulin after surgery Iodine-avid metastatic disease on imaging
2. When is RAI often not needed?
For many patients with true low-risk differentiated thyroid cancer, excellent outcomes can be achieved with surgery and careful follow-up without RAI.
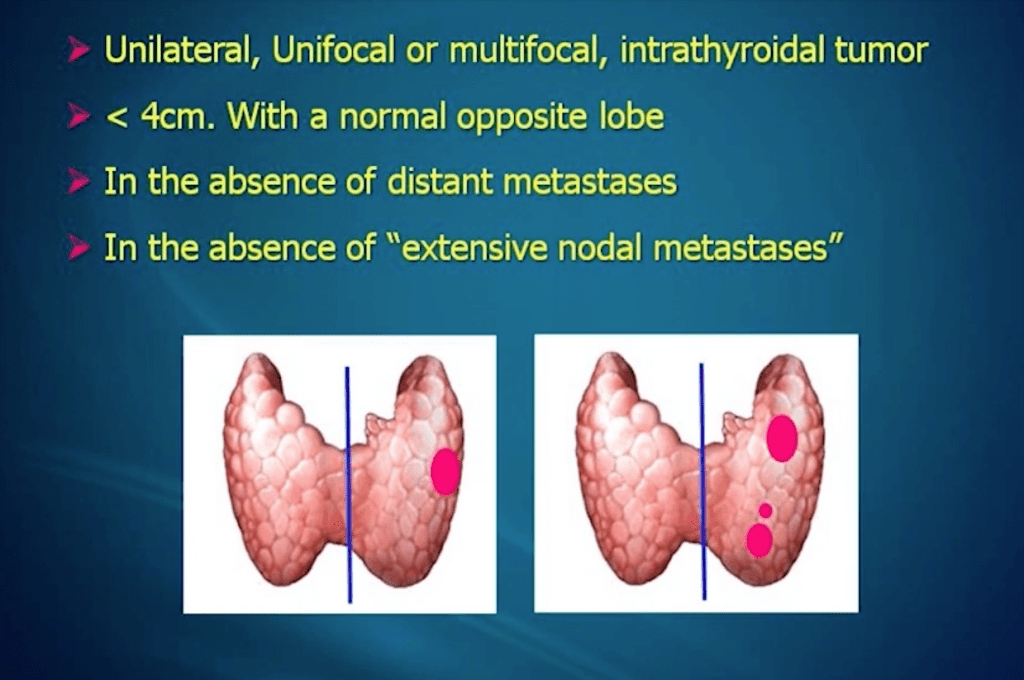
The ESTIMABL2 randomized trial showed that in low-risk patients (small, node-negative tumors), follow-up without RAI was non-inferior to routine RAI at 5 years, with no loss of oncologic opportunity. The 2015 ATA guidelines and subsequent analyses recommend that RAI is not routinely used in ATA low-risk patients, particularly for tumors ≤4 cm without worrisome features.
For many patients, this means less treatment, fewer side effects, and the same excellent prognosis.
3. Common short-term side effects
Most side effects are mild and temporary:
Neck discomfort or swelling Nausea, metallic taste, or loss of taste Dry mouth or thick saliva Swollen, tender salivary glands (parotid/submandibular sialadenitis) Fatigue for days to weeks Temporary changes in blood counts (mild bone-marrow suppression)
Some patients also report:
Dry eyes, tearing problems, or a “gritty” sensation Nasal dryness and crusting
4. Less common or long-term risks
These are less frequent but important to discuss before treatment:
Chronic salivary gland dysfunction Persistent dry mouth (xerostomia) Difficulty with chewing/swallowing dry foods Increased dental caries and oral infections Lacrimal (tear duct) problems Nasolacrimal duct obstruction → watery or irritated eyes Sometimes requires ophthalmology intervention Fertility and pregnancy Transient effects on sperm parameters and ovarian reserve have been described at higher cumulative doses, so we usually recommend avoiding pregnancy for 6–12 months after RAI and consider sperm banking in selected young men likely to need repeated high-dose treatments. Second primary malignancies (very rare) Large observational studies suggest a small increase in risk of secondary malignancies (e.g., leukemia, salivary gland tumors) at higher cumulative doses, which reinforces the move toward lower doses and more selective use.
5. How we minimize and manage side effects
a) Use the lowest effective dose
Trials such as HiLo and related studies have shown that low-dose (≈30 mCi) RAI with recombinant TSH is as effective as higher doses for remnant ablation in low-risk patients, with fewer side effects.
b) Protect salivary glands
Aggressive hydration for several days after therapy Frequent chewing (sugar-free gum) and sour candies starting after the first 24 hours, as guided by the treating team, to stimulate saliva flow Good oral and dental hygiene, with dental follow-up for patients receiving higher doses In selected patients with significant chronic symptoms, sialogogues (pilocarpine, cevimeline) and targeted ENT/salivary management may help
c) Protect eyes and tear ducts
Artificial tears and ocular lubricants from the early post-treatment period Early evaluation by ophthalmology if tearing, pain, or recurrent eye infections develop In selected complex cases, interventional approaches to the nasolacrimal duct can be considered.
d) Monitor blood counts and overall health
Baseline and follow-up blood counts in patients receiving moderate/high doses Correct nutritional deficiencies and manage anemia or other cytopenias if they occur
e) Clear radiation-safety instructions
Temporary restrictions on close contact with children and pregnant women, sleeping in the same bed, and travel, adapted to the administered dose and national regulations.
6. Take-home messages for patients
Not everyone with thyroid cancer needs RAI. Many low-risk patients do very well with surgery and surveillance alone. When indicated, RAI can reduce recurrence and treat iodine-avid metastatic disease, particularly in higher-risk patients. Most side effects are short-term and manageable; long-term complications are less common and are more likely with higher cumulative doses. Careful risk stratification, dose selection, and prevention strategies (hydration, salivary and ocular care, blood count monitoring) are key to minimizing toxicity. Decisions about RAI should be personalized, ideally made in a multidisciplinary team with a thyroid surgeon, endocrinologist, and nuclear medicine specialist.
Suggested references (for the post footer)
Haugen BR, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016. Pacini F, et al. What are the indications for post-surgical radioiodine therapy in differentiated thyroid cancer? Eur Thyroid J. 2022. Leboulleux S, et al. Thyroidectomy without radioiodine in patients with low-risk thyroid cancer (ESTIMABL2, 5-year follow-up). Lancet Diabetes Endocrinol. 2025. Mallick U, et al. Ablation with low-dose radioiodine and thyrotropin alfa. N Engl J Med. 2012. (HiLo trial) Nguyen NC, et al. Radioactive Iodine Therapy in Differentiated Thyroid Cancer: An Update on Dose Recommendations and Risk of Secondary Primary Malignancies. Semin Nucl Med. 2024. Orosco RK, et al. Radioactive iodine in differentiated thyroid cancer. Head Neck. 2019. Jeong SY, et al. Salivary gland function 5 years after radioactive iodine ablation. J Nucl Med. 2013. Solans R, et al. Salivary and lacrimal gland dysfunction after radioiodine therapy. J Nucl Med. 2001. Baudin C, et al. Dysfunction of the salivary and lacrimal glands after radioiodine therapy: START study. Thyroid. 2023. Rahmanipour E, et al. Eye-related adverse events after I-131 radioiodine therapy: systematic review. Endocr Pract. 2024. Berta DM, et al. Effect of radioactive iodine therapy on hematological parameters: systematic review and meta-analysis. Front Endocrinol. 2025.
Why Not All Thyroid Cancers Need Aggressive Treatment
Not all thyroid cancers behave the same. Modern care is personalized—the goal is to treat what matters while avoiding unnecessary treatment.
🧠 The key concept: Risk-adapted management
Many thyroid cancers—especially low-risk papillary thyroid cancers—are:
Slow-growing Unlikely to spread Associated with excellent long-term survival
Because of this, more treatment is not always better.
⚖️ Treatment options today
Depending on risk, options may include:
Active surveillance (careful ultrasound follow-up, no immediate surgery) Thyroid lobectomy instead of total thyroidectomy Selective use of radioactive iodine (not routine for everyone)
➡️ These approaches are evidence-based and safe for appropriately selected patients.
📉 Why avoid overtreatment?
Unnecessary aggressive treatment can:
Increase risk of hypocalcemia and voice changes Require lifelong thyroid hormone replacement Affect quality of life without improving outcomes
🦋 What matters most
Treatment decisions should be guided by:
✔️ Tumor size and ultrasound features
✔️ Pathology and risk of recurrence
✔️ Patient age, preferences, and values
✔️ Expertise of a multidisciplinary thyroid team
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
The best thyroid cancer treatment is the right treatment for the right patient—not the most aggressive one.
📚 References
Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Tuttle RM et al. Active surveillance for low-risk papillary thyroid cancer. JAMA Brito JP et al. Overdiagnosis and overtreatment of thyroid cancer. BMJ
Mucinous carcinoma of the breast (also known as colloid carcinoma) is a special type of breast cancer:
Presenting with a large amount of extracellular mucin:
That is associated with a relatively favorable prognosis
These tumors are uncommon:
In most series account for approximately 1% to 2% of all invasive breast carcinomas of the breast
It is divided into two main subtypes based upon the quantification of cellularity:
The pure type:
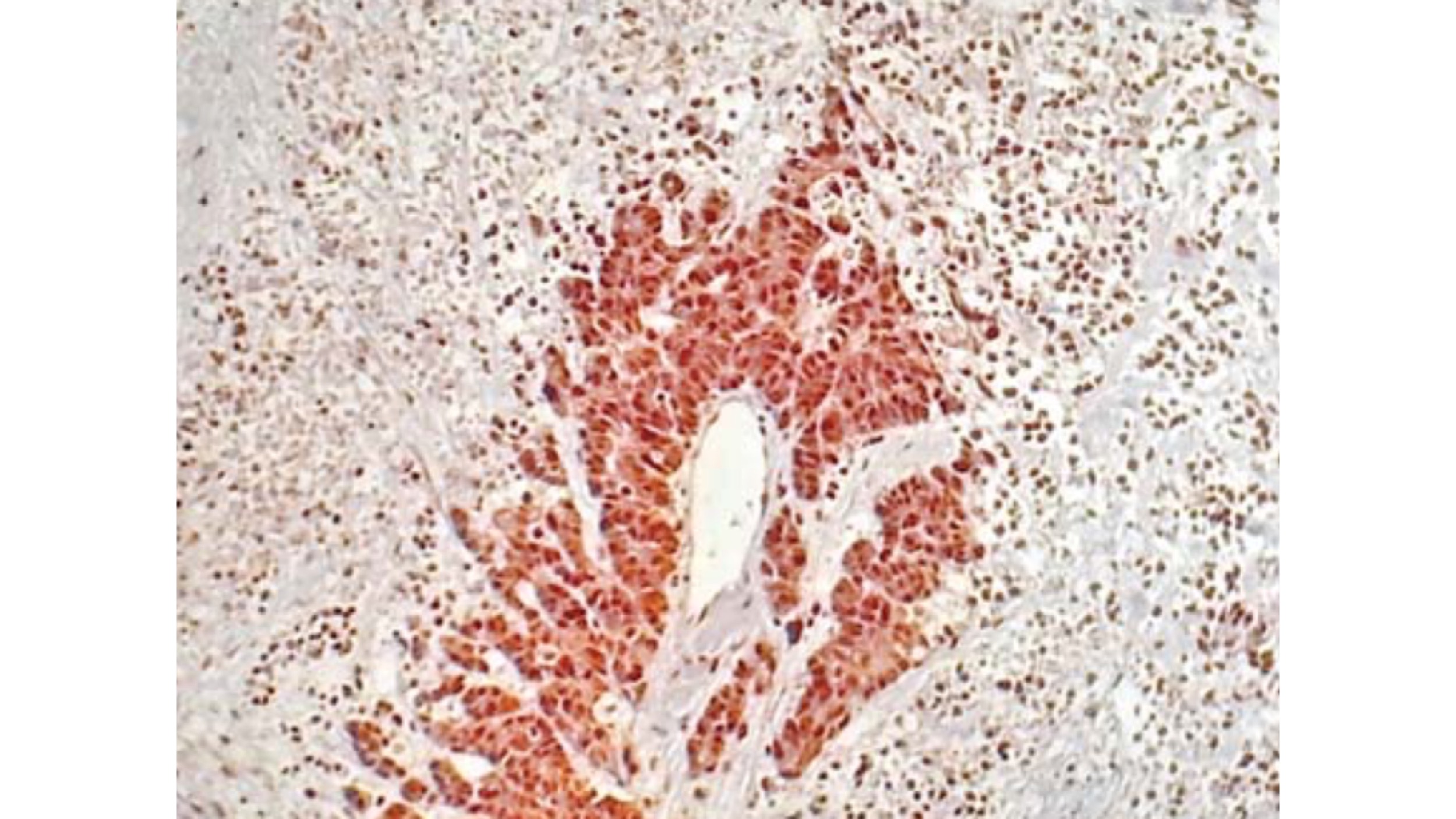
In pure mucinous carcinomas:
Over 90% of the tumor is made up of malignant cell clusters floating in pools of mucin (see images)
Frequently, pure mucinous carcinomas can have posterior enhancement by ultrasound imaging:
That can lead to mistaking these lesions for cysts
Patients with pure mucinous carcinomas:
Tend to be postmenopausal:
Between the ages of 59 and 71 years:
But it can occasionally occur in patients who are younger than age 40 years:
The incidence of mucinous breast cancer in women under 35 years of age is less than 1%
The mixed type:
Tumors in which 50% to 90% of the mass is composed of malignant cell clusters floating in mucin are considered to be a mixed NOS and mucinous category:
Mixed mucinous carcinomas show a less distinct margin, a higher grade, and more mitotically active cytology
Their clinicopathologic features:
Are similar to those of invasive ductal carcinoma, NOS type
Some mucinous breast carcinomas (mainly mixed type) are associated with lobular or ductal neoplasia (in situ or invasive) and some have neuroendocrine differentiation:
Mucinous breast carcinomaassociated with lobular neoplasiacomponents:
Seems to be a biologically distinct subset that frequently shows decreased cell to cell adhesion, loss of cell polarity molecules and lack of neuroendocrine differentiation:
Also in this subset of tumors, the neoplastic cells with signet-ring features are most likely to be found
Mucinous breast cancer is a slow-growing neoplasm:
With an estimated growth rate of one third of invasive breast cancer no special type
This malignancy also shows:
Fewer axillary lymph node metastases
Conventional, pure mucinous carcinomas:
Exhibit a rate of metastasis of less than 15%
Current studies have shown that a subset of patients diagnosed with mucinous carcinoma:
Do not manifest such favorable outcomes:
Some authors suggested that specific subtypes of pure mucinous carcinoma:
Those with a micropapillary pattern demonstrate significantly worse prognosis:
In one study more than half of the patients with this particular type of pattern were found to have vascular invasion and synchronous axillary lymph nodes
A subset of mucinous breast carcinomas shows neuroendocrine differentiation:
Defined by cytoplasmic argyrophilia or immunoreactivity to markers such as:
Synaptophysin
Chromogranin
Neuronal specific enolase
Although in one study neuroendocrine differentiation:
Was associated with a favorable histology and a good outcome others did not find this association
Rodrigo Arrangoiz MS, MD, FACS a surgical oncologist and is a member of Mount Sinai Medical Center in Miami:
He is an expert in the management of breast cancer:
If you have any questions about breast cancer statistics please fill free to ask Dr. Arrangoiz
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
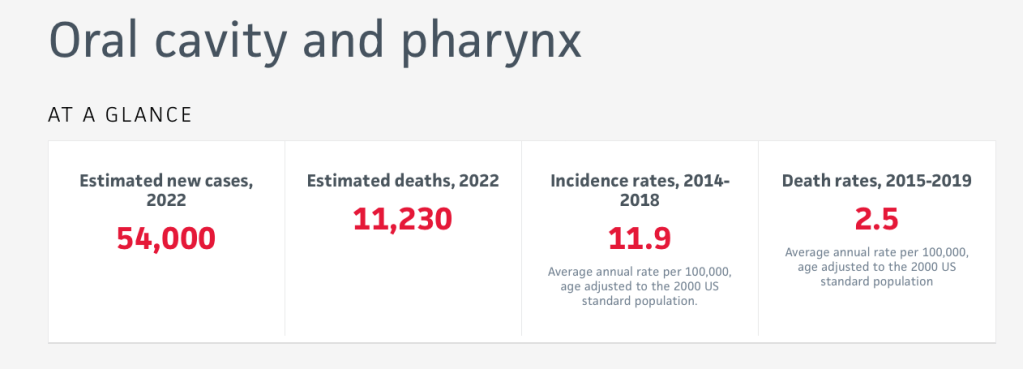
Ranks as the 13th most common cancer in the world and 7th most frequent in males
There is not only a marked variation in the incidence and mortality from oral cancer between various countries:
But also between ethnic groups and regions of one country:
This is primarily attributable to variations in the prevalence of major risk factors between populations:
However, other dietary and genetic influences may also contribute
The lower gingivobuccal complex:
Is comprised of buccal mucosa, gingivobuccal sulcus, inferior alveolar ridge, lower gingiva and retromolar trigone
It is the most common site for oral cancer in the Indian subcontinent due:
To the habit of chewing tobacco
The goal of evaluating a patient with gingivobuccal complex cancer:
Is to assess the extent of disease and to define the tumor type histologically
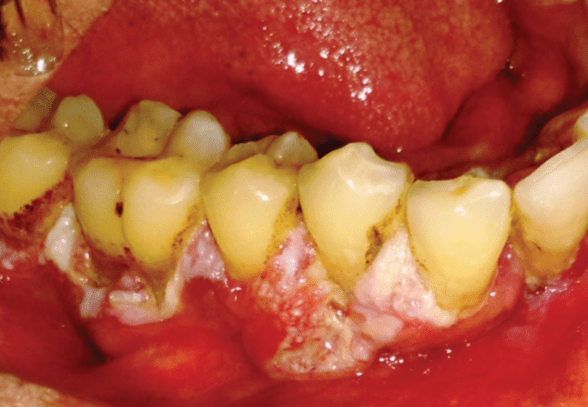
Patients usually present with:
A persistent ulcer or an exophytic growth in the gingivobuccal complex
Loosening of teeth
Ill-fitting denture
Trismus
Pain:
Is a late feature
Patients with advanced disease present with:
Orocutaneous fistula
Severe trismus
Lymph node metastasis
Many patients have associated premalignant lesions like:
Leukoplakia and erythroplakia or premalignant condition like submucous fibrosis
An asymptomatic lesion, with a history of tobacco and / or alcohol consumption:
Should raise suspicion of oral cancer and biopsy should be done
Examination assesses the extent of involvement of important structures such as:
Mandible, floor of the mouth musculature and cervical nodes
The presence of trismus:
May suggest deep invasion
It is important to determine whether this trismus is due to:
Associated submucous fibrosis or malignant disease
The clinician should evaluate any medical and nutritional problems
Common problems in patients with cancer of the oral cavity are:
Hepatic disease, pulmonary disease and malnutrition
Knowledge of the mode of spread of gingivobuccal complex cancer:
Is important for developing a rational therapeutic approach
Local spread to adjacent structures:
May lead to invasion of the underlying soft tissue, muscles, bone and neurovascular structures
Gingivobuccal complex cancer extends:
Along surface mucosa and the submucosal soft tissue:
To approach the buccal or labial gingiva
From this point onwards:
The tumour does not extend directly through the intact periosteum and cortical bone towards the cancellous part:
Because the periosteum acts as a significant protective barrier
Instead:
The tumor advances along the attached gingiva towards the alveolus
Subsequently:
The mandible is involved by infiltration through the dental sockets or the dental pores (in edentulous patients) on the alveolar ridge:
These cells proceed along the root of the tooth into the cancellous part of the mandible and then along the mandibular canal:
This understanding has led to the development of mandible-sparing, surgical resections
Cervical lymph nodes:
Are the most commonly involved metastatic site
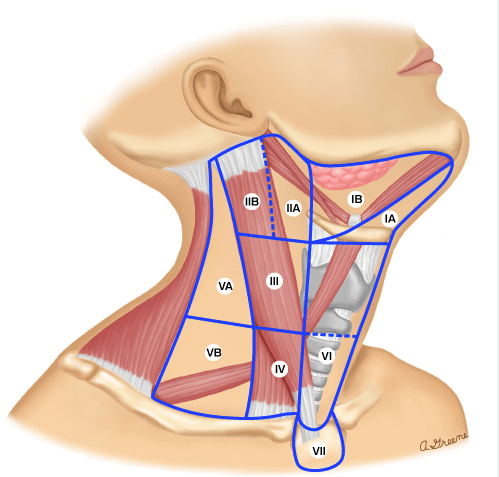
The neck has been divided into five nodal levels:
For planning treatment of gingivobuccal complex cancer
The gingivobuccal complex has a predictable lymphatic drainage:
The first echelon lymph nodes are in the:
Supraomohyoid triangle of neck:
Levels I, II, III
Spread to lymph nodes in posterior triangle:
In the absence of metastasis at other levels:
Is rare
Skip metastasis from gingivobuccal complex carcinomas:
Are rare
Distant metastasis at the time of initial diagnosis is exceedingly rare:
When it does occur it is to lung and bones
Biopsy of the lesion is mandatory before treatment:
Often, this can be done under local anaesthesia
The biopsy should be deep and encompass a portion of the tumour as well as adjacent normal appearing mucosa
Superficial biopsies are inconclusive and yield negative results
In suspected verrucous carcinomas:
Where the basement membrane is intact:
A deep biopsy is mandatory to reach a diagnosis
Imaging work-up depends on the extent of the disease:
Patients with early lesions do not need an extensive evaluation:
An orthopantomogram or oblique radiograph of the mandible is a cost-effective initial investigation to assess mandibular involvement
The accuracy of clinical examination, peroperative periosteal stripping and imaging techniques have been compared:
Clinical examination alone was not shown to be accurate:
But periosteal stripping at the time of resection was extremely accurate
No single imaging technique will accurately predict mandibular invasion:
However, a combination of orthopantomogram and bone scintigraphy is recommended in early invasion
Magnetic resonance imaging (MRI) is more sensitive than computerised tomography (CT) for mandibular invasion
CT scanning gives additional information regarding the extent of mandibular involvement, malignant infiltration and cervical nodal disease
MRI can be used to determine soft tissue and perineural involvement
However, all patients do not need CT scan or MRI:
These are especially indicated in patients with large lesions having trismus and lesions abutting the mandible where marginal mandibulectomy is being planned
It is also used to evaluate patients with a clinically negative neck or those with large nodes for presence of carotid involvement
Ultrasound guided fine needle aspiration cytology (FNAC) has the highest accuracy in diagnosing cervical nodal metastasis in the clinically negative neck compared to ultrasonography, CT scan and MRI:
However, none of the imaging methods can determine occult metastatic nodal disease
In view of the risk of multifocal changes:
Endoscopic evaluation (panendoscopy) of the upper aerodigestive tract is recommended to evaluate the presence of second primaries:
Direct laryngoscopy, bronchoscopy, esophagoscopy and examination under general anesthesia may be done for accurate assessment of the disease and the upper aerodigestive tract
Depending on the specific site in the gingivobuccal complex (alveolus, gingivobuccal sulcus or buccal mucosa alone):
The extent of the primary tumor and the status of lymph nodes:
The treatment of these cancers may be by surgery or radiation therapy used alone or in combination, with or without chemotherapy
Early lesions (T1, T2) can be effectively treated with either surgery or radiation as a single modality:
Certain factors influence this decision:
For example, in the presence of associated submucous fibrosis:
Surgery is preferable to radiation therapy
Lesions located in lower gingivobuccal sulcus or involving mandible are usually not treated with radiation:
Because of proximity to bone and chances of osteo-radionecrosis
Advanced lesions require a combined modality treatment
Treatment of gingivobuccal complex cancer:
Is primarily surgical:
The aim of surgical treatment is to excise the entire primary lesion with clear margins (1 cm to 2 cm) three-dimensionally, and also effectively treat the regional lymph nodes
This ablative surgery is followed by primary reconstruction:
To provide rapid healing, restore function and appearance and thereby improve patient’s quality of life
These lesions are resected either by an upper or lower cheek flap with a lip split, visor flap or per-orally:
Depending upon the size and location of the primary
These cancers often abut or involve the mandible
Most of these cancers are not amenable to per-oral resection:
Owing to inadequate access:
Which may jeopardise the oncological resection
Per-oral resection is possible in:
Small lesions (usually, 2 cm or less), situated anteriorly, with no or minimal mandibular involvement, and with good mouth opening
Radical ablative surgery is followed by reconstructive surgery:
Surgical defects may be reconstructed by primary closure, skin graft, locoregional flaps or free tissue transfer from different sites
The decision to resect the mandible as part of the management of oral cancer:
Should be taken on the evidence of clinical examination, periosteal stripping and at least two imaging techniques that complement each other in terms of specificity and sensitivity
Lesions that directly invade the bone:
Should undergo a segmental or hemi-mandibulectomy
Resection of the posterior part of the body or ramus of mandible leaves very little aesthetic deformity, but there is always functional compromise with segmental resection of any part of mandible
Resection of anterior arch of mandible:
Results in significant functional and cosmetic deformity and immediate reconstruction should be done by an osteomyocutaneous flap or composite free tissue transfer
If immediate reconstruction is not feasible or desirable, the mandibular stirrups should be immobilised by internal, external or interdental fixation
Heavy reconstruction plates may also be used in this situation
Mandibular sparing techniques like marginal mandibulectomy have gained popularity for lesions with no, or minimal, cortical mandibular invasion:
Marginal mandibulectomy has been used for along time in cancer of the floor of the mouth and can also be used for cancers of gingivobuccal complex
Mandibular continuity is maintained and a much better cosmetic and functional end result is achieved with marginal mandibulectomy:
At least, a 1-cm thick segment of bone must be left inferiorily after a marginal mandibulectomy
Marginal mandibulectomy is contraindicated in patients with:
Gross clinical and radiological involvement of mandible
Invasion of mandibular canal by cancer
In deeply infiltrating lesions of gingivobuccal sulcus where there is paramandibular infiltration:
As the margin of resection may pass through infiltrated paramandibular tissue
It is also contraindicated in previously irradiated mandible
Reduced vertical height of the bone in an edentulous mandible is a relative contraindication for marginal mandibulectomy
Marginal mandibulectomy is also usually not done in lesions of the retromolar trigone as clearance of pterygoid region is possible only if ascending ramus of the mandible is resected:
However, some studies have also reported satisfactory results of marginal mandibulectomy in lesions of the retromolar trigone
Results of marginal mandibulectomy for gingivobuccal complex carcinoma show an:
Overall local recurrence-free survival rate of 79% and 70% at 2 and 5 years, respectively
Other studies have also demonstrated the oncological safety of marginal mandibulectomy in carefully selected patients with oral cancers
The management of neck for gingivobuccal complex cancers:
Depends on whether the neck is clinically node-negative or node-positive
In patients with clinically positive lymph nodes (N1, N2, N3):
Radical neck dissection (RND) has been the gold standard
However, there is mounting evidence that RND should not be the only therapeutic option for the clinically positive neck:
In patients with clinical N1 disease and selected N2 disease:
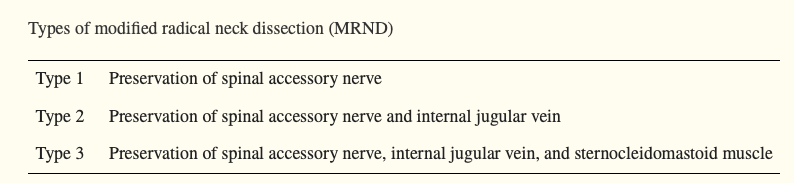
A modified radical neck dissection may be done for better cosmetic and functional results
Preservation of the spinal accessory nerve, internal jugular vein (IJV) and sternocleidomastoid muscle:
Is done in the form of a modified radial neck dissection (MRND)
RND, however, is still appropriate for patients with:
Massive lymphadenopathy (N3 disease)
Multiple positive nodes involving the spinal accessory nerve and / or the IJV
Residual or recurrent neck disease after radiotherapy
Gross extranodal spread
A supraomohyoid neck dissection (SOHND):
Clearance of level I, II and III nodes plus postoperative radiation therapy has been advocated by a few authors for N1, level I disease:
There are still no prospective, randomised trials comparing SOHND with RND / MRND in clinically positive neck and it is unlikely that studies large enough to answer this question will be carried out in the future
Nodal spread can occur to both sides of neck:
Especially in lesions:
Close to mid-line
In patients with bilateral nodal metastasis:
A bilateral neck dissection with preservation of IJV on at least one side (the less affected side) is indicated:
An alternative to this is to do a staged RND:
The IJV resection is done on both the sides with an interval of 4 weeks between them
Occult nodal metastatic disease:
Is present in 5% to 26% of gingivobuccal complex cancers:
Depending on the T-status and grade
Management of the clinically negative is thus an important issue:
Patients with T1 / T2 cancers (low risk, less than 20% risk of nodal metastasis):
Do not require elective neck treatment
SOHND should be performed in patients with:
T3 / T4 primary (high risk, greater than 20% risk of nodal metastasis)
If entering the neck to resect the primary
Short-necked individuals:
Who require a bulky flap for oral reconstruction:
To create space in neck
Patients who are unreliable for follow-up
Patients who are found to have pathologically positive neck nodes after SOHND:
Should receive additional treatment
If detected positive intra-operatively (on frozen section):
Then SOHND should be changed to RND or MRND
Patients with positive lymph nodes, diagnosed on histopathology following SOHND:
Should either undergo RND / MRND or postoperative radiotherapy
Patients with a single positive, level I node only, without extra-capsular spread:
May not need additional treatment
A randomized trial comparing SOHND with comprehensive neck dissection in patients with clinically negative nodes:
Found no difference in the regional control and overall survival rates between the two groups:
However, SOHND alone is inadequate treatment for patients with pathologically confirmed or clinically positive nodes
Patients undergoing MRND need adjuvant radiation therapy to the neck if N2 disease is present:
Adjuvant radiation provides good regional control
The role of ultrasound-guided FNAC of the N0 neck in the decision for elective neck dissection has been reported:
However, its application to gingivobuccal complex cancers in particular is uncertain
Recently, lymphatic mapping with sentinel lymph node biopsy has been used in N0 oral cancer patients but further refinement of technique and larger studies are needed before this can be recommended as standard treatment
Radiation therapy and surgery:
Have equal success in controlling early lesions of the oral cavity
Radiation is given either as:
External beam, brachytherapy or acombination of both
For gingivobuccal complex cancers:
Radiotherapy is usually not the preferred modality of treatment for early cancers (T1, T2):
Due to the close proximity of the tumor to bone and risk of radionecrosis
Radiotherapy is used for treatment of early lesions of buccal mucosa and gingivobuccal sulcus:
Where the patient is not medically fit or is unwilling for surgery
It is also used as an adjuvant treatment for the primary tumor in patients with histologically positive margins on resection:
And has been shown to decrease the local recurrence rate
In patients with advanced lesions (T3, T4):
A combination of surgery and radiation therapy provides a better chance of cure than either modality alone
The 3-year survival for stages III and IV disease treated with radiation therapy or surgery alone:
Is 41% and 15%, respectively
These rates increase to 60% and 35%, respectively:
When surgery is combined with postoperative radiation therapy
In a randomized trial, Mishra et al:
Have reported a significant improvement in disease-free survival in patients with T3 / T4 carcinoma of the buccal mucosa
Postoperative radiation therapy is indicated in all patients with:
T3 primary tumors
T4 primary tumors
Patients with positive or close surgical margins
Pathologically positive lymph nodes after SOHND
Two or more positive lymph nodes after RND / MRND
Lymph nodes showing extracapsular spread
There is evidence for the use of adjuvant concurrent chemoradiotherapy:
In patients of head and neck cancers with poor prognostic factors
Definitive radiation or concurrent chemoradiotherapy:
Is used in advanced (stage III / IV) disease, if the disease is inoperable or the patient is unfit or unwilling for surgery
Concurrent chemoradiotherapy:
Has evolved as the standard of care for such locally advanced head and neck cancers
The toxicity of concurrent chemoradiotherapy is more than radiation therapy alone and requires aggressive supportive measures:
However, evidence for use of concurrent chemoradiotherapy for oral cavity subsite is sparse
In clinically node-negative neck cancer, elective neck irradiation is done if the primary is being treated with radiation therapy
Age plays an important role in how thyroid cancer behaves, how it is staged, and how it is treated.
👶 Thyroid cancer in younger patients
More common in women Often presents with lymph node involvement Tumors may look aggressive on imaging 👉 Despite this, prognosis is excellent
✔️ Patients under 55 years are staged differently
✔️ Even with lymph nodes, survival rates exceed 98–99%
✔️ Treatment focuses on curing disease while preserving quality of life
👴 Thyroid cancer in older patients
Less common, but tumors may be biologically more aggressive Higher likelihood of: Extrathyroidal extension Distant metastases Higher-stage disease Outcomes are still often very good, but treatment may need to be more comprehensive
⚖️ Why age matters
Age helps determine:
AJCC stage Expected prognosis Intensity of treatment and follow-up
🧠 Important clarification:
Age alone does not determine outcome.
➡️ Tumor biology, pathology, and response to treatment matter most.
🦋 What this means for patients
Thyroid cancer is not the same disease in every patient.
The goal is personalized, risk-adapted care—not one-size-fits-all treatment.
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
Mount Sinai Medical Center
📌 Take-home message:
Young patients do extremely well.
Older patients still have excellent outcomes with expert, individualized care.
📚 References
AJCC Cancer Staging Manual, 8th Edition Haugen BR et al. ATA Guidelines for Differentiated Thyroid Cancer. Thyroid Tuttle RM et al. Risk-adapted management of thyroid cancer. Lancet Diabetes Endocrinol
Updated 2018 American Society for Radiation Oncology (ASTRO) guidelines:
State that patients 50 and younger, and 51 to 70 years of age with high-grade tumors or positive margins:
Should receive a tumor bed boost
A boost may be omitted for women:
Older than 70 with hormone receptor positive and low- or intermediate-grade disease with widely negative margins (> 2 mm)
If the patient does not meet either of those criteria, individualized decision making is recommended
For ductal carcinoma in situ (DCIS):
Tumor bed boost may be used for women:
50 years of age and younger
Close (less than 2 mm) or positive margins
High-grade disease
It may be omitted for patients:
Older than 50 with screening detected
Total size less than 2.5 cm
Low to intermediate nuclear grade
Widely negative margins:
Greater than 3 mm
Long-term 20-year follow-up of a phase 3 trial of boost vs. no boost:
Reported a benefit in all groups with the largest absolute risk reduction in younger patients
References
Smith BD, Bellon JR, Blitzblau R, et al. Radiation therapy for the whole breast: executive summary of an American Society for Radiation Oncology (ASTRO) evidence-based guideline. Pract Radiat Oncol. 2018;8(3):145-152.
Bartelink H, Maingon P, Poortmans P, et al. Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. Lanc Oncol. 2015;16(1):47-56.