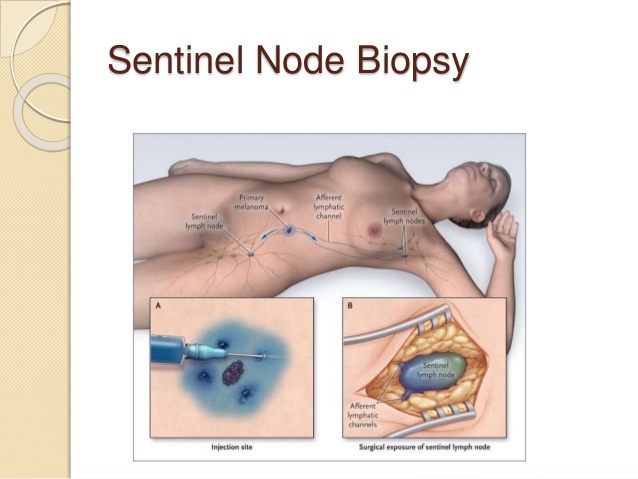
👉 The rationale for performing sentinel lymph node biopsy (SLNB) is to have nodal staging in the event invasive carcinoma is identified pathologically in the breast that was removed prophylactically
👉 Multiple studies have reported that the chance of finding invasive disease in the surgical specimen with prophylactic mastectomy is less than 3%
👉 In a large series from the MD Anderson Cancer Center that included 436 prophylactic mastectomies, cancer was identified in 22 (5%) cases
👉 Of these, the majority of patients (14) had ductal carcinoma in situ
👉 Only eight patients (1.8%) had invasive cancer, with a mean tumor size of 5 mm
👉 The study included 23 patients with BRCA mutations, and no invasive cancers were identified in these cases
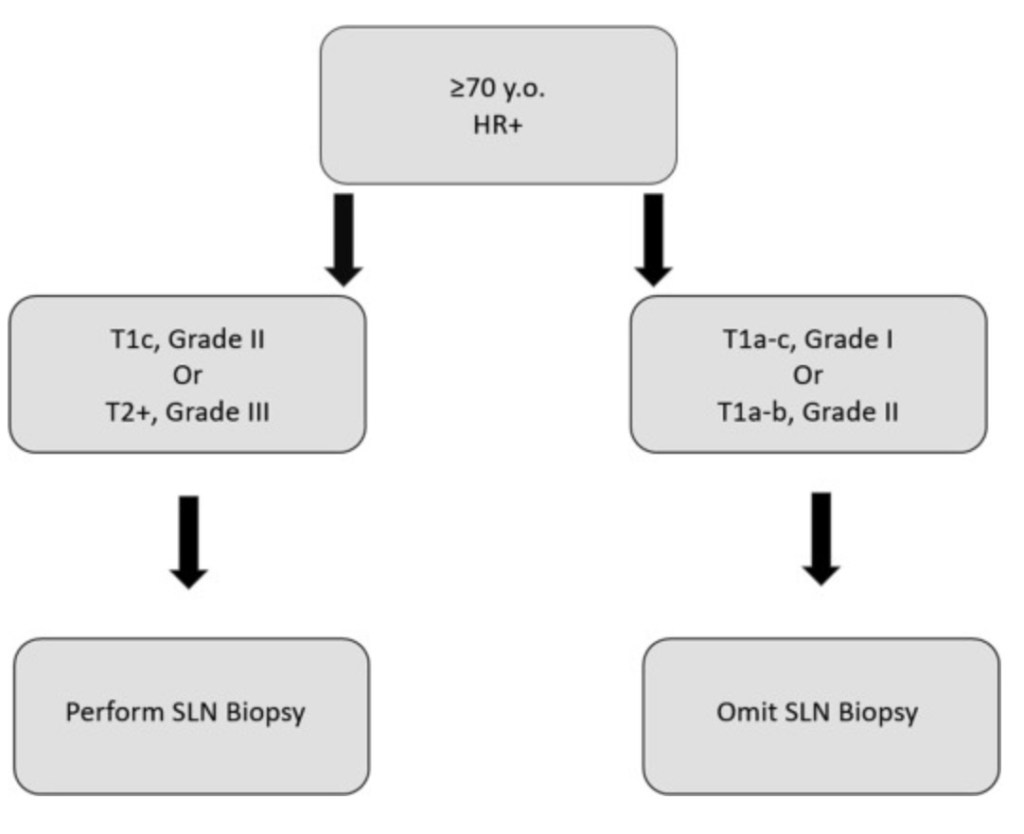
👉 Significantly increased risk of invasive cancer in the prophylactic mastectomy was seen in postmenopausal patients (3.7%; p=0.007), patients age greater than 60 years (7.5%; p=0.008), and patients with invasive lobular carcinoma (9.7%; p0.0002) or lobular carcinoma in situ (7.7%; p=0.008).
👉 A decision-analytic model was created by the same group to compare the risk / benefit ratio of routine SLNB for all prophylactic mastectomies compared to omitting SLNB and performing ALND only when invasive cancer is found in the breast
👉 The pertinent literature was reviewed to determine the chance of finding invasive cancer in a prophylactic mastectomy specimen and to estimate the chance of complications (lymphedema, paresthesias, decreased range of shoulder motion) with SNLB and ALND
👉 At a rate of finding invasive cancer of 1.9%, 73 SLNBs were required to avoid 1 ALND
👉 After reviewing the literature, the complication rate was estimated at 7% for SLNBs and 31% for ALND
👉 In one model scenario, the probability of complications per breast cancer detected was 9-fold greater with the SLNBs strategy than with the directed ALND strategy
👉 This model supported the decision to forego SLNB in most patients undergoing prophylactic mastectomy, given the large number of procedures required to benefit one patient

👉Rodrigo Arrangoiz MS, MD, FACS, FSSO cirujano oncólogo y cirujano de mamá en Mount Sinai Medical Center en Miami:
-
Es experto en el manejo del cáncer de mama

👉Es miembro de la American Society of Breast Surgeons:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


#Arrangoiz
#Surgeon
#Cirujano
#SurgicalOncologist
#CirujanoOncologo
#BreastSurgeon
#CirujanodeMama
#CancerSurgeon
#CirujanodeCancer