- Improvements in adjuvant therapy for breast cancer:
- Have allowed surgeons to perform less aggressive surgical procedures safely
- Axillary staging in women with hormone-positive (HR+) breast cancer (BC) and clinically negative lymph nodes has evolved from upfront axillary lymph node dissection (ALND) to sentinel lymph node mapping an biopsy (SLNM / SLNB):
- Landmark trial NSABP-32:
- Demonstrated no difference in survival or locoregional control in patients who received ALND compared to SLNB:
- Thereby propelling SLNM / SLNB as the gold standard for axillary evaluation in patients with negative clinical axillae
- Demonstrated no difference in survival or locoregional control in patients who received ALND compared to SLNB:
- Landmark trial NSABP-32:
- Although more slowly adopted, de-escalating axillary surgery by omitting SLMN / SLNB:
- Has been shown to be safe in selected patient populations such as:
- Older women with early-stage HR+ tumors
- Has been shown to be safe in selected patient populations such as:
- In Western countries:
- Nearly a third of breast cancers (BCs) occur in patients over 65:
- With the greatest incidence in women aged 75 to 79
- Nearly a third of breast cancers (BCs) occur in patients over 65:
- Given the central role of surgery:
- The question arises as to whether the surgical evaluation of the axilla is necessary for older patients with early BC and clinically negative axillary nodes
- The American Board of Internal Medicine Foundation:
- Launched a national initiative called Choosing Wisely to prompt provider discussion about the appropriate use of tests, treatments, and procedures based on evidence-driven medicine
- In conjunction with the Society of Surgical Oncology in 2016:
- Recommendations were released:
- The first recommendation stated “Don’t routinely use sentinel node biopsy in clinically node-negative women ≥70 years of age with early-stage hormone receptor-positive, HER2 negative invasive breast cancer”:
- This recommendation was based on several prospective trials highlighting that SLNB had no impact on locoregional recurrence or breast-cancer-specific mortality (BCSS)
- Recommendations were released:
- One such trial was conducted by Martelli et al evaluating the long-term safety of no axillary surgery for patients > 70 years old with operable BC and negative clinical axillae who received adjuvant endocrine therapy:
- This study found that axillary surgery did not increase overall survival (OS) or BCSS over 5 years
- The cumulative 15-year incidence of axillary disease:
- Remained low at 5.8% and 3.7% for T1 patients who received ALND compared to those who did not
- Martelli et al concluded there was:
- No benefit to axillary surgery for older patients with node-negative early BC who received BCS with adjuvant endocrine therapy
- Similarly, Chung et al evaluated the safety of SLNB omission in women >70 years old with T1 to T2 tumors:
- The 5-year OS was 70%:
- Whereas BCSS was 96%:
- Ischemic heart disease was the most common cause of death
- Whereas BCSS was 96%:
- The authors also found that adjuvant therapy was less likely to be offered regardless of nodal status, indicating that nodal status did not influence care:
- As patients were more likely to die from causes other than BC
- The 5-year OS was 70%:
- The IBCSG 10-93 trial:
- Assessed whether omitting axillary surgery in older people would improve quality of life (QOL) with equivalent disease-free survival (DFS) and OS:
- A total of 473 women received primary breast surgery with adjuvant tamoxifen and were randomly assigned to receive or omit axillary staging
- Adverse QOL effects from axillary surgery were evident early in the postoperative period but dissipated 6 to 12 months after surgery
- At the 6-year follow-up:
- There was no difference in DFS or OS
- The investigators concluded that the omission of axillary surgery corresponded with improved early QOL without differences in DFS or OS
- Assessed whether omitting axillary surgery in older people would improve quality of life (QOL) with equivalent disease-free survival (DFS) and OS:
- CALGB 9343:
- Which addressed the need for adjuvant radiation after a lumpectomy in early-stage HR+ BC in older people, included a small subset of patients who received no axillary surgery or radiation:
- In this patient cohort, only 3% developed ipsilateral axillary recurrence compared to no recurrences in patients who received radiation without axillary staging
- Due to low axillary recurrence among those who had omitted nodal surgery and radiotherapy:
- Authors surmised SLNB might be safely omitted in this population
- Which addressed the need for adjuvant radiation after a lumpectomy in early-stage HR+ BC in older people, included a small subset of patients who received no axillary surgery or radiation:
- Application of Choosing Wisely in clinical practice:
- After releasing the Choosing Wisely recommendation, Welsh et al sought to develop a risk stratification model to facilitate guideline adoption for patients at low risk for nodal positivity
- Using the National Cancer Database data from 2010 to 2013, a total of 71,834 patients met the criteria for SLNB omission
- The pathologic nodal positivity rate for patients with axillary staging was 15.3%
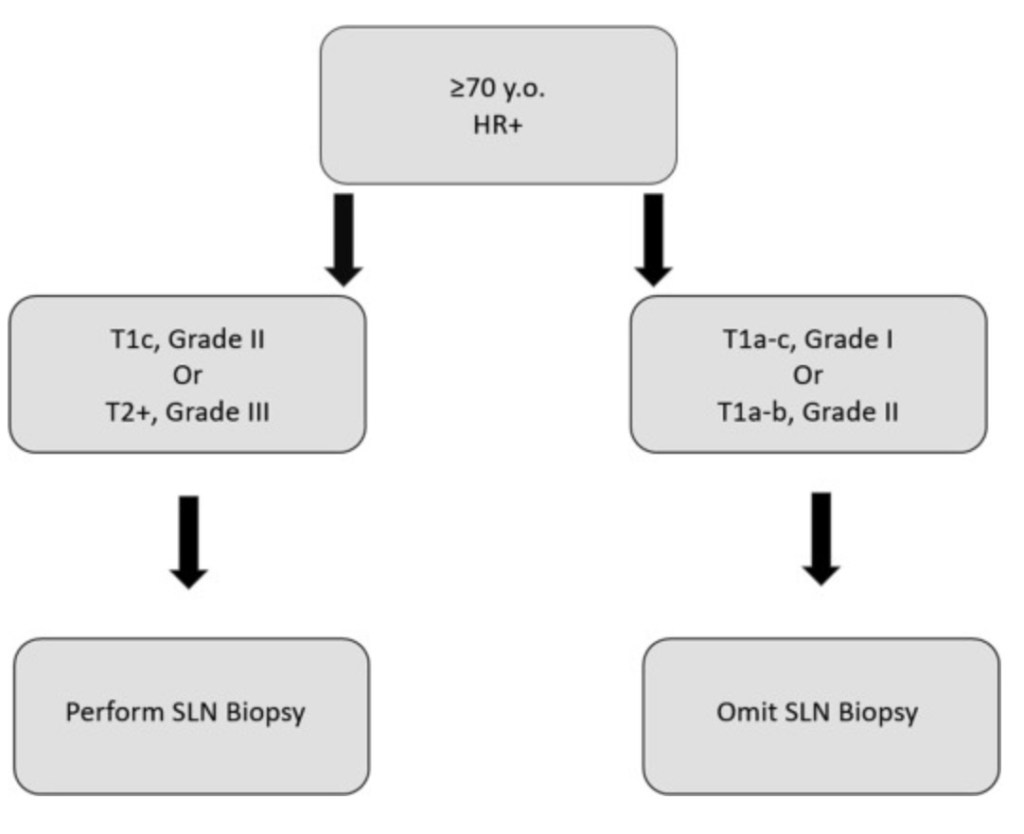
- Welsh et al classified low-risk patients as those with:
- Grade 1 less than 2 cm tumors or grade 2 less than 1 cm tumors:
- Translating to a nodal positivity rate of 7.8% compared to 22.3% among patients who did not meet low-risk criteria
- The authors concluded that SLNB might be safely omitted in older patients with:
- Grade 1 cT1mi to T1c HR+ tumors
- Grade 2 cT1mi to T1b HR+ tumors
- Grade 1 less than 2 cm tumors or grade 2 less than 1 cm tumors:
- Moorman explored the utility of a nomogram to aid decision-making for SLNB omission:
- Presenting a model with an excellent predictive value that can select one-third of patients in whom SLNB is deemed unnecessary because of a less than 5% chance of nodal involvement
- Similar nomograms have been adopted by MSKCC and the Mayo Clinic to predict the likelihood of nodal positivity
- Additionally, the ongoing prospective Sentinel Node Vs Observation After Axillary Ultra-souND trial:
- Examines the safety of SNLB omission in patients of any age with T1 tumors and clinically, radiographically negative axillae without prior systemic treatment:
- This trial will clarify the safety of SNLB omission in patients with small tumors while examining the effects on adjuvant treatment and quality of life
- Examines the safety of SNLB omission in patients of any age with T1 tumors and clinically, radiographically negative axillae without prior systemic treatment:
- Adherence to Choosing Wisely
- Several investigators have demonstrated the slow implementation of Choosing Wisely campaign in clinical practice
- For example, Wang et al examined 4 low-value BC operations identified through the Choosing Wisely campaign before and after evidence demonstrated that each procedure was unnecessary:
- The retrospective cohort study using the National Cancer Database registry, which included 1,500 facilities across the United States, examined a total of 920,256 women with a median age of 63 years diagnosed with BC between 2004 and 2016 and identified 4 low-value BC operation cohorts: ALND, lumpectomy margin reoperation, contralateral prophylactic mastectomy, and SLNB
- Although ALND and margin re-excision surgeries decreased during the study period, rates of contralateral prophylactic mastectomy and SLNB in older women increased
- Academic research programs and high-volume facilities demonstrated the greatest reduction in use, indicating that facility-level characteristics were associated with the use of low-value BC operations
- This was further corroborated by Armani et al, whose survey showed that although academic centers were more likely to practice according to national guidelines, adherence overall was low
- Tonneson et al identified a group of women at low risk of nodal positivity where SLNB may be omitted (grade 1, cT1mi-T1c, or grade 2, cT1mi-T1b) and evaluated the impact of SLNB omission by performing a retrospective chart review of women aged ≥70 years with HR+ node-negative BC at the Mayo Clinic between 2010 and 2020 and compared SLNB use before (2010–2016) and after (2017–2020) the Choosing Wisely guideline release according to clinical risk and the association with adjuvant therapy:
- This group found that the SLNB surgery rate significantly decreased from 90.6% (2010–2016) to 62.8% in 2020 (P < .001) and that this was driven by BCS with SLNB rates of 88.2% (2010–2016) and 46.7% in 2020
- In conclusion, the safety and efficacy of the omission of SLNB with ER+ BC in older people continues to be studied:
- Choosing Wisely states that routine SLNB should not be performed in this population, acknowledging that a subset of patients is low risk and may be spared the morbidity of axillary staging
- Ongoing research continues to identify these low-risk populations while improving adherence to Choosing Wisely guidelines to prevent overtreatment in the rest of this cohort

