The risk of underlying invasion in patients with DCIS:
Is roughly 25% (Bundred et al, BMJ. 2013) in this era of core biopsies
Risk of SLN metastasis in pure DCIS:
Is 0.2% to 0.7% (Zetterfund et al; BJS. 2014; Nicholson et al, EJSO. 2015):
Risk may rise to 9% if known micro-invasion (Meretoja et al, Ann Surg Onc. 2009)
Vacuum assisted devices (VAB):
Can lower the risk of invasion to 11% in retrospective data (Sumian et al, EJSO, 2016)
In prospective data (Cinnamome Study):
The upgrade was 39% (Tunon-De-Lara, Ann Surg Onco. 2015)
Routine MRI does not improve surgical outcomes:
Upgrade, size, or re-excision rates
(Fancellu et al, BJS. 2015; Chou et al ECON-AGRIN E4112, Radiology. 2021; Roque et al, NPJ breast cancer. 2022)
Dedicated breast PET? (Grana-Lopez et l Eur J Rad. 2020; Sasada et al, EJSO. 2021):
Up to know have not shown improve outcomes
There are approximately 50 retrospective studies evaluating nomograms and there predictive value on the risk of finding invasion in DCIS:
The usual risk factors are:
Size, grade 2 and 3, comedo necrosis, mass effect, micro-invasion:
Among “high-risk” DCIS:
Axillary evaluation in DCIS affects treatment but not survival (Coromilas et al, Ann Surg Onc 2016)
Axillary evaluation in DCIS increases complications and long-term morbidity (relative increase up to 6 to 8 times (Kilelea et al, Ann Surg Onc. 2018)
SLNB can be omitted in patients with DCIS planned for breast conserving surgery (BCS):
Detection rate at reoperation is 85.5% (GATA Study, Breast 2015)
NO data on feasibility after oncoplastic surgery
NO data on procedure accuracy
DCIS is noninvasive:
By definition, is unable to metastasize:
However, some studies have shown that up to 15% of patients with pure DCIS have isolated tumor cells (ITCs) or micrometastasis on nodal evaluation compared to others that show a 0.2% to 0.7% risk of nodal metastasis:
However, these small tumor deposits likely have little prognostic significance and may be cell clusters displaced by biopsy
In patients with DCIS detected by core biopsy:
There is a 15% to 25% associated risk of an invasive component when excised
Patients undergoing mastectomy for DCIS:
Should be offered SLNB since it would not be feasible to perform following mastectomy if invasive carcinoma is subsequently identified
ASCO consensus guidelines recommend that patients with DCIS who undergo breast-conserving operation should not routinely have SLNB:
However, SLNB could be discussed with patients undergoing breast conservation:
Who have a core biopsy diagnosis of DCIS and:
A large area of DCIS on imaging (2 to 5 cm)
High-grade DCIS
Comedonecrosis
When a physical examination or imaging shows a discrete mass
These findings have been associated with an increased risk of invasive cancer, and SLNB at the time of the initial operation could avoid a second operation
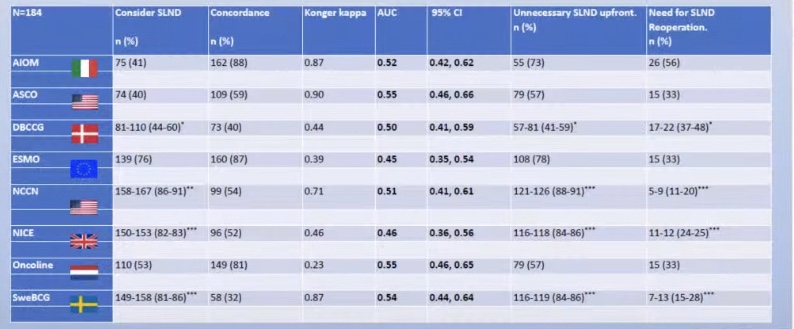
All of the guidelines that try and help us decide when to perform of SLNB in DCIS show a predictive value of a coin toss.
Studies continue to evaluate for a subset of patients with DCIS who may not require adjuvant radiation therapy following breast-conserving surgery
In a prospective nonrandomized trial, ECOG E5194 evaluated two cohorts of patients:
Groups:
Group 1 had ≤ 2.5-cm low- and intermediate- grade DCIS
Group 2 had ≤ 1 cm high-grade DCIS
Both cohorts had margins of at least 3 mm and did not receive adjuvant radiation therapy
Tamoxifen was given to 30% of patients
Local recurrence at 5 years was:
6.1% in group 1 and 15.3% in group 2
The rate at 12 years was:
14.4% in group 1 and 24.6% in group 2
There was no plateau in the incidence of local recurrence over time
The Radiation Therapy Oncology Group (RTOG) 9804 study:
Randomized patients with < 2.5 cm low- and intermediate-grade DCIS and margins ≥ 3 mm to adjuvant radiation or no radiation therapy following partial mastectomy
Seven-year outcomes demonstrated an increase in local recurrence with the omission of radiation therapy (6.7% vs. 0.9%)
Tamoxifen was given to 62% of patients
Similar outcomes were also noted in the Dana Farber Cancer Institute prospective trial of excision alone
Trials are currently underway evaluating the omission of surgery for low-risk DCIS including:
The COMET (grade 1/2 ADH/DCIS ER+, primary outcome: ipsilateral invasive cancer at 2 years) – data recently published
The LORD (age > 45, primary outcome: ipsilateral invasive breast cancer free rate at 10 years)
LORIS trials:
However, there is limited prospective data published with respect to outcomes for patients forgoing surgery.
References:
McCormick B, Winter K, Hudis C, et al. RTOG 9804: a prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J Clin Oncol. 2015;33(7):709-715.
Solin LJ, Gray R, Hughes LL, et al. Surgical excision without radiation for ductal carcinoma in situ of the breast: 12-year results from the ECOG-ACRIN E5194 study. J Clin Oncol. 2015;33(33):3938-3944.
Wong JS, Kaelin CM, Troyan SL, et al. Prospective study of wide excision alone for ductal carcinoma in situ of the breast. J Clin Oncol. 2006;24(7):1031-1036.
The breast extends from the lateral border of the sternum to the midaxillary line:
In some individuals, into the axilla itself
The adult breast consists of:
Glandular and adipose tissue:
Together with a system of connecting ligaments
1. Nipple:
This is located at the apex of the breast and projects up to 1 cm
Optimizing its positioning is of utmost importance in breast surgery
In the average adult female the nipples lie in the midclavicular line:
19 cm to 21 cm from the sternal notch and 9 cm to 11 cm from the midline:
But their position varies widely according to shape, size and age
2. Areola:
This is a circular area of skin that surrounds the nipple
Its color darkens during pregnancy due to the deposition of melanin
The areolar skin contains Montgomery glands:
Which secrete a protective oily lubricant
3. Glandular tissue:
The glandular tissue is the functional component of the lactating breast and the site of milk production, which is passed to the nipple via a system of ducts:
Each breast, or mammary gland:
Contains 15 to 20 lobes and each lobe is comprised of 20 to 40 terminal ductal lobular units (TDLU):
The TDLU is the functional unit of the breast
The breast mound is roughly hemispherical
The bulk of the glandular tissue is found in the upper outer quadrant:
Which is the commonest site of malignancy.
4. Adipose tissue:
This forms up to 70% of the breast mass:
It is the main determinant of breast size
5. Ligaments:
The structure and shape of the breast is maintained by fascial and ligamentous supports:
As first described by Sir Astley Cooper in 1840
Superficial fascial system:
The breast is enveloped by the superficial and deep laminae of the superficial fascia:
The superficial lamina is separated from the dermis by a thin layer of fatty tissue:
But is often difficult to identify as a separate entity
Suspensory ligaments of Cooper:
These fibrous strands extend through the breast parenchyma between the layers of the superficial and deep (pre-pectoral) fascia:
They help to maintain a non-ptotic breast shape
6. Axillary tail (of Spence):
There is a variable extension along the inferior edge of pectoralis major towards the axilla
This usually lies within the subcutaneous fat but may penetrate the axillary fascia to lie adjacent to the lymph nodes
Occasionally it is a separate entity with ducts that do not drain to the nipple.
7. Retromammary space:
In reality this is not a space but a plane of loose connective tissue lying between the deep lamina of the superficial fascia and the deep pre-pectoral fascia
Chassaignac bursa (also known as the retromammary bursa, submammary serous bursa or occasionally Chassaignac bag):
Is the space behind the breast, lying between the pectoralis fascia posteriorly and deep layer of superficial fascia anteriorly
This is the plane of dissection in which a subglandular pocket can be created for insertion of a prosthesis for breast augmentation
8. Muscle:
The medial two-thirds of the base of the breast lie over the pectoralis major muscle
The lateral one-third lies over serratus anterior and a small portion of the rectus abdominis and external oblique muscles
The muscles are separated from the breast by the deep fascia
9. Rib cage:
Deformities of the ribs, including those that are secondary to a spinal deformity can lead to an apparent asymmetry of breast position and/or shape
Vascular Supply of the breast:
The breast has a rich blood supply:
Which permits safe division and excision of breast tissue:
The viability of the nipple areolar complex is dependent on vessels that pass through the gland:
Which must therefore be preserved
There are three main arterial systems:
Internal Thoracic (Mammary) Artery:
Is responsible for roughly 60% of the vascular supply to the breast
Arising directly from the subclavian artery, the internal thoracic artery passes posterior to the subclavian vein and runs along the edge of the sternum, deep to the costal cartilages
Perforating branches of the internal thoracic artery pass through the 2nd to 6th intercostal spaces to supply the medial half of the breast:
The 2nd and 3rd perforators are the predominant vessels and these are preferred for anastomosis when reconstructing the breast with a free tissue transfer
Lateral Thoracic Artery:
A branch of the second portion of the axillary artery:
Supplies the upper outer quadrant of the breast
The lateral thoracic artery runs along the lower border of the pectoralis minor muscle and curls around the lateral border of pectoralis major to enter the breast
Other branches of the lateral thoracic artery perforate pectoralis major to supply the overlying breast tissue
Posterior Intercostal Arteries:
The lateral branch of the posterior intercostal arteries divides into posterior and anterior branches
The anterior branches from the 3rd to 6th intercostal spaces supply the lateral portion of the breast and the overlying skin through their mammary branches
Other Supply:
The axillary artery also provides other branches to the breast, including the:
Superior thoracic artery:
A branch from the first part of the axillary artery)
The pectoral branch of the thoracoacromial artery and the subscapular artery
The venous drainage of the breast is via two venous systems:
Superficial system:
Which lies within the subdermal venous plexus:
The pattern of drainage is highly variable
Deep system:
The deep venous system parallels the arterial supply:
The medial half of the breast drains via veins that accompany the perforating branches of the internal mammary artery through the intercostal spaces, back to the internal mammary vein
The lateral thoracic veins drain into the axillary vein
The posterior intercostal veins drain into the azygous vein on the right and the hemiazygous vein on the left
Innervation of the breast:
The nerve supply to the breast consists of sensory fibres from the skin and sympathetic efferent fibres to the blood vessels, glandular tissue and smooth muscle cells in the skin and nipple
The sensory nerve supply is derived from cutaneous branches of the intercostal nerves:
Medially:
Anterior branches of the 1st to 6th intercostal nerves
Laterally:
Lateral branches of the 2nd to 6th intercostal nerves
Nipple areola complex:
Supplied by the anterior branch of the 4th intercostal nerve
There is an extensive nerve plexus within the nipple
The skin of the nipple areola complex contains free nerve endings, Meissner’s corpuscles and Merkel disc endings
Partial mastectomy only or partial mastectomy followed by lattice radiotherapy (LRT; a novel technique of delivering heterogeneous doses of radiation to voluminous tumors not amenable to surgery) for the treatment of localized DCIS
The trial showed a clear benefit for the addition of radiation
Patients enrolled in the NSABP B-24 trial:
Were randomly assigned to receive LRT or LRT plus tamoxifen (LRTT)
At 15-year follow-up:
The risk of death in these trials was low:
Ranging from 2.3% for patients who had LRTT to 4.7% for patients who had LRT
Ipsilateral breast tumor recurrence was:
35% (19.6% invasive, 15.4% DCIS) in the lumpectomy only arm of B-17 and 19.8% (10.7% invasive, 9.0% DCIS) in the LRT arm
In B-24 IBRT was 16.6% (9.0 invasive, 7.6% DCIS) in the LRT arm and 13.2% (6.6% invasive, 6.7% DCIS) in the LRTT arm
The risk of contralateral new primary ranged from:
4.9% (3.3% invasive, 1.6% DCIS) in the LRTT arm of B-24 to 9.3% (5.6% invasive, 3.7% DCIS) in the LRT arm of B-17
References:
Wapnir IL, Dignam JJ, Fisher B, Mamounas EP, Anderson SJ, Julian TB, et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J Natl Cancer Inst. 2011;103(6):478-488.
Was a phase 3 clinical trial that randomized postmenopausal women with ER positive DCIS (n = 3,104) to either five years of anastrozole or tamoxifen following breast-conserving surgery and radiation:
The trial sought to determine how effective anastrozole was compared to tamoxifen in preventing a breast cancer occurrence
With a median follow-up of 9 years:
Investigators found significantly fewer breast cancer events in the anastrozole group (n = 90) than in the tamoxifen group (n = 122)
The 10-year breast cancer event rate was lower among women randomized to anastrozole compared to tamoxifen:
6.9% [anastrozole] vs. 10.9% [tamoxifen], HR 0.73, p=0.02
This recorded difference in breast cancer events was attributable almost entirely to:
Younger postmenopausal women less than 60 years of age who received tamoxifen
Women less than 60 receiving tamoxifen had nearly twice the events as those receiving anastrozole:
Events on tamoxifen: 63 vs events on anastrozole: 34, HR 0.53 (0.35-0.80), p=0.0026)
Interestingly, the difference between treatments did not become apparent until after 5 years of follow-up:
Likely due to the low number of events in both groups
There was no difference in overall survival (OS) between the two treatment groups:
The 10-year estimates for overall survival were 92.1% for the tamoxifen group and 92.5% for the anastrozole group (p=0.38)
In B-35, anastrozole was found to further significantly reduce the rate of contralateral invasive cancer compared with tamoxifen
Based on this trial and others:
Aromatase inhibitors are the preferred adjuvant hormonal therapy for ER positive disease in post-menopausal women with either DCIS or invasive breast cancer:
Provided they have no contraindications to taking an aromatase inhibitor
References
Margolese RG, Cecchini RS, Julian TB, Ganz PA, Constantino JP, Vallow LA, et al. Anastrozole versus tamoxifen in postmenopausal women with ductal carcinoma in situ undergoing lumpectomy plus radiotherapy (NSABP B-35): a randomised, double-blind, phase 3 clinical trial. Lancet. 2016;387(10021):849-856
M Baum, AU Budzar, J Cuzick, et al., ATAC Trialists’ Group. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomized trial. Lancet. 2002;359(9324):2131-2139.
Is a rare benign inflammatory breast disease first described in 1972 by Kessler and Wolloch
The most common presenting symptom is:
A unilateral, firm, and discrete breast mass:
Which may be accompanied by overlying skin changes and / or possible lymph node involvement
The average duration of symptoms is around 3.9 months with:
The most common signs and symptoms including:
Discrete mass
Tenderness to palpation
Erythema
Swelling
The pain could be out of proportion to findings:
Suggestive of a localized ischemic etiology
The pain could be a motivating factor in prompting all symptomatic patients to seek consultation
The lesion may occur in any quadrant of the breast:
But often extends radially from the retroareolar region
The disease often presents in women:
Of childbearing age:
With a recent history of pregnancy or ongoing lactation:
The mean age of diagnosis is around:
31.7 years and all within reproductive years
The high majority of women are:
Hispanic or African / African-American ancestry
A history of previous granulomatous disease (tuberculosis, sarcoidosis, autoimmune disease, or granulomatous disease) is very rare
The overlap of presenting symptoms with other disease processes such as:
Malignancy, acute or chronic infections, and chronic inflammatory diseases:
Makes definitive diagnosis difficult
Because the differential may include malignancy:
The patient may experience significant anxiety during the evaluation
In addition, the broad differential and the lack of pathognomonic features make definitive diagnosis difficult:
Often resting as a diagnosis of exclusion on a clinical basis
The typical mammographic and ultrasonographic findings of granulomatous mastitis are:
Mammogram:
Ill-defined mass to an asymmetric density without specific margins
It is usually not accompanied by microcalcifications or architectural distortion
Ultrasound:
Heterogeneously hypoechoic lesion
Segmental masses with ill-defined margins, with tubular structures extending from the mass:
The tubular structures may be clustered, separate or contiguous
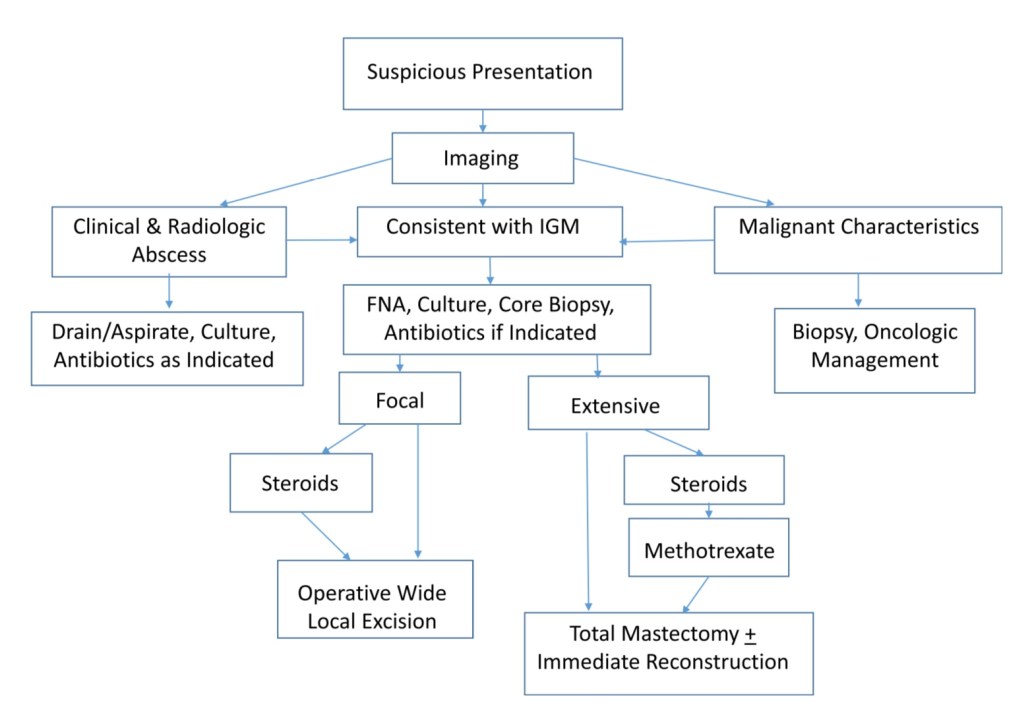
Malignant features or findings:
Suspicious microcalcifications, architectural distortion, or intra-ductal mass:
Would warrant appropriate histologic diagnosis and subsequent management
If the findings clinically and radiographically indicate an abscess:
They warrant treatment with antibiotics along with drainage by aspiration or incision, if the abscess is larger
Idiopathic granulomatous mastitis is usually regarded as a sterile process:
However, there is evidence to suggest a link to Corynebacterium kroppenstedtii infection or colonization:
This would then mandate routine cultures
One-third of the patients with granulomatous mastitis who are evaluated:
Have findings suggestive of an abscess
Because diagnosis is difficult, patients typically have received:
Prolonged courses of antibiotics, frequent biopsies, or surgical procedures
With a lack of pathognomonic imaging findings associated with granulomatous mastitis:
Histopathology is key to confirming a diagnosis
Histologically:
The disease has been described as non-caseating granulomas among epithelioid histiocytes and multinucleated giant cells surrounded by lymphocytes and plasma cells
Histologic differentials begin with the use of:
Hematoxylin and eosin stains, gram stain, and may also include acid fast stains and Grocott’s methenamine silver to evaluate for the possibility of sarcoidosis or mycobacterium infection
Once the diagnosis is made, treatment strategies are not clearly delineated but are often supportive
Steroid treatment has been shown to decrease the extent of involvement, and enable complete resection with removal of less breast tissue should resection be pursued:
However, lower doses have also proven to be efficacious and help to avoid adverse effects of weight gain, hyperglycemia, and Cushingoid symptoms
Regimens of 16 mg of prednisone twice a day for two weeks with a slow taper over a two-month period are described in the literature, as is prednisolone 30 mg/day for eight weeks, with taper
If symptoms do not improve, a course of methotrexate could be utilized:
Since there is a contingent who feel that this disease is an abnormal immune response
Success with methotrexate, including administration in steroid refractory cases:
Is limited to small studies of 3 to 5 patients
In consideration of the duration of symptoms patients experienced, along with the lack of durable evidence favoring treatment with methotrexate, our institution favors proceeding directly to surgery in steroid-refractory cases
We recommend the surgical options of:
Wide local excision for focal involvement and
Total mastectomy with the option of reconstruction for diffuse involvement
A 15% to 20% recurrence rate has been reported for surgery alone:
And inversely proportional to negative surgical margins
In light of the fact that these masses are painful and may lead to fistula formation and deformity:
Intervention may be the preferred path to avoid progression or static disease
Our experience allowed for a trial of “conservative” medical management for two months:
Followed by treatment escalation for lack of progress
A course of methotrexate may be entertained in patients who desire continued attempts at medical management, to help preserve breast tissue
However, it is not included in the first line of conservative management
DCIS is a proliferation of malignant cells that have not breached the ductal basement membrane:
They arise from ductal epithelium:
In the region of the terminal ductal–lobular unit (TDLU)
DCIS had previously been considered one stage in the continuum of histologic progression from ADH to invasive carcinoma:
But, in fact, DCIS comprises a heterogeneous group of lesions:
With variable histologic architecture, molecular and cellular characteristics, and clinical behavior
Malignant cells proliferate:
Until the ductal lumen is obliterated
There is an associated breakdown of the myoepithelial celllayer of the basement membrane surrounding the ductal lumen
DCIS has also been linked with changes in the surrounding stroma resulting in:
Fibroblast proliferation
Lymphocyte infiltration
Angiogenesis
Thus, although the process is poorly understood:
Most but not all invasive ductal carcinomas are believed to arise from DCIS:
Which is considered a nonobligate precursor of invasive breast carcinoma
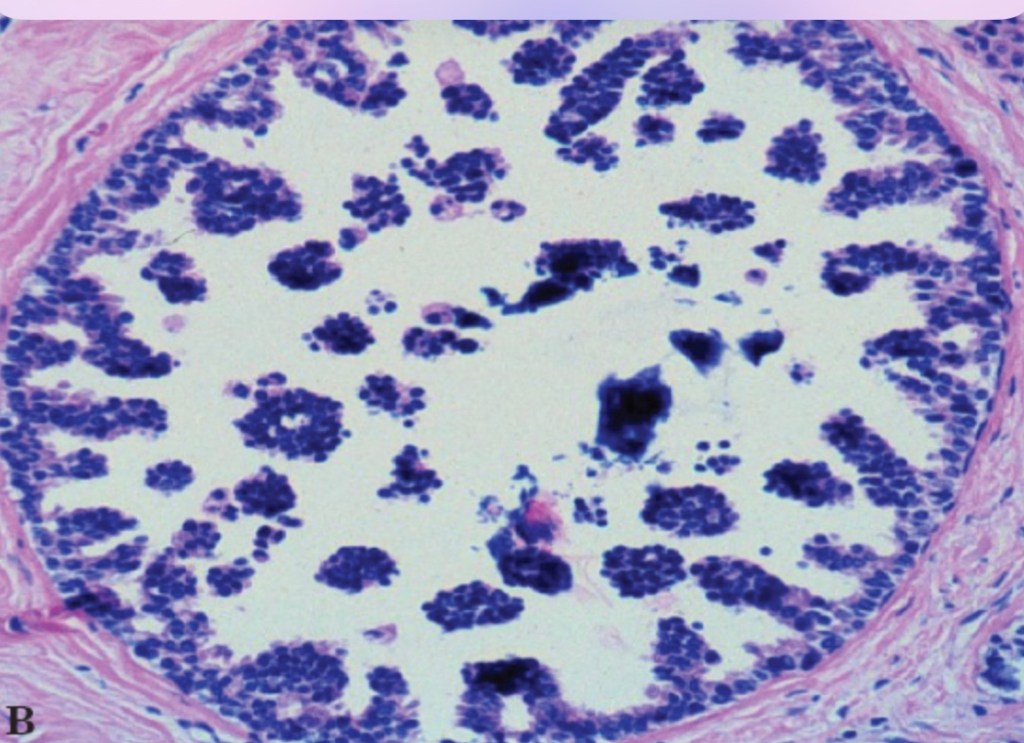
Architectural heterogeneity is a common feature of DCIS. Even in the same lesion, DCIS may show different growth patterns. Image is showing a cribriform DICSMicropapillary DCISPapillary DCISSolid DCIS
Most patients with papillary thyroid cancer (PTC) have an excellent prognosis:
But predicting which patients do not do well has been an ongoing area of interest
Ideally, identifying those at higher risk of cancer recurrence:
Would potentially allow the more aggressive therapies to be utilized when appropriate for patients with high risk papillary thyroid cancer
A lot of work has identified molecular markers, which are mutations in cancer-related genes that can help in the diagnosis of thyroid cancer on thyroid biopsy specimens
Two specific molecular markers, BRAFv600E and TERT promotor mutations:
Have been associated with aggressive tumor behavior and worse outcomes in papillary thyroid cancer
The BRAFv600E mutation is quite common in papillary thyroid cancer:
So using this mutation alone to predict outcome has been challenging, though it has been associated with poor prognosis
The TERT promoter mutation alone was not shown to cause adverse outcomes in some previous studies, though other studies suggested it was associated with a more aggressive clinical picture
A study by Moon S et al. aimed to determine the prognosis of papillary thyroid cancer in patients with either of these mutations alone or in combination by a review of the current studies:
Moon S et al. Effects of coexistent BRAFV600E and TERT promoter mutations on poor clinical outcomes in papillary thyroid cancer: a meta-analysis
Summary of the Study:
A literature review was done to identify studies that included BRAFV600Eand TERT promoter mutations in thyroid cancer
A total of 13 studies were identified
Data was extracted and reviewed for clinical information to include the number of males and females, age at diagnosis, cancer stage, spread to lymph nodes, extrathyroidal extention, spread outside of the neck, cancer recurrence and death
A total of 4347 patients with papillary thyroid cancer were evaluated in the study and 283 patients had both BRAFv600E and TERT promoter mutations
A BRAFv600E mutation alone:
Was related to advanced age at time of diagnosis, advanced cancer stage, extrathyroidal extension of tumor, and spread to lymph nodes, compared with no mutation
A TERT promoter mutation alone:
Was associated with older age at diagnoses, spread to lymph node and spread outside of the neck
The combination of BRAFv600E and TERT promoter mutations together when compared with no mutations:
Was associated with older age at diagnosis, male gender, advanced cancer staging, extrathyroidal extension, spread to lymph node and spread outside of the neck
Overall, the combination of BRAF600E and TERT mutations:
Was associated with high recurrence rate when compared with no mutations
Further, it was noted that the combination of mutations also had a higher risk of death than no mutations or BRAFv600E alone, although few patients were in this group
What are the implications to this study:
This study shows that molecular marker analysis can be used to identify patients that have more aggressive thyroid cancer
The combination of BRAFv600E and TERT promotor mutations worsens the prognosis for papillary thyroid cancer
Additionally, a limited data set suggested higher risk of death with the combination of BRAF600E and TERT promoter mutations
As we improve our understanding of the molecular changes in thyroid cancer, we will improve our ability to identify patients that have a more aggressive thyroid cancer
Ultimately this knowledge will lead to improved treatment options
Future studies must aim to determine if identifying these mutations at the time of diagnosis can lead to improved outcomes for patients at higher risk