Diagnosis:The diagnosis of medullary thyroid cancer (MTC):Is usually made after fine-needle aspiration (FNA) biopsy in a patient who has a solitary thyroid nodule (or a dominant nodule within a multinodular goiter):The sensitivity of FNA is 50% to 80%:Although higher sensitivity can be obtained by the addition of immunohistochemical staining for calcitoninIf the clinical suspicion for MTC is high:Patient with diarrhea, flushing, and a thyroid nodule):Calcitonin can be measured in the washout of the FNA biopsy needle:Although this may not be readily available in many commercial laboratoriesIn some cases:The diagnosis of MTC is made after thyroid lobectomy for a suspicious or indeterminate FNA biopsy:Surgical specimens from patients with MTC show:Spindle-shaped and frequently pleomorphic cells without follicle development:Because these cells originate from the calcitonin-producing parafollicular C cells of the thyroidThe use of serum calcitonin screening to complement ultrasound and FNA in the routine diagnosis of thyroid nodules is controversial in the United States:Measurement of serum calcitonin has not been a part of the routine evaluation of patients with thyroid nodules in the United States:The high frequency of falsely elevated serum calcitonin values, the inability to confirm the high calcitonin by pentagastrin stimulation in the United States, and the accuracy of FNA biopsy:Would argue against a change in this recommendation
Further, occasional patients with locoregional metastases or locally invasive MTC will have normal unstimulated serum calcitonin concentrations
In some countries (eg, European countries) where pentagastrin is available, however, serum basal and stimulated calcitonin levels are routinely used in the evaluation of thyroid nodules to facilitate the preoperative diagnosis of MTC
Differential Diagnosis:The differential diagnosis in a patient presenting with a neck mass:Is extensive and varies with the age of the patient at presentationThe majority of these masses represent benign thyroid nodules and cysts
Neck masses that are not of thyroidal origin may be from:Congenital:Vascular anomaly)Inflammatory:Lymph node enlargement)Other neoplastic:Primary or metastatic disease disorders
In addition to medullary thyroid cancer (MTC):Elevated calcitonin results may also be seen in patients with:Hypercalcemia
Hypergastrinemia
Neuroendocrine tumors
Renal insufficiency
Papillary and follicular thyroid carcinomas
Goiter
Chronic autoimmune thyroiditis
Prolonged treatment with:Omeprazole (greater than two to four months)Beta blockersGlucocorticoids:Has been associated with hypercalcitoninemia
In addition, the presence of heterophilic antibodies to calcitonin:Can falsely elevate serum calcitonin levels
Elevated carcinoembryonic antigen (CEA) levels can also occur in patients with:Heterophilic antibodiesGastrointestinal tract inflammatory diseaseBenign lung diseaseNonthyroid malignanciesCigarette smoking
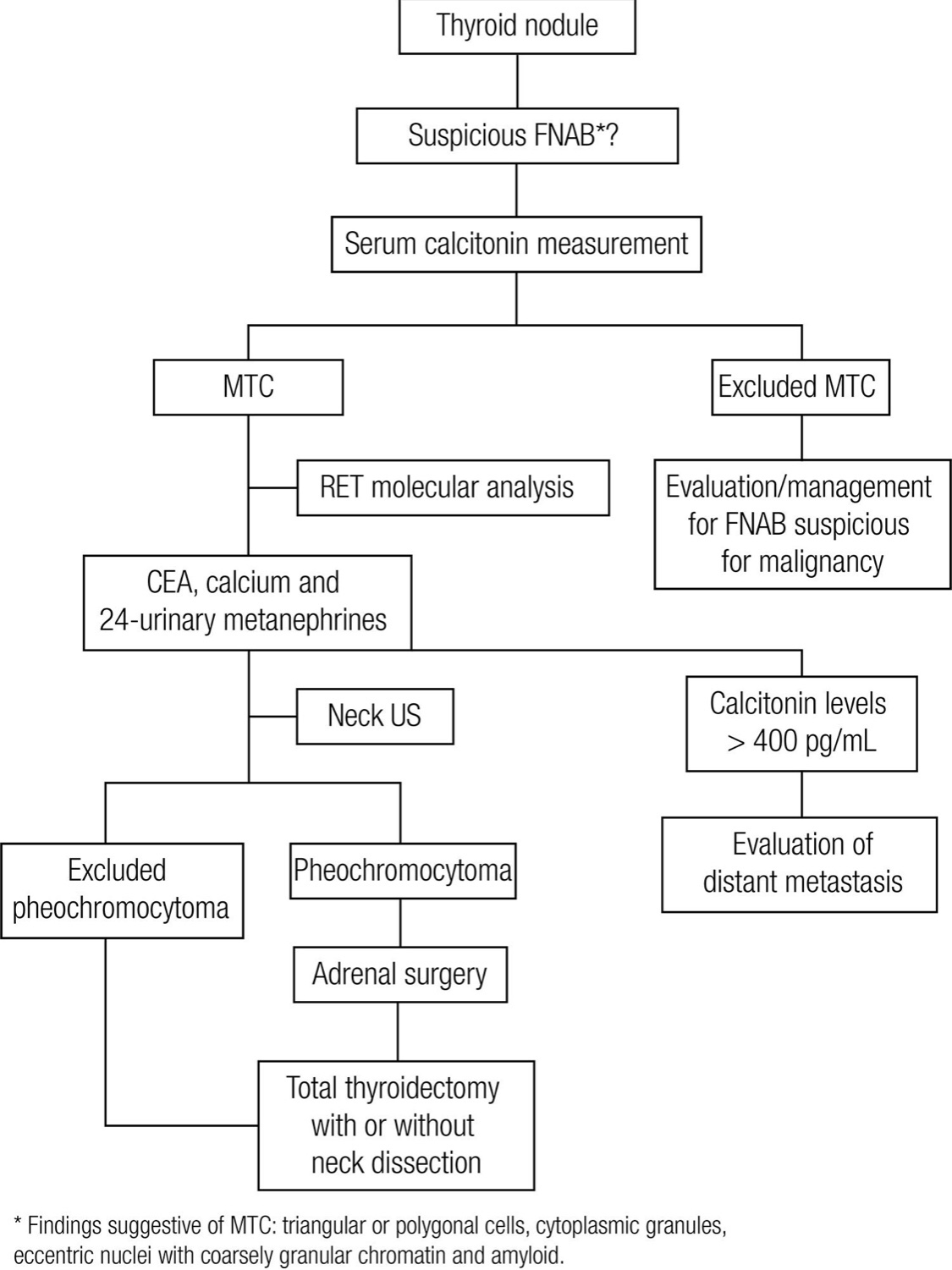
Evaluation:For patients diagnosed with medullary thyroid cancer (MTC) on the basis of cytologic evaluation of a thyroid nodule:Evaluation should include:Measurement of serum calcitonin, carcinoembryonic antigen (CEA), ultrasonography of the neck (if not already performed), genetic testing for germline RET mutations, and biochemical evaluation for coexisting tumors, especially pheochromocytoma. Serum calcitonin and CEA:The serum calcitonin and carcinoembryonic antigen (CEA) concentrations should be measured in patients diagnosed with MTC on the basis of cytologic evaluation of a thyroid nodule:
These tests can establish that the tumor is capable of hypersecreting the hormones and, if so, the values can be compared with postoperative values
Postoperatively:Results may provide a prognostic factor or indicate biochemical cure
In a study of 226 patients with MTC:Preoperative serum calcitonin concentrations:Where significantly correlated with tumor size in both the sporadic and familial casesIn addition, among 45 patients who had a preoperative serum calcitonin concentration of 50 pg/mL or less:44 had normal concentrations after surgery:In contrast, only 50 of 120 patients with preoperative serum calcitonin concentrations higher than 50 pg/mL had normal concentrations after surgery
In a second study of 224 patients with MTC:62% of patients without nodal metastases had normal calcitonin postoperatively:10% of node positive patients had normal postoperative calcitonin levels
Assessment of calcitonin and CEA doubling times postoperatively:Provides sensitive markers for progression and aggressiveness of metastatic MTC:Postoperative calcitonin doubling time was a prognostic factor for survival in a study of 65 patients followed for 3 to 30 years: Ten-year survival was: 8%, 37%, and 100% for doubling times:Under six months, between six months and 24 months, and greater than 24 months, respectively
Radiologic evaluation:MTC can spread by:Local invasion or metastasis:Within the neck or distantlyWhen MTC is diagnosed by fine-needle aspiration (FNA) biopsy:Ultrasonography of the neck is indicated to look for cervical lymph node involvementFor patients with local lymph node metastases on ultrasound or with preoperative serum basal calcitonin > 500 pg/mL (indicating high risk of local or distant metastatic disease):Additional imaging is required to assess for metastatic disease:In this setting, based con literature review I suggest cross-sectional imaging including:Chest computed tomography (CT)
Neck CT with IV contast
Three-phase contrast-enhanced liver CT or contrast-enhanced liver magnetic resonance imaging (MRI)
Axial MRI, and bone scintigraphy:In patients suspected of having skeletal metastases:MRI may be superior to other imaging modalities
I do not recommend 18-fluoro-2-deoxyglucose positron emission tomography (FDG-PET) imaging or somatostatin receptor imaging:For routine initial screening for metastatic disease:The sensitivity of FDG-PET scanning for detecting metastatic disease is variable:But improves with higher calcitonin levels:Sensitivity 78% versus 20% for basal calcitonin value greater than or less than 1000 pg/mL, respectively)
The use of radionuclide imaging with 111-In-octreotide or 99m-Tc-DMSA:Is not currently recommended for routine initial screening for metastatic disease:However, three patients have been described who had regional and distant metastases of MTC detected by somatostatin receptor scintigraphy but not by CT scan
How to select patients with a negative CT scan to undergo somatostatin receptor scintigraphy is not clear:Scanning may be more useful in localizing residual or recurrent disease after primary therapy
Genetic screening in sporadic MTC:Germline RET testing:In all patients with newly diagnosed C cell hyperplasia or apparently sporadic MTC:Initial germline testing in patients with C cell hyperplasia or apparently sporadic MTC should include:Sequencing of exons 10, 11, and 13 through 16 of the RET gene
Sequencing of the remaining exons in the RET gene should be considered in patients with:Clinical features or family history highly suggestive of hereditary medullary syndromes:Who demonstrate no mutations in exons 10, 11, or 13 through 16
While it is possible for clinicians to directly order genetic testing from reference laboratories:It is strongly encourage to have a consultation with genetic counselors who are familiar with both the ethical issues and legal informed consent requirements (which can vary significantly in different regions) that are involved in germline testing
When the index patient is positive for a germline mutation:Family members should be offered genetic counseling and genetic screening
An important question is what proportion of patients with apparently sporadic MTC have unsuspected germline mutations in the RET proto-oncogene (the underlying defect in MEN2) and, therefore, have heritable disease:Studies of unselected patients with MTC have found, on average:That approximately 6% to 7% (range 1.5% to 24%) have germline RET mutationsIn one report:35 of 482 patients (7.3%) with apparently sporadic MTC had mutations, and in 18 of these 35:Gene carriers were identified in relatives
75% of the familial medullary cases:Had no prior family history:A much higher percentage (approximately 60%) of patients with sporadic MTC have somatic (acquired) mutations in the RET gene within the tumor cells:These mutations are present only in the tumor cells and are not detected by standard genetic testing, ie, using leukocyte DNA
The presence of somatic RET mutations correlate with:Lymph node metastasesPersistent diseaseLower survivalHowever, in one study:Only mutations in exons 15 and 16 of the RET gene:Were associated with the worse prognosis:While those in other exons had a more indolent course
Since it is unclear how knowledge of a specific somatic (acquired) RET mutation should impact clinical management:I do not routinely test tumor samples
Testing for coexisting tumors:Most patients require biochemical evaluation for coexisting tumors (particularly pheochromocytoma and hyperparathyroidism) prior to thyroidectomy:Even when genetic screening is performed preoperatively:The results are rarely known prior to surgery.For patients with unknown RET mutational status and for patients who have a germline RET mutation:Serum calcium:To rule out hyperparathyroidism requiring concomitant surgical interventionPlasma fractionated metanephrines:As the initial screen for pheochromocytoma):Normal plasma fractionated metanephrines values:Exclude a symptomatic catecholamine-secreting neoplasm
Mildly elevated values of normetanephrine could be falsely positive:In which case additional evaluations including 24-hour urinary fractionated metanephrines, catecholamines, and adrenal imaging may be required to effectively rule in or rule out pheochromocytoma prior to surgery:Adrenal imaging should not be performed unless there is biochemical evidence suggesting a possible pheochromocytoma. (See
In a patient with negative RET proto-oncogene testing and no family history of MEN2 syndrome:Biochemical testing for coexisting tumors is typically not required
What is Head and Neck Surgery?:
It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
The head and neck surgeon’s work area:Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:This is the neurosurgeon field.
Among the diagnostic procedures performed by the head and neck surgeon, are the following:
Nasopharyngolaryngoscopy:
Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions.
The surgeries most commonly performed by the head and neck surgeon are:
Total or near total thyroidectomies
Hemithryoidectomies (lobectomies)
Comprehensive neck dissections
Selective neck dissections
Maxillectomies:
Total maxillectomy
Subtotal maxillectomy
Infrastructure maxillectomy
Suprastructure maxillectomy
Medial maxillectomy
Mandibulectomy:
Segmental
Marginal
Tracheostomy
Salivary gland surgeries:
Parotid gland operations:
Limited superficial parotidectomy with identification and preservation of the facial nerve
Superficial parotidectomy with identification and preservation of the facial nerve
Near total parotidectomy with identification and preservation of the facial nerve
Total parotidectomy
Submandibular gland resection
Sublingual gland resection
Resection of tumors of the oral cavity:
Glossectomy
Resection of the floor of the mouth tumors
Resection of tumors of the pharynx
Resection of tumors of the larynx
Split-thickness skin grafts
Full-thickness skin grafts
Sentinel lymph node mapping and sentinel lymph node biopsy
Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
The formation of the head and neck surgeon includes mastering the following subjects:
Surgical Anatomy
History and Basic Principles of Head and Neck Surgery
Epidemiology, Etiology, and Pathology of Head and Neck Diseases
Diagnostic Radiology of the Head and Neck Region
Tumors of the Scalp, Skin and Melanoma
Eyelids and Orbit
Nasal Cavity and Paranasal Sinuses
Skull Base and Temporal Bone
Lips and Oral Cavity
Pharynx and Esophagus
Larynx and Trachea
Cervical Lymph Nodes
Thyroid and Parathyroid Glands
Salivary Glands
Neurogenic Tumors and Paragangliomas
Soft Tissue Tumors
Bone Tumors and Odontogenic Lesions
Reconstructive Surgery
Oncologic Dentistry and Maxillofacial Prosthetics
Principles of Radiation Oncology
Principles of Chemotherapy
Molecular Oncology, Genomics and Immunology
Nutrition
Biostatistic
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
Rodrigo Arrangoiz MS, MD, FACS:
Is a member of the American Head and Neck Society
He is a member of the American Thyroid Association:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
The neuroendocrineparafollicular C cellsor C cells of the thyroid gland
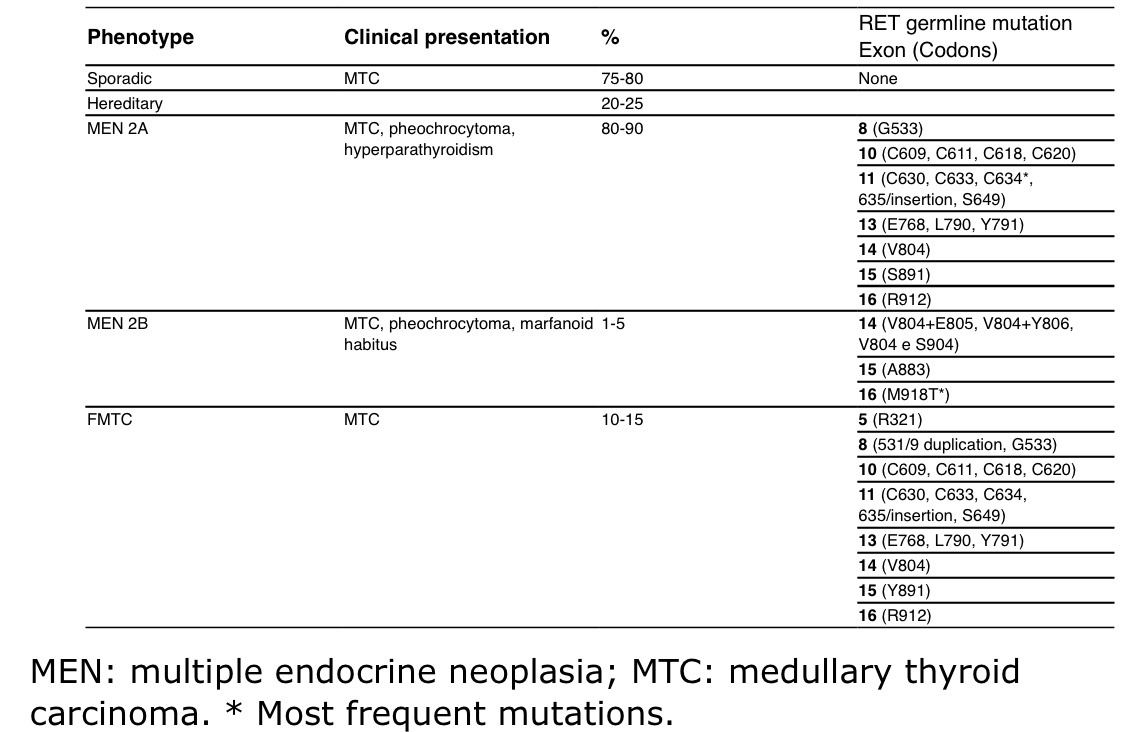
Sporadic MTC accounts for about 75% to 80% of all cases of the disease:
The remaining cases – 20% to 25% consist of inherited tumor syndromes, such as:
MEN type 2A (MEN2A):
Which is the most common type
MEN2B
Familial MTC:
Is now viewed as a variant of MEN2A
Sporadic disease:
Typically presents in the fifth or sixth decade of life
Inherited forms of the disease:
Tend to present at earlier ages
The 5-year relative survival for:
Stages I to III:
93%
Stage IV:
28%
Because the C cells are predominantly located in the upper portion of each thyroid lobe:
Patients with sporadic disease typically present with:
Upper pole nodules
Metastatic cervical adenopathy:
Appears in about 50% (50% to 70%) of patients at initial presentation
Symptoms of upper aerodigestive tract compression or invasion:
Are reported by up to 15% of patients with sporadic disease
Distant metastases:
In the lungs or bones cause symptoms:
In 5% to 10% of patients
Many patients with advanced MTC can have:
Diarrhea, Cushing syndrome, or facial flushing:
Because the tumor can secrete calcitonin and sometimes other hormonally active peptides (ie, adrenocorticotropic hormone [ACTH], calcitonin gene-related peptide [CGRP]):
Treatment with somatostatin analogs (eg, octreotide, lanreotide) may be useful in patients with these symptoms
Patients with unresectable or metastatic disease:
May have either slowly progressive or rapidly progressive disease
Nodule Evaluation and Diagnosis Patients with MTC:
Can be identified by using:
Pathologic diagnosis or by prospective genetic screening
Sporadic MTC:
Is usually suspected after FNA of a solitary nodule
Reports suggest that about:
3% of patients with nodular thyroid disease:
Will have an increased serum calcitonin level when measured by a sensitive immunometric assay:
40% of these patients will have MTC at thyroidectomy
However, routine measurement of the basal serum calcitonin concentration is not recommended by the NCCN Panel for evaluating a patient with nodular thyroid disease because of:
The expense of screening all thyroid nodules and only finding a few cases of MTC
The lack of confirmatory pentagastrinstimulation testing
The resulting need for thyroidectomy in some patients who have benign thyroid disease
The ATA is:
Equivocal about routine calcitonin measurement
Inherited MTC:
For patients in known kindreds with inherited MTC:
Prospective family screening with testing for mutant RET genes:
Can identify disease carriers long before clinical symptoms or signs are noted
The traditional approach of stimulating secretion of calcitonin:
By either pentagastrin or calcium infusion to identify patients with MTC:
Is no longer recommended:
Because elevated calcitonin is not a specific or adequately sensitive marker for MTC and because pentagastrin is no longer available in the United States
When MEN2A is suspected, the NCCN Guidelines recommend measurement of:
Calcium levels with (or without) serum intact parathyroid hormone levels
Compared with sporadic disease, the typical age of presentation for familial disease:
Is the third or fourth decade of life, without gender preference
In patients with MEN2A:
Signs or symptoms of hyperparathyroidism or pheochromocytoma rarely present before those of MTC, even in the absence of screening
All familial forms of MTC and MEN2 are:
Inherited in an autosomal-dominant fashion
Mutations in the RET proto-oncogene:
Are found in at least 95% of kindreds with MEN2A and 88% of cases of familial MTC
The RET proto-oncogene codes for:
A cell membrane-associated tyrosine kinase receptor for a glial, cell line-derived neurotrophic factor
Mutations associated with MEN2A and familial MTC:
Have been primarily identified in several codons of the cysteine-rich extracellular domains of:
Exons 10, 11, and 13
MEN2B and some familial MTC mutations are found within the:
Intracellular exons 14 to 16
Somatic mutations in exons 11, 13, and 16 have also been found:
In at least 25% of sporadic MTC tumors:
Particularly the codon 918 mutation:
That activates the tyrosine kinase function of the receptor and are associated with poorer prognosis of the patient
About 6% of patients with clinically sporadic MTC:
Carry a germline mutation in RET:
Leading to identification of new kindreds with multiple (previously undiagnosed) affected individuals
Germline testing for RET proto-oncogene mutations with genetic counseling by a physician or genetic counselor:
Is recommended for all patients with newly diagnosed clinically apparent sporadic MTC:
If a germline RET mutation is found:
Then mutation testing should also be done for family members
MTC can involve difficult ethical decisions for clinicians:
If parents or guardians refuse screening and /or treatment for children with possible MTC
The generally accepted preoperative workup includes:
Measurement of serum markers:
Basal serum calcitonin and serum carcinoembryonic antigen [CEA]
Screening of patients with germline RET proto-oncogene mutations for:
Pheochromocytoma (MEN2A and MEN2B):
Before surgery for MTC:
It is important to diagnose and address coexisting pheochromocytoma, to avoid hypertensive crisis during surgery:
Pheochromocytoma can be removed using laparoscopic adrenalectomy
Hyperparathyroidism (MEN2A)
Preoperative thyroid and neck ultrasound (including central and lateral neck compartments) is recommended
Contrast-enhanced CT of neck / chest and liver MRI or 3-phase CT of liver can be considered as clinically indicated:
Such as in cases of:
High burden of disease
Calcitonin greater than 400 pg/mL
Elevated CEA levels
Distant metastasis:
Does not contraindicate surgery
Liver imaging is rarely needed:
If the calcitonin is less than 400 pg/mL
Evaluation of vocal cord mobility can also be considered:
For patients with:
Abnormal voice, surgical history involving the recurrent laryngeal or vagus nerves, invasive disease, or bulky disease of the central neck
Staging:
The NCCN Guidelines for Thyroid Carcinoma:
Do not use TNM stages to guide therapy:
Instead, many characteristics of the tumor and patient play important roles in these NCCN Guidelines:
Many specialists in thyroid cancer also follow this paradigm
The TNM criteria for clinicopathologic tumor staging are based on:
Tumor size
The presence or absence of extrathyroidal invasion
Locoregional nodal metastases
Distant metastases
The 8th edition of the AJCC Cancer Staging Manual separated MTC into its own stand-alone chapter:
However, the TNM staging classification lacks other important prognostic factors:
Notably absent is the age at diagnosis:
Patients younger than 40 years at diagnosis have a:
5- and 10-year disease-specific survival rate of about 95% and 75%, respectively, compared with 65% and 50% for those older than 40 years
Controlling for the effect of age at diagnosis:
The prognosis of patients with inherited disease (who typically are diagnosed at an earlier age):
Is probably similar to those with sporadic disease
Despite an even younger typical age at diagnosis, however:
Patients with MEN2B who have MTC:
Are more likely than those with MEN2A (or familial MTC) to have:
Locally aggressive disease
Other factors that may be important for predicting a worse prognosis include:
The heterogeneity and paucity of calcitonin immunostaining of the tumor
A rapidly increasing CEA level:
Particularly in the setting of a stable calcitonin level
Postoperative residual hypercalcitoninemia
A study comparing different staging systems found that a system incorporating:
Age, gender, and distant metastases (EORTC):
Had the greatest predictive value:
However, the AJCC staging system was deemed to be the most appropriate
Codon analysis:
Is useful for predicting prognosis
Presence of an exon 16 mutation:
Either within a sporadic tumor or associated with MEN2B:
Is associated with more aggressive disease
More than 95% of patients with MEN2B:
Have a mutation in exon 16 (codon 918)
Whereas 2% to 3% have a mutation in:
Exon 15 (codon 883)
Surgical Management:
Surgery is the main treatment for MTC
While no curative systemic therapy for MTC is available:
Vandetanib and cabozantinib are recommended for:
Locally advanced and metastatic MTC
MTC cells do not concentrate RAI:
Therefore, iodine-131 imaging cannot be used, and RAI treatment is not effective in these patients
MTC does not respond well to conventional cytotoxic chemotherapy
Postoperative levothyroxine is indicated for all patients:
However, TSH suppression is not appropriate:
Because C cells lack TSH receptors:
Thus, TSH should be kept in the normal range by adjusting the levothyroxine dose
Patients should be assessed for hyperparathyroidism and pheochromocytoma preoperatively:
Even in patients who have apparently sporadic disease:
Because the possibility of MEN2 should dictate testing for a germline RET proto-oncogene mutation for all patients with MTC
Pheochromocytomas should be removed (eg, laparoscopic adrenalectomy) before surgery on the thyroid:
To avoid hypertensive crisis during surgery
Patients with pheochromocytomas must be treated preoperatively with:
Alpha-adrenergic blockade (phenoxybenzamine) or with alpha-methyltyrosine:
To avoid a hypertensive crisis during surgery
Forced hydration and alpha-blockade:
Are necessary to prevent hypotension after the tumor is removed
After institution of alpha-blockade and hydration:
Beta-adrenergic blockade may be necessary to treat tachyarrhythmia
Total thyroidectomy and bilateral central neck dissection (level VI):
Are indicated in all patients with MTC:
Whose tumor is 1 cm or larger
Who have bilateral thyroid disease
Total thyroidectomy is recommended and neck dissection can be considered for:
Those whose tumor is smaller than 1 cm
For unilateral thyroid disease
Given the risks of thyroidectomy in very young children:
Referral to a surgeon and team with experience in pediatric thyroid surgery is advised
If a patient with inherited disease is diagnosed early enough:
The recommendation is to perform a prophylactic total thyroidectomy:
By age 5 years or
When the mutation is identified (in older patients), especially in patients with:
Codon 609, 611, 618, 620, 630, or 634 RET mutations:
Note that C634 mutations:
Are the most common mutations
Total thyroidectomy is recommended in:
The first year of life or at diagnosis for patients with:
MEN2B who have codon 883 RET mutations, 918 RET mutations, or compound heterozygous (V804M + E805K, V804M + Y806C, or V804M + S904C) RET mutations:
Because these RET mutations carry the highest risk for MTC
However, for patients with codon 768, 790, 791, 804, and 891 RET (risk level A) mutations:
The lethality of MTC may be lower than with other RET mutations:
In patients with these less high-risk (ie, lower-risk level A) RET mutations:
Annual basal calcitonin testing and annual ultrasound are recommended
Total thyroidectomy and central node dissection may be deferred:
If these tests are normal
There is no family history of aggressive MTC
The family agrees to defer surgery
Delaying thyroidectomy may also be appropriate for children with lower-risk mutations (ie, level A):
Because of the late onset of MTC development
A study found no evidence of persistent or recurrent MTC 5 years or more after prophylactic total thyroidectomy;
In young patients with RET mutations for MEN2A:
Longer follow-up is necessary to determine if these patients are cured
Variations in surgical strategy for MTC depend on:
The risk for locoregional node metastases and on
Whether simultaneous parathyroid resection for hyperparathyroidism is necessary
A bilateral central neck dissection (level VI):
Can be considered for all patients with MEN2B
For those patients with MEN2A who undergo prophylactic thyroidectomy:
Therapeutic ipsilateral or bilateral central neck dissection (level VI) is recommended:
If patients have an increased calcitonin or CEA test or
If ultrasound shows a thyroid or nodal abnormality
Similarly, more extensive lymph node dissection (levels II–V) is considered for:
These patients with primary tumor(s) 1 cm or larger in diameter (> 0.5 cm for patients with MEN2B) or for patients with central compartment lymph node metastases
With a concurrent diagnosis of hyperparathyroidism in MEN2A or familial MTC:
The surgeon should leave or autotransplant the equivalent mass of one normal parathyroid gland if multiglandular hyperplasia is present
Cryopreservation of resected parathyroid tissue should be considered to allow future implantation in the event of iatrogenic hypoparathyroidism
Disfiguring radical node dissections:
Do not improve prognosis and are not indicated
In the presence of grossly invasive disease:
More extended procedures with resection of involved neck structures may be appropriate:
Function-preserving approaches are preferred
In some patients, MTC is diagnosed after thyroid surgery:
In these patients, additional workup is recommended:
To ascertain whether they have RET proto-oncogene mutations (eg, exons 10, 11, 13–16):
Which will determine whether they need additional surgery (eg, completion thyroidectomy and/or neck dissection)
Adjuvant RT EBRT and IMRT:
Have not been adequately studied as adjuvant therapy in MTC:
Slight improvements in local disease-free survival have been reported after EBRT for selected patients:
Such as those with:
Extrathyroidal invasion or
Extensive locoregional node involvement
However, most centers do not have extensive experience with adjuvant EBRT or IMRT for this disease
While therapeutic EBRT or IMRT may be considered for grossly incomplete resection:
When additional attempts at surgical resection have been ruled out:
Adjuvant EBRT or IMRT is rarely recommended
EBRT or IMRT can also be given to palliate painful or progressing bone metastases
Persistently Increased Calcitonin:
Basal serum concentrations of calcitonin and CEA:
Should be measured 2 or 3 months postoperatively
About 80% of patients with palpable MTC and 50% of those with nonpalpable but macroscopic MTC:
Who undergo supposedly curative resection:
Have serum calcitonin values indicative of residual disease:
Those patients with residual disease may benefit from further evaluation to detect either residual resectable disease in the neck or the presence of distant metastases
Patients with detectable basal calcitonin or elevated CEA:
Who have negative imaging and who are asymptomatic:
May be followed
Patients with a basal serum calcitonin value greater than 1000 pg/mL and with no obvious MTC in the neck and upper mediastinum:
Probably have distant metastases:
Most likely in the liver
However, occasionally patients have relatively low serum CEA and calcitonin levels:
But have extensive metastatic disease:
Initial postoperative imaging is therefore reasonable despite the absence of very high serum markers
The prognosis for patients with postoperative hypercalcitoninemia:
Depends primarily on:
The extent of disease at the time of initial surgery
In a study of 31 patients (10 patients with apparently sporadic disease, 15 patients with MEN2A, and 6 patients with MEN2B):
The 5- and 10-year survival rates were 90% and 86%, respectively
Two studies have reported higher mortality rates for patients with high postoperative serum calcitonin values:
With more than 50% of patients having a recurrence during a mean follow-up of 10 years
Routine lymphadenectomy or excision of palpable tumor:
Generally fails to normalize the serum calcitonin concentrations in such patients:
Therefore, some have focused on detection and eradication of microscopic tumor deposits with a curative intent in patients without distant metastases
Extensive dissection to remove all nodal and perinodal tissue from the neck and upper mediastinum:
Was first reported to normalize the serum calcitonin levels in 4 of 11 patients at least 2 years postoperatively
In subsequent larger studies, 20% to 40% of patients undergoing microdissection of the central and bilateral neck compartments:
Were biochemically cured, with minimal perioperative morbidity
When repeat surgery is planned for curative intent:
Preoperative assessment should include locoregional imaging (ie, ultrasonography of the neck and upper mediastinum) and attempts to exclude patients with distant metastases, which may include:
Contrast-enhanced CT or MRI of the neck, chest, and abdomen
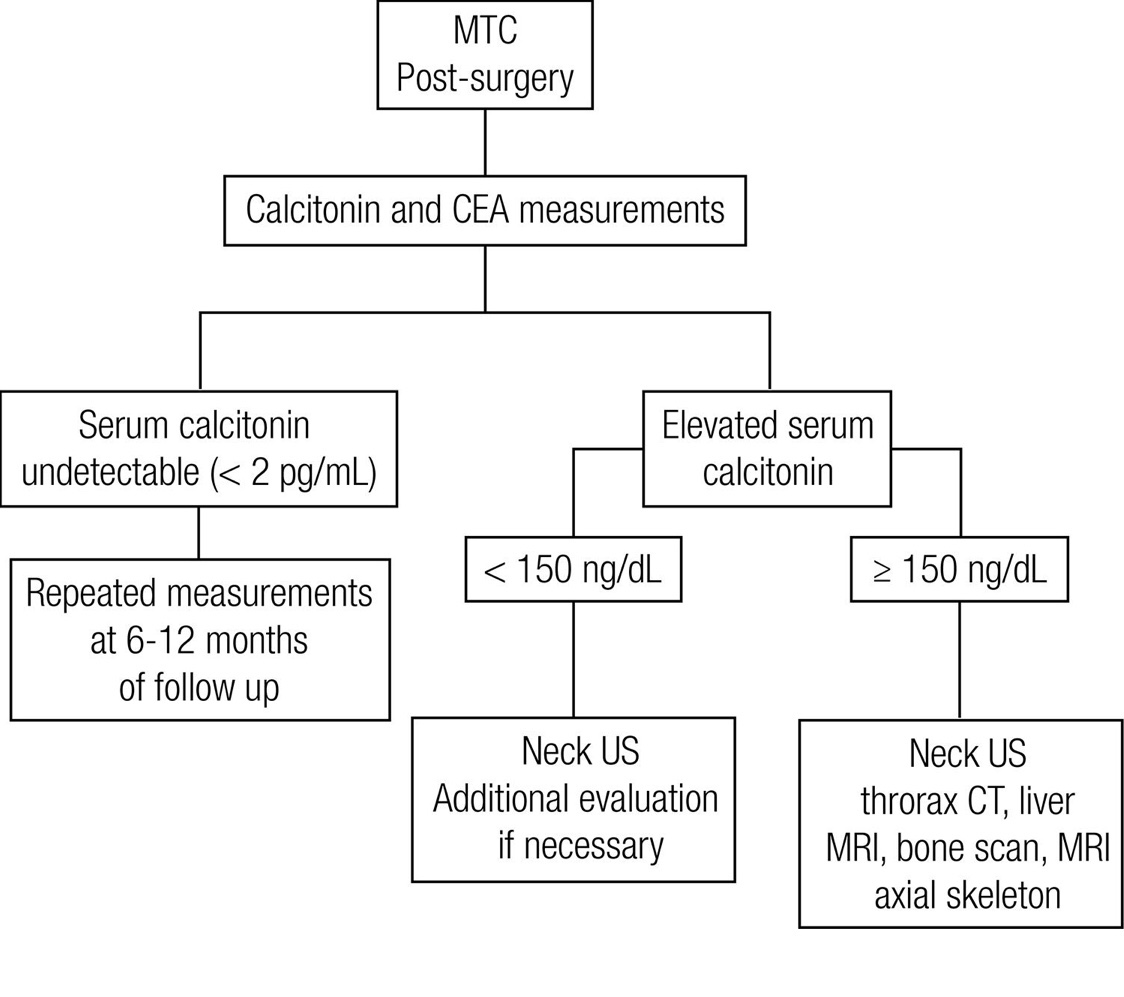
Postoperative Management and Surveillance:
Calcitonin is very useful for surveillance:
Because this hormone is only produced in the parafollicular cells
Thus, measurements of serum calcitonin and CEA levels:
Are the cornerstone of postoperative assessment for residual disease
For patients with a detectable basal calcitonin or elevated CEA level:
Neck ultrasound is recommended
Patients with undetectable calcitonin levels and normal CEA levels:
Can subsequently be followed with annual measurements of serum markers
Additional studies or more frequent testing:
Can be done for those with significantly rising calcitonin or CEA
Nonetheless, the likelihood of significant residual disease is very low in patients with an undetectable basal calcitonin level in a sensitive assay
If the patient has MEN2:
Annual screening for pheochromocytoma (MEN2B or MEN2A) and hyperparathyroidism (MEN2A):
Should also be performed
For some low-risk RET mutations:
Examples:
Codons 768, 790, 804, or 891:
Less frequent screening may be appropriate
Patients with detectable serum markers:
Calcitonin levels ≥ 150 pg/mL:
Should have CT of the neck, chest, and liver
Bone scan and MRI of axial skeleton:
Should be considered in select patients such as those with very elevated calcitonin levels
The NCCN Panel recognizes that many different imaging modalities may be used to examine for residual or metastatic tumor:
But there is insufficient evidence to recommend any particular choice or combination of tests
For patients with asymptomatic disease and detectable markers in whom imaging fails to identify foci of disease:
The NCCN Panel recommends conservative surveillance:
With repeat measurement of the serum markers every 6 to 12 months
Additional imaging studies (eg, FDG PET/CT, Ga68 DOTATATE, or MRI with contrast of the neck, chest, and abdomen with liver protocol):
May be indicated depending on calcitonin / CEA doubling time
For patients who are asymptomatic with abnormal markers and repeated negative imaging:
Continued disease monitoring or consideration of cervical reoperation is recommended if primary surgery was incomplete
For the patient with increasing serum markers:
More frequent imaging may be considered
Outside of clinical trials:
No therapeutic intervention is recommended on the basis of abnormal markers alone
Introduction:Medullary thyroid cancer (MTC):Is a neuroendocrine tumor of the parafollicular or C cells of the thyroid gland:MTC accounts for:Approximately 1% to 2% of all thyroid cancers in the United States:
The production of calcitonin:Is a characteristic feature of this tumor
Most medullary thyroid carcinomas:Are sporadic (75% to 80%):However:Approximately 20% to 25% are familial:As part of the multiple endocrine neoplasia type 2 (MEN2) syndrome
Clinical Presentation:Sporadic MTC:Sporadic medullary thyroid cancer (MTC):Accounts for approximately 75% of all cases of the disease:The typical age of presentation:Is in the fourth and sixth decades of lifeSymptoms and signs:The most common presentation of sporadic MTC:Is that of a solitary thyroid nodule:Which occurs in 75% to 95% percent of patientsThe C cells or parafoliccular cells are predominantly located in the upper portion of each thyroid lobe:Thus:Most tumors are located in this region
In most patients with MTC:The disease has already metastasized at the time of diagnosis:Approximately 70% of patients have clinically detectable cervical lymph node involvementUp to 15% of patients with MTC:Have symptoms of upper aerodigestive tract compression or invasion:Such as dysphagia or hoarseness
Approximately 5% to 10%:Have distant metastatic disease:Distant metastases may occur in the:Liver, lung, bones, and, less often, brain and skin
Nodal metastases:Are more common in patients with multifocal disease:However, as calcitonin screening results in the identification of more “micro” medullary cancers:The number of patients with metastases at presentation appears to be decreasing
Calcitonin screening for MTC in patients with thyroid nodules is controversial
Systemic symptoms may occur due to hormonal secretion by the tumor:Tumor secretion of calcitonin, calcitonin gene-related peptide, or other substance:Can cause diarrhea or facial flushing in patients with advanced diseaseIn addition, occasional tumors secrete corticotropin (ACTH):Causing ectopic Cushing’s syndrome
Biochemical tests:Basal serum calcitonin concentrations:Usually correlate with tumor mass but also reflect tumor differentiation, and they are almost always high in patients with a palpable tumorMost MTCs also secrete carcinoembryonic antigen (CEA):Which, like calcitonin, can be used as a tumor markerIn addition, the expression of CEA on MTC cells has led to the use of anti-CEA antibodies for immunotherapy
Thyroid function tests are normal in patients with MTC
Imaging:There are several ultrasound features of thyroid nodules (eg, hypoechoic, microcalcifications) that are associated with thyroid cancer risk:However, there are no ultrasound features that are pathognomonic for thyroid cancer.
Furthermore, the majority of studies evaluating suspicious ultrasound characteristics of nodules focused on papillary thyroid cancer
In a small retrospective study examining the ultrasound characteristic of nodules that were histologically proven to be MTC and papillary thyroid cancer50% of MTCs were solid and hypoechoic16% showed microcalcificationsCompared with 69.2% and 69.2%:Respectively, for papillary thyroid cancers The presence of at least one suspicious ultrasound feature was almost equal in patients with MTC (58.3%) and controls with benign nodules (55.5%), whereas it was significantly more frequent in patients with papillary thyroid cancer (100%)
In other seriesHypoechogenicity was present in 50% to 89% and microcalcifications in 30% to 70%:There was no difference in echogenicity or the presence or type of calcifications between MTC and papillary thyroid cancer . Large areas of calcification (macrocalcification) were noted in 16% to 30%:Rarely:The diagnosis of MTC is suggested by the presence of dense calcifications seen on radiographs or imaging of the anterior neck.
Inherited MTC:Multiple endocrine neoplasia type 2 (MEN2):Is subclassified into two distinct syndromes (MEN2A and MEN2B):Each of which is transmitted in an autosomal dominant fashion and is associated with MTC
These syndromes result from:Different mutations in the RET proto-oncogene
In the past:Familial MTC (FMTC):An inherited syndrome characterized by the presence of only MTCwithout hyperparathyroidism or pheochromocytoma:Was considered a separate entity but is now considered a variant of MEN2A
Hereditary MTC is:Typically bilateral and multicentric:Classical MEN2A is associated with: MTC
Pheochromocytoma
Primary parathyroid hyperplasiaWhile the penetrance of MTC is nearly 100%:There is inter- and intrafamily variability in the specific pattern of the other disease manifestations
MEN2B shares the inherited predisposition to MTC and pheochromocytoma present in classical MEN2A:But does not include hyperparathyroidismMTC occurs in almost all patients
The tumor develops at:An earlier age and may be more aggressive than in MEN2A
Patients typically have:A marfanoid habitus (but do not have Marfan syndrome),Mucosal neuromas
Intestinal ganglioneuromatosis
In the index case:The clinical presentation and manifestations of MEN2-associated MTC are similar to those of sporadic MTC:The most common presentation is that of:;A solitary thyroid nodule or cervical lymphadenopathyEarly diagnosis (prior to any clinical manifestations) by screening of “at-risk” family members in MEN2 kindreds is important because MTC is a life-threatening disease that can be cured or prevented by early thyroidectomy
What is Head and Neck Surgery?:
It is a surgical sub-specialty that deals mainly with benign and malignant tumors of the head and neck region, including:
The scalp, facial region, eyes, ears, nose, nasal fossae, paranasal sinuses, oral cavity, pharynx (nasopharynx, oropharynx, hypopharynx), larynx (supraglotic larynx, glottis larynx, subglotic larynx), thyroid gland, parathyroid gland, salivary glands (parotid glands, submandibular glands, sublingual glands, minor salivary glands), soft tissues of the neck, skin of the head and neck region.
The head and neck surgeon’s work area:Does not cover tumors or diseases of the brain and other areas of the central nervous system or those of the cervical spine:This is the neurosurgeon field.
Among the diagnostic procedures performed by the head and neck surgeon, are the following:
Nasopharyngolaryngoscopy:
Performed to examine, evaluate and, possibly perform a biopsy, of oral cavity, pharyngeal and laryngeal lesions.
The surgeries most commonly performed by the head and neck surgeon are:
Total or near total thyroidectomies
Hemithryoidectomies (lobectomies)
Comprehensive neck dissections
Selective neck dissections
Maxillectomies:
Total maxillectomy
Subtotal maxillectomy
Infrastructure maxillectomy
Suprastructure maxillectomy
Medial maxillectomy
Mandibulectomy:
Segmental
Marginal
Tracheostomy
Salivary gland surgeries:
Parotid gland operations:
Limited superficial parotidectomy with identification and preservation of the facial nerve
Superficial parotidectomy with identification and preservation of the facial nerve
Near total parotidectomy with identification and preservation of the facial nerve
Total parotidectomy
Submandibular gland resection
Sublingual gland resection
Resection of tumors of the oral cavity:
Glossectomy
Resection of the floor of the mouth tumors
Resection of tumors of the pharynx
Resection of tumors of the larynx
Split-thickness skin grafts
Full-thickness skin grafts
Sentinel lymph node mapping and sentinel lymph node biopsy
Resection of malignant skin tumors (BCC, SCC, melanoma) of the head and neck region
The formation of the head and neck surgeon includes mastering the following subjects:
Surgical Anatomy
History and Basic Principles of Head and Neck Surgery
Epidemiology, Etiology, and Pathology of Head and Neck Diseases
Diagnostic Radiology of the Head and Neck Region
Tumors of the Scalp, Skin and Melanoma
Eyelids and Orbit
Nasal Cavity and Paranasal Sinuses
Skull Base and Temporal Bone
Lips and Oral Cavity
Pharynx and Esophagus
Larynx and Trachea
Cervical Lymph Nodes
Thyroid and Parathyroid Glands
Salivary Glands
Neurogenic Tumors and Paragangliomas
Soft Tissue Tumors
Bone Tumors and Odontogenic Lesions
Reconstructive Surgery
Oncologic Dentistry and Maxillofacial Prosthetics
Principles of Radiation Oncology
Principles of Chemotherapy
Molecular Oncology, Genomics and Immunology
Nutrition
Biostatistic
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon / endocrine surgeon / surgical oncologist and is a member of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center in Mexico City:
Rodrigo Arrangoiz MS, MD, FACS:
Is a member of the American Head and Neck Society
He is a member of the American Thyroid Association:
Training:
• General surgery:
• Michigan State University:
• 2004 al 2010
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012
• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
In the United States, MTCs represent 1% to 2% of all thyroid malignancies, with a slight preponderance in women
MTC originates from parafollicular calcitonin-producing cells (C- cells)
Approximately 75% to 80% of cases are sporadic:
While hereditary forms such as multiple endocrine neoplasia (MEN) type 2A or 2B account for almost 20% to 25% of cases
The 10-year survival rates of MTC are estimated at 81% to 89%
Calcitonin is a specific tumor marker for MTC:
Although the routine use of serum calcitonin measurements for the preoperative assessment of thyroid nodules is still controversial, according to current guidelines
The aim of this study was to assess serum calcitonin cutoff levels in patients undergoing surgery for benign and malignant thyroid disease in Germany and Austria
A second goal was to assess the potential correlations between serum calcitonin levels and size of the resected MTCs, the presences of lymph node metastases, and the time to biochemical normalization
Methods:
The cohort was obtained from the German DGAV/StuDoQ registry, which is a prospective, multi-center database that includes data on the surgical treatment of benign and malignant thyroid disease, as well as hyperparathyroidism
All patients with thyroid surgery documented in the registry between March 2017 and September 2020 were included
Data regarding subject demographics, preoperative and postoperative serum calcitonin levels, the diagnosis of C-cell hyperplasia or MTC, surgical procedures, histopathology, and biochemical cure rates were recorded
C-cell hyperplasia was defined as the presence of > 50 microscopically calcitonin-positive cells in at least one low-power field and considered to be a benign thyroid pathology
Biochemical recovery of MTC was defined by serum calcitonin levels below 10 pg/ml postoperatively (timepoint unspecified)
The study also assessed sex-specific calcitonin cutoff levels
The tumor size and the presence of lymph node metastases predicting biochemical recovery of calcitonin levels were analyzed by univariate and multivariate logistic regression
Results:
Total thyroidectomy was performed in 93% of the patients
MTC was diagnosed in 1.2%, and the mean (±SD) tumor diameter was 14.7±12.43 mm (range, 1–80)
Histopathology of MTCs revealed that 173 ± 48.4% were pT1a, 100±28.0% pT1b, 65±18.2% pT2, 17±4.8% pT3, and 2±0.6% pT4
Preoperative calcitonin screening was available in 92.4% of the data set
Of the 29,054 patients without C-cell hyperplasia or MTC:
The median preoperative calcitonin level was 2.0 pg/ml, and calcitonin levels were marginally higher in those with coexisting renal hyperparathyroidism than in those without
In the 206 patients with C-cell hyperplasia:
The median calcitonin level was 16.1 pg/ml (range, 1–183.3)
There were 330 patients with MTC:
In whom the median calcitonin level was 168.0 pg/ml, with men having higher calcitonin levels than women
Both female and male patients with C-cell hyperplasia or MTC:
Demonstrated significantly higher calcitonin levels than those with benign thyroid disease
Using receiver operating characteristic (ROC) analysis:
The serum calcitonin thresholds for predicting MTC were 7.9 pg/ml in women and 15 pg/ml in men (P<0.001)
The tumor size of MTC was positively correlated with median calcitonin levels:
Tumor diameters of 6 to 10 mm had a median calcitonin level of 81 pg/ml (range, 10.6–2000), tumors with diameters between 3 and 5 mm 31 pg/ml (range, 1–5890), and tumors smaller than 3 mm 13 pg/ml (range, 0-187.8)
Single lymph node metastases were detected at a median calcitonin level of 256 pg/ml (range, 23–2740), which increased to 3012 pg/ml (range, 825–4410) in patients with more than 21 metastatic lymph nodes
The median calcitonin level in those with metastatic MTC was 7025 pg/ml (range, 1538–85,800)
In 71.4% of patients with MTC, biochemical normalization of serum calcitonin levels was achieved after thyroid surgery:
With higher rates seen in those with hereditary MTCs than in those with sporadic forms
Overall, biochemical cure was achieved in:
90% of pT1a tumors, 66.7% of pT1b tumors, 48.7% of pT2 tumors, and 25% of pT3 tumors, but calcitonin normalization was not significantly correlated with tumor size
Conclusions:
Preoperative serum calcitonin levels of > 7.9 pg/ml in women and >15 pg/ml in men should be regularly monitored and considered for the diagnosis of MTC, particularly in patients with increasing serum calcitonin levels or sonographically suspicious thyroid nodules
It is well established that the early diagnosis and surgical treatment of MTC significantly improve the outcomes of this disease
The routine measurement of serum calcitonin in patients with thyroid nodules is still controversial in the United States; the latest guidelines from the American Thyroid Asso-ciation do not recommend it as a routine screening test
In contrast, several European countries have implemented the preoperative measurement of serum calcitonin to improve the diagnosis of MTC
During the beginning of the COVID-19 pandemic, restrictions for outpatient procedures were implemented across institutions in the United States
In the Phoenix Veteran Administration Hospital, they implemented a protocol for thyroid nodules that included serum calcitonin as a surrogate marker for the potential diagnosis of MTC
Recommendations are emergent fine-needle aspiration (FNA) in patients with serum calcitonin levels >10 pg/ml
In patients with calcitonin levels > 100 pg/ml, thyroid surgery was recommended
The strengths of this study include its large sample size, multicenter cohort, and long follow-up (mean duration, 3.5 years)
In addition, the establishment of a sex-specific serum calcitonin cutoff is useful for clinicians
However, limitations include the use of different calcitonin assays among the various centers and missing data regarding the use of proton-pump inhibitors, renal function, and liver cirrhosis, all of which may falsely increase calcitonin levels
In summary, the evidence provided by this study suggests that routine serum calcitonin screening in patients with thyroid nodules allows earlier diagnosis and improves the prognosis of MTC, particularly in those with smaller tumor sizes and less lymph node involvement
Although the cost-effectiveness of such a strategy is an important factor, the practice should be considered in our thyroid clinics across the United States
Which are neural crest derivatives and produce a variety of biogenic amines, including:
Calcitonin and carcinoembryonic antigen (CEA):
Used as tumor markers
MTC:
Represents up to 2% to 4% of thyroid cancer cases
Accounts for about 14% of all thyroid cancer related deaths
MTC can be:
Sporadic (or acquired via somatic mutation):
In 75% of the cases
Hereditary (or familial via germline mutation):
In the remaining 25%:
With the latter comprising the polyglandular cancer syndrome:
Known as multiple endocrine neoplasia 2 (MEN2): types A and B
The RET oncogene:
Is the most common genetic alteration in MTC:
Being present in 100% of MEN2 syndromes and in about 45% of sporadic MTC
Mutually exclusive point mutations of RAS has been reported in sporadic MTC:
But with less frequency (approximately 15%),
The remainder cases of sporadic MTC:
Do not have identifiable mutations
Many patients are diagnosed incidentally in the absence of symptoms:
Although some may experience compressive symptoms, diarrhea, and / or flushing
MTC is initially diagnosed by:
US-guided fine-needle aspiration (FNA) biopsy of a thyroid nodule
There are no distinctive ultrasound features between MTC and a follicular-derived thyroid cancer:
Hence, cytology findings suggestive of MTC should be further assessed with immunohistochemistry
MTC stains positive for:
Calcitonin, chromogranin, and CEA, and negative for thyroglobulin
The advent of molecular genetic testing for thyroid nodules has significantly improved diagnosis among indeterminate FNA samples
After a cytological diagnosis of MTC (prior to surgery):
The serum calcitonin and CEA levels should be measured:
Followed by a genetic testing for a RET germline mutation
All patients with MTC should undergo genetic testing because up to 7% of apparent sporadic MTC:
Are indeed de-novo hereditary mutations:
Meaning not inherited from either parent
In addition, up to 75% of patients with MEN2B have a de-novo germline RET mutation
It is important that pediatricians, primary care providers, and dentists be able to recognize the characteristic MEN2B body features:
Including a marfanoid body habitus, eye abnormalities (thickened and everted eyelids and inability to produce tears), mucosal neuromas in the eyelids and aerodigestive tract (visible in the lips, tongue, nostrils), and diffuse ganglioneuromas of the gastrointestinal tract:
Leading to chronic constipation, abdominal pain, and possible intestinal obstruction
Total thyroidectomy with cervical lymph node dissection is the standard treatment:
Unfortunately, there is only a 10% cure rate when cervical lymph nodes are involved at the time of initial surgery
Post-operative levothyroxine:
Should be administered to maintain euthyroidism, and radioactive iodine treatment is not indicated
For persistent locoregional and / or distant metastases:
Repeat surgery, external beam radiation, or other focal therapies can be implemented
When these therapies are no longer options due to progressive or symptomatic disease:
Systemic therapy should be considered:
There are 4 FDA approved kinase inhibitors for MTC
The non-selective multi-kinase inhibitors:
Vandetanib and cabozantinib:
Were the first drugs approved for MTC
The selective RET-inhibitors:
Selpercatinib and pralsetinib:
Were approved in 2020 and may be used as first or subsequent lines of therapy for RET mutated MTC
New treatments with immunotherapy, tumor vaccines, peptide receptor radionuclide therapy (PRRT) are being studied in clinical trials for MTC
References:
Wells SA, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid 2015; 25: 567–610.
Roman S, Lin R, Sosa JA. Prognosis of medullary thyroid carcinoma: demographic, clinical, and pathologic predictors of survival in 1252 cases. Cancer 2006; 107: 2134–2142.
Wirth LJ, Waguespack SG, Busaidy NL, et al. Genomic landscape of FNAs positive for medullary thyroid cancer (MTC) and potential impact on systemic therapy. JCO 2019; 37: 6087–6087.
Hu MI, Waguespack SG, Dosiou C, et al. Afirma Genomic Sequencing Classifier and Xpression Atlas Molecular Findings in Consecutive Bethesda III-VI Thyroid Nodules. J Clin Endocrinol Metab 2021; 106: 2198–2207.
Ciarletto AM, Narick C, Malchoff CD, et al. Analytical and clinical validation of pairwise microRNA expression analysis to identify medullary thyroid cancer in thyroid fine-needle aspiration samples. Cancer Cytopathol 2021; 129: 239–249.
Nikiforov YE, Baloch ZW. Clinical validation of the ThyroSeq v3 genomic classifier in thyroid nodules with indeterminate FNA cytology. Cancer Cytopathology 2019; 127: 225–230.
Wells SA, Robinson BG, Gagel RF, et al. Vandetanib in Patients With Locally Advanced or Metastatic Medullary Thyroid Cancer: A Randomized, Double-Blind Phase III Trial. JCO 2012; 30: 134–141.
Elisei R, Schlumberger MJ, Müller SP, et al. Cabozantinib in Progressive Medullary Thyroid Cancer. JCO 2013; 31: 3639–3646.
Wirth LJ, Sherman E, Robinson B, et al. Efficacy of Selpercatinib in RET -Altered Thyroid Cancers. N Engl J Med 2020; 383: 825–835.
Subbiah V, Hu MI, Wirth LJ, et al. Pralsetinib for patients with advanced or metastatic RET-altered thyroid cancer (ARROW): a multi-cohort, open-label, registrational, phase 1/2 study. The Lancet Diabetes & Endocrinology; 0. Epub ahead of print 9 June 2021. DOI: 10.1016/S2213-8587(21)00120-0.
Liu C-Q, Shen C-K, Du Y-X, et al. Survival outcome and optimal candidates of primary tumor resection for patients with metastatic medullary thyroid cancer. J Clin Endocrinol Metab 2024;109(11):2979-2985; doi: 10.1210/clinem/dgae214. PMID: 38570918.
Background:
Medullary thyroid cancer (MTC):
Is a rare malignancy with high metastatic potential
Distant metastases are present in 10% of patients at diagnosis and portend an overall poor prognosis:
With 10-year survival rates below 50%
Complete surgical excision of the primary tumor, including lymph nodes:
Is the only curative strategy for localized MTC:
However, limited data exist on the potential benefit of primary tumor resection (PTR) on survival in people with distant metastases at diagnosis
This study aimed to leverage a population-based registry to:
Assess the prognostic significant of site-specific metastasis and number of metastases
Evaluate survival outcomes of patients with metastatic MTC who underwent PTR
Identify the optimal candidates for PTR in patients with metastatic MTC
Methods:
This study analyzed the Surveillance, Epidemiology, and End Results (SEER) database:
Between 2010 and 2020 for patients with MTC who had distant metastasis at diagnosis
Key variables extracted included demographics (age, gender), tumor characteristics (grade, size, metastatic site), and treatment details (PTR, neck dissection, radiation, and chemotherapy)
The SEER database exclusively provides data on five metastatic sites: lung, bone, liver, brain, and distant lymph nodes
Patients were divided into PTR and non-PTR groups, and survival outcomes (overall survival [OS] and cancer-specific survival [CSS]) were analyzed using Kaplan–Meier curves and log-rank tests
Cox regression models were used to identify independent prognostic factors
Results:
The most common metastatic sites in the 186 patients (median age, 56 years; range, 8 to 89) included in this study were:
Bone (45.7%)
Liver (39.8%)
Lung (36.6%)
Brain metastasis (n = 10, 5.4%):
Was associated with significantly poorer:
OS (P = 0.0007) and CSS (P = 0.0013):
As compared to other metastatic sites
Kaplan–Meier analyses found that patients with more metastatic sites had worse CSS (P= 0.026):
However, the number of metastases was not a significant predictor of survival on univariable and multivariable Cox regression
More than half of the cohort (n = 106, 56.5%) underwent PTR
The PTR group had approximately one-third the hazard of overall mortality (HR, 0.29; 95% CI, 0.13–0.64; P = 0.002) and cancer-specific mortality (HR, 0.38; 95% CI, 0.16–0.94; P = 0.036) than the non-PTR group
In subgroup analyses by metastatic site:
PTR was associated with better survival in patients with metastasis to the lung, bone, liver, or distant lymph node (DLN):
But showed no significant difference for those with brain metastasis
In patients who had one or two organs with metastasis:
PTR was associated with improved OS (P< 0.01) and CSS (P < 0.05):
Whereas no survival difference was observed in those who had more than two organs with metastasis
Conclusions:
In patients with MTC and distant metastasis at diagnosis:
Patients who underwent PTR had better OS and CSS than those who did not
No difference in survival with PTR was observed in the small subgroup with:
Brain metastases, who also had a worse prognosis than those with other metastatic sites
The authors conclude that PTR may confer survival benefits in metastatic MTC:
Optimal candidates are those with metastases in one or two organs and those without brain metastases
Summary:
For patients with extensive regional or metastatic MTC:
For whom the goals of care are palliative:
The 2015 American Thyroid Association (ATA) guidelines recommend a personalized approach:
With consideration of neck surgery, radiation and systemic therapies
PTR for patients with distant metastatic MTC is often performed for local control, including with palliative intent:
Given the high mortality and morbidity associated with airway or neck invasion
Tumor debulking:
Can also offer reduction in calcitonin level to improve rates of chronic diarrhea:
However, this contrasts with the traditional treatment of other stage IV neoplasms and has to date lacked randomized prospective data
Using SEER data between 2010 and 2020, this study showed that patients who underwent PTR had better survival outcomes than those who did not
These findings are largely consistent with an earlier analysis of the SEER database capturing cases between 1998 and 2015
A key limitation of this registry-based study is the absence of data on performance status, a putative risk factor for survival and an important predictor of PTR eligibility
Given the retrospective design and lack of adjustment for performance status as a confounder, causality between the role of PTR and survival cannot be established
Additionally, metastatic MTC varies widely in behavior, from indolent to aggressive
Predictors of disease activity such as tumor markers and doubling times of calcitonin and carcinoembryonic antigen were not included in this study owing to registry limitations
The multiple subgroup analyses that aimed to identify optimal candidates for PTR based on metastatic site and number were also largely underpowered
Thus, the authors’ recommendation that PTR should only be considered in those with one or two metastatic organs or those without brain metastases should be interpreted with caution
Notably, these data from 2010 to 2020 largely precede the widespread use of multikinase and selective RET inhibitors:
Which have changed the therapeutic landscape of MTC, and also may alter the role of PTR
Data on RET pathogenic variant status and use of targeted therapies were not captured by the SEER database
The role of RET-targeted kinase inhibitors as neoadjuvant therapy is under active investigation with an ongoing phase II trial on the use of selpercatinib before surgery for RET-altered thyroid cancers
Although we cannot infer a survival benefit from PTR from these retrospective registry-based studies:
These data reassure clinicians to continue recommending PTR in suitable candidates with MTC and distant metastases
Furthermore, although quality of life was not examined in this article, the importance of lowering calcitonin cannot be overstated, as high calcitonin can confer significant morbidity through hormone-mediated chronic diarrhea
As targeted molecular therapy becomes more prevalent, further data will be required to inform the evolving role of PTR in metastatic MTC management
Adjuvant therapy with olaparib vs placebo demonstrated a benefit in overall survival, invasive disease‒free survival, and distant disease‒free survivalin eligible patients with early breast cancer and gBRCApathogenic variants.
With the expanded role of BRCA testing in early breast cancer, completion of testing in eligible patients is critical
Given the survival benefit of adjuvant PARP inhibition in this population:
Patient and healthcare professional education on the importance of genetic testing and benefits of therapy is key
The safety and efficacy of olaparib as adjuvant therapy was evaluated in the phase 3 OlympiA trial:
That enrolled patients with a germline BRCA mutationand HER2 negative, high-risk, early-stage breast cancer:
Who had completed definitive local treatment and at least 6 cycles of neoadjuvant or adjuvant chemotherapy containing anthracyclines, a taxane, or both (prior platinum for previous cancer or as adjuvant /neoadjuvant breast cancer treatment was permitted)
Patients were randomly assigned (1:1) to receive:
Olaparib tablets 300 mg orally twice daily or placebo
Treatment was continued for up to 1 year or until disease recurrence or unacceptable toxicity occurred
In this study, patients with high-risk, early stage breast cancer were identified using the following criteria:
Patients who received prior neoadjuvant chemotherapy:
Triple-negative breast cancer (TNBC):
They needed to have residual invasive cancer in the breast and / or the resected lymph nodes (nonpathologic complete response) at the time of surgery
Hormone receptor–positive breast cancer:
They needed to have residual invasive cancer in the breast and / or the resected lymph nodes (nonpathologic complete response) at the time of surgery:
Additionally, they needed a score of 3 or more based on pretreatment clinical and post-treatment pathologic stage, ER status, and histologic grade (Table)
Patients who received prior adjuvant chemotherapy:
TNBC:
They needed to have node-positive disease or node-negative disease with the primary tumor measuring 2 cm or more
Hormone receptor–positive, HER2 negative breast cancer:
They needed to have 4 or more pathologically-confirmed positive lymph nodes
Early Breast Cancer Stage, Receptor Status, and Grade Scoring Requirements for OlympiA Enrollment
Updated results, representing a median follow up of 3.5 years, were published in October 2022:
A significant improvement in OS was observed in the olaparib group compared to the placebo group:
HR, 0.68; 98.5% CI, 0.47-0.97; P = 0.009:
Four-year OS rates were 89.8% with olaparib and 86.4% with placebo
Continued benefit in terms of invasive disease free survival (IDFS) and distant DFS (DDFS) were demonstrated with olaparib versus placebo
In subset analyses, OS, IDFS, and DDFS benefits were observed across major subgroups
Are associated with an increased risk of breast cancer
The most common involve mutations of the:
BRCA1 and BRCA2 genes
The risk of breast cancer among women with BRCA1 mutations:
Approaches 80%,with ovarian cancer risk as high as 45%
BRCA2 carriers:
Have slightly lower rates of both breast (up to 60%) and ovarian (up to 25%) cancers
Male breast cancers:
Are more likely to be BRCA2 if the man is found to be a gene carrier
Less than half of the hereditary cancers are secondary to non-BRCA genetic mutations
Cowden Syndrome:
Is associated with PTEN mutations and has an autosomal dominance inheritance pattern
Individuals have an increased lifetime risk of:
Breast cancer (20% to 50%):
With most diagnosed before age 50 years
As well as high rates of benign breast disease
Follicular thyroid and endometrial cancers:
Are commonly seen in association with this syndrome as well
Screening includes surveillance of the kidneys and colon, as they are increased in risk for cancers of these organs as well
Peutz-Jeghers syndrome:
Is characterized by mutations in STK11 and also demonstrates autosomal dominant inheritance
Individuals have a breast cancer risk of 55%:
Along with elevated rates of both ovarian and uterine cancer
These individuals often have:
Multiple hamartomatous polyps throughout the gastrointestinal tract:
As well as multiple melanin deposits in the mouth, lips, fingers, and toes
Li-Fraumeni syndrome:
Is characterized by mutations of the TP53:
A suppressor gene and is also inherited in an autosomal dominant pattern
These individuals have strikingly high rates of malignancy:
With 50% of individuals diagnosed with cancer by age 30, and 90% diagnosed with cancer by age 70
Malignancies include:
Breast:
With the majority diagnosed by age 45 years
Sarcomas, osteosarcomas, leukemias, brain tumors, and adrenocortical tumors
Radiation-induced tumors have been seen frequently among these patients:
Leading many radiation oncologists to advise against breast-conservation therapy in women with Li-Fraumeni diagnosed with breast cancers
References:
Economopoulou P, Dimitriadis G, Psyrri A. Beyond BRCA: New hereditary breast cancer susceptibility genes. Cancer Treat Rev. 2015;41:1-8.
Issacs C, Peshkin BN, Schwartz M. Genetic testing and management of patients with hereditary breast cancer diseases of the breast. In: Harris JR, Lippman ME, Morrow M, Osborne CK, eds. Diseases of the Breast. 4th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2010:224-247.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Genetic / Familial High-Risk Assessment: Breast and Ovarian. Available at http://www.nccn.org.
Ready K, Arun B. Breast cancer syndromes: counseling and management. In: Babiera GV, Skoracki RJ, Esteva FJ, eds. Advanced Therapy of Breast Disease. 3rd ed. Shelton, CT: People’s Medical Publishing House-USA; 2012:29-38.