The 15.8% skip metastasis rate reported by Byers et al. (1997):
Is widely considered an overestimate due to several important methodological issues that have been carefully dissected in subsequent literature:
Most notably by Warshavsky et al. in their 2019 JAMA Otolaryngology meta-analysis [1][2]
What Byers Reported:
Byers et al. reviewed 277 previously untreated patients with oral tongue SCC (1970 to 1990):
Who underwent glossectomy and neck dissection
They reported that 15.8% of all patients had either:
Level IV metastasis as the only manifestation of neck disease
Level III as the only positive node without disease in levels I to II
Subsequent level IV recurrence after initial dissection that did not include level IV
Based on this, they recommended routine dissection of levels I to IV for all oral tongue SCC [2]
Why the 15.8% Figure Is Misleading:
Warshavsky et al. performed a careful reanalysis of the Byers data and identified several critical flaws that inflated the rate [1]:
Conflation of skip metastasis definitions:
Byers combined true level IV skip metastasis with level III skip metastasis (level III positive without levels I to II involvement):
These are fundamentally different clinical scenarios — level III disease is already captured by a standard supraomohyoid neck dissection (levels I to III)
By lumping both together, the rate was artificially elevated
Inclusion of neck recurrences as “skip metastases”:
Nine patients (9.9%) who developed level IV recurrences after an initial dissection that did not include level IV were counted toward the 15.8% figure:
As Warshavsky et al. noted, counting neck recurrence as a missed pathological lymph node is problematic because the neck has lost its normal anatomical lymphatic drainage and, in many cases, has been irradiated
This makes it impossible to determine whether these were true skip metastases or recurrences from altered lymphatic flow [1]
True level IV skip metastasis rate was only 5.5%:
When the data are restricted to patients with cN0 disease who had level IV metastasis found in the initial neck dissection specimen (i.e., true pathologic skip metastasis):
The rate drops to 5.5% — roughly one-third of the reported figure [1]
Even the most generous calculation yields only 4.8%:
When accounting for all cases mentioned in the study (both initial pathologic findings and subsequent recurrences), the combined incidence of skip metastasis or subsequent recurrence in level IV was only 4.8% (13 of 270), not 15.8% [1]
Mixed cN0 and cN+ populations:
The study included patients across all clinical N stages, and the data were not clearly stratified by preoperative nodal status, making it difficult to isolate the true elective (cN0) skip metastasis rate
Era of the study (1970 to 1990):
Preoperative imaging was far less sophisticated, meaning some patients classified as cN0 may have had undetected nodal disease, further confounding the results
What Modern Data Shows:
The Warshavsky et al. meta-analysis of 13 studies (1,359 cN0 patients):
Found the true skip metastasis rate to level IV is only 0.50% (95% CI, 0.09%–1.11%):
With an overall level IV involvement rate of 2.53% [1]
Even for oral tongue specifically — the highest-risk subsite:
The level IV involvement rate was 3.60% [1]
A large Tata Memorial audit of 761 early-stage cN0 patients:
Found skip metastasis to level IV in only 0.3% [3]
In summary, the Byers 15.8% figure resulted from a broad definition of “skip” that included level III skips (already addressed by SOHND), conflation of initial pathologic findings with subsequent recurrences, and lack of stratification by preoperative nodal status:
Modern evidence overwhelmingly supports that true skip metastasis to level IV in cN0 oral tongue SCC is a rare event (~0.5%), and supraomohyoid neck dissection (levels I to III) remains adequate for the elective setting
References:
1. Assessment of the Rate of Skip Metastasis to Neck Level IV in Patients With Clinically Node-Negative Neck Oral Cavity Squamous Cell Carcinoma: A Systematic Review and Meta-analysis. Warshavsky A, Rosen R, Nard-Carmel N, et al. JAMA Otolaryngology– Head & Neck Surgery. 2019;145(6):542-548. doi:10.1001/jamaoto.2019.0784.
2. Frequency and Therapeutic Implications of “Skip Metastases” in the Neck From Squamous Carcinoma of the Oral Tongue. Byers RM, Weber RS, Andrews T, et al. Head & Neck. 1997;19(1):14-9. doi:10.1002/(sici)1097-0347(199701)19:13.0.co;2-y.
3. Incidence and Impact of Skip Metastasis in the Neck in Early Oral Cancer: Reality or a Myth?. Gurmeet Singh A, Sathe P, Roy S, et al. Oral Oncology. 2022;135:106201. doi:10.1016/j.oraloncology.2022.106201.
The basis and need for elective nodal treatment in head and neck cancer:
Have been based largely on surgical series evaluating pathologic nodal involvement found on elective neck dissection in patients with clinically negative necks
In a consecutive series of 1,081 head and neck cancer patients undergoing radical neck dissection:
The incidence of pathologic node involvement:
Was 33% among those undergoing elective neck surgery
The pathologic findings identified the nodal stations at risk by tumor site:
To establish the rationale for selective neck dissection (SND) as the elective surgical procedure
Several reports have summarized the risk for metastases and nodal stations at risk
Some general observations from such data can be made:
Regarding larynx cancers:
Candela reported the Memorial Sloan Kettering Cancer Center (MSKCC) experience in determining the patterns of cervical nodal metastases in 247 larynx cancer patients undergoing radical neck dissections:
The majority of patients (n = 189) were supraglottic larynx and 58 were glottic
Pathologic nodal involvement:
Was found in 37% undergoing elective neck dissection
It is noted that cervical nodes spread in a similar fashion whether the patients are clinically node negative or positive:
With predominant involvement of:
Level II and III jugular nodes
In clinically node-negative patients:
The incidence of involvement of level I and V:
Is less than 5% with less than 10% involvement of level IV
In node-positive patients:
The incidence of level IV node increases from 15% to 31% with greater involvement of levels II and III
In clinically node-positive patients:
Very rarely did patients present with isolated level I nodal metastases without involvement of the jugular nodes
Shah and Candela reported that among oropharynx or hypopharynx cancers:
Treated with elective radical neck dissection:
Occult metastases are found in 26%
Level I and V were involved in only 1.4%:
Always in association with nodal disease at level II to IV
No skip metastases were reported
Among oropharynx patients:
Levels II to IV were predominantly involved
Among hypopharynx lesions:
The primary levels involved were levels II and III
In patients clinically node positive undergoing therapeutic neck dissection:
The incidence of level I and V involvement increased to about 10% to 15%:
However, levels II to IV were predominantly involved
Level V involvement:
Only occurred in association with nodal involvement at levels II to IV
Whereas the incidence isolated level I involvement without levels II to IV involvement (“skip metastasis”):
Occurred in 0.4%:
Thus, based on these studies, elective treatment of the neck in oropharynx or hypopharynx can be directed at levels II to IV
Among oral cavity patients:
The incidence of nodal disease was 34% on elective evaluation
The majority of metastatic nodes involved:
Levels I to III:
With only 1.5% incidence of skip metastasis to level IV
Level V involvement:
Is found in only 0.5% with occult disease simultaneously involving other levels
Among those undergoing therapeutic neck dissections:
The incidence of level IV involvement increased to 20%
Level V was 4% always restricted to lower gum or floor of mouth primary sites
The need for elective treatment not only relates to the estimated probability of nodal involvement and usually is implemented when the risk is 20% or greater but also relates to the morbidity of such treatment as well as the adequacy of coverage
Guiding the decision to perform END in cN0 oral cavity SCC
The NCCN Guidelines stratify the decision as follows [1]:
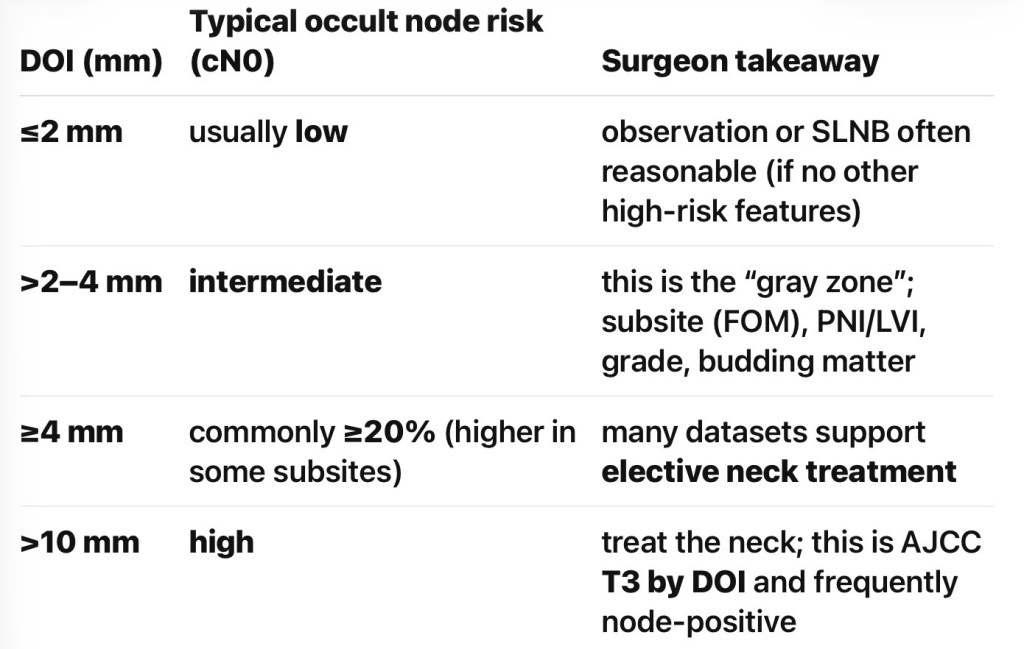
DOI 3 mm:
END should be strongly considered if RT is not already planned (supported by level 1 evidence from the D’Cruz / Tata Memorial trial)
The landmark D’Cruz et al. (2015) randomized trial of 500 patients with cT1 to T2 cN0 oral cavity SCC:
Demonstrated that upfront END significantly improved 3-year overall survival (80.0% vs. 67.5%) and disease-specific survival (69.5% vs. 45.9%) compared to therapeutic neck dissection [2]
Post hoc analysis showed no benefit for tumors with DOI ≤ 3 mm, while 28% of cN0 necks with DOI >3 mm harbored occult metastases [3]
A 2025 meta-analysis of 17 studies (2,263 patients):
Confirmed END reduces regional recurrence (RR 0.47) and improves OS (RR 0.75) and DSS (RR 1.32) [4]
A validation study of 300 patients:
Confirmed that DOI ≥ 4 mm is the optimal ROC-derived threshold (95.1% sensitivity, 52.9% specificity) for predicting occult nodal metastasis:
With regional recurrence-free survival significantly higher in the END group for DOI ≥ 4 mm (p = 0.002) [5]
A recent systematic review found:
Diagnostic thresholds converging around 4 mm for mixed oral cavity sites and 3 mm for high-risk subsites (floor of the mouth) [6]
The ASCO Clinical Practice Guideline (2019) recommends [2]:
cT2 to cT4, cN0:
Ipsilateral END should be performed (strong recommendation, high-quality evidence)
cT1, cN0:
Ipsilateral END should be performed:
Alternatively, close surveillance with specialized ultrasound may be offered for selected highly reliable patients
Tumor Size Considerations:
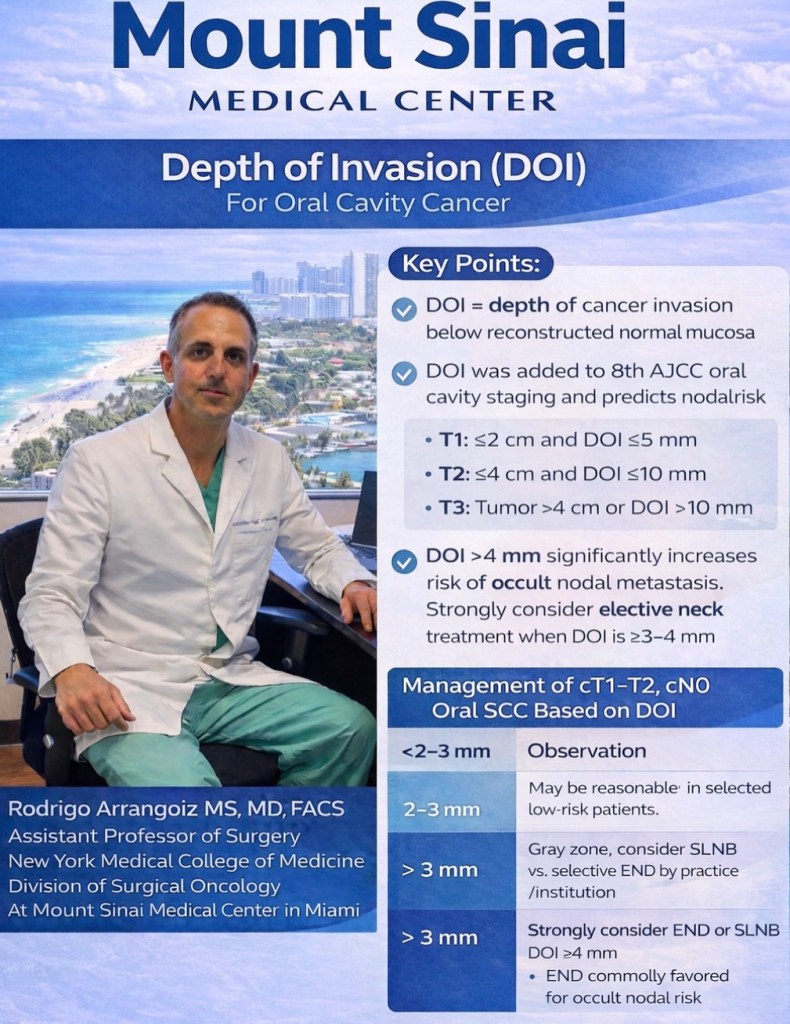
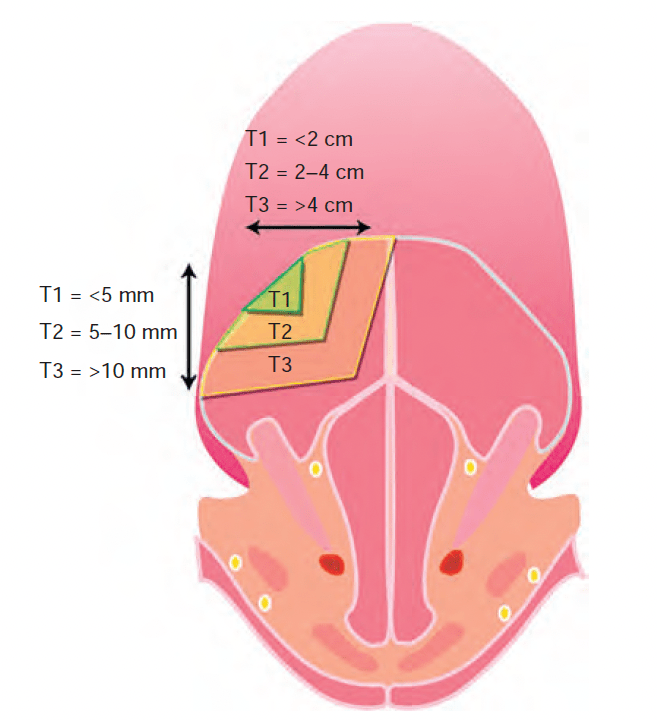
Under AJCC 8th edition staging, both surface size and DOI determine T classification [1]:
T1:
≤ 2 cm with DOI ≤ 5 mm
T2:
≤ 2 cm with DOI > 5 mm
> 2 cm and ≤ 4 cm with DOI ≤ 10 mm
T3 to T4:
T3:
> 4 cm
DOI > 10 mm
Locally advanced tumors carry ~40% to 50% risk of occult nodal metastases, making END essentially mandatory [2]
DOI cutoffs are more predictive of overall survival than T category based on tumor surface size alone [3]:
For T1 tumors, those with DOI ≤ 2 mm rarely demonstrate occult neck disease:
While DOI ≥ 2 mm confers at least a 20% risk of pN+ disease [3]
Subsite-Specific Considerations:
Oral Tongue:
The most extensively studied subsite
DOI ≥ 3 mm to 4 mm:
Is the standard threshold for END [3]
Higher propensity for skip metastases:
To level III (17.5% of specimens) compared to other subsites
Anterior tongue tumors at / near midline:
Warrant consideration for bilateral neck dissection [1]
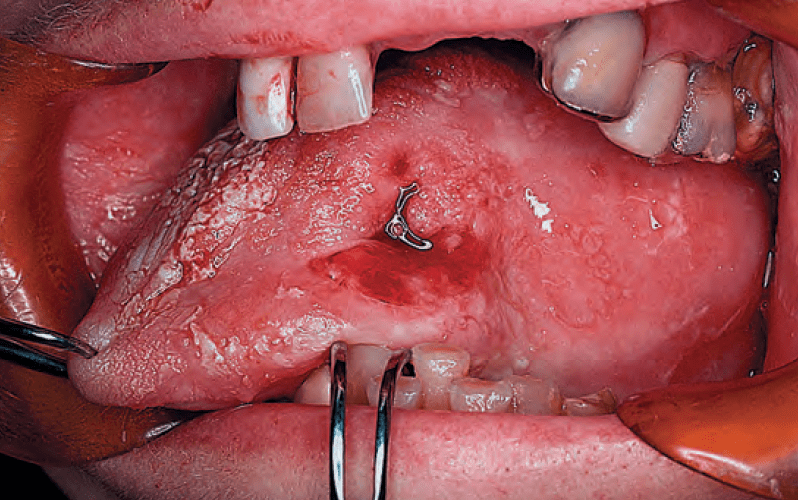
Floor of Mouth (FOM):
FOM tumors cross the critical 20% threshold for nodal metastasis at a lower DOI (≥ 2 mm) compared to oral tongue (≥ 4 mm):
Based on a study of 343 patients:
41.7% nodal metastasis rate for FOM tumors 2.1 mm to 4 mm thick vs. 11.2% for tongue tumors of similar thickness [7]
FOM primaries have a predisposition for contralateral metastases even at earlier T stages:
With a 50% higher risk of contralateral metastasis and 2.6-times higher risk when FOM invasion / extension is present [3][2]
However, a more recent study of 825 patients:
Found no significant difference in the incidence of or correlation between DOI and nodal metastases when FOM was compared to other subsites [8]
SLN biopsy accuracy:
Is lower for FOM than for tongue primaries [1]
Buccal Mucosa:
Behaves more aggressively:
With occult metastasis rates as high as 32% and up to 43% presenting with clinical / radiographic nodal disease [3]
END is recommended for all buccal cases:
Irrespective of DOI given higher rates of nodal metastases even in early T-category disease [3]
A multicenter study of 101 patients confirmed END improved survival in pT2, cN0 buccal SCC:
123 months vs. 26 months, p = 0.009) [9]
END demonstrated improved:
Locoregional recurrence-free rates (61% vs. 38%, p = 0.042)
5-year DFS (75% vs. 63%, p = 0.019) [10]
Other Subsites (Alveolar Ridge, Retromolar Trigone, Hard Palate):
Generally follow the same DOI-based principles
Hard palate and upper gingiva:
May not lend themselves well to SLN biopsy [1]
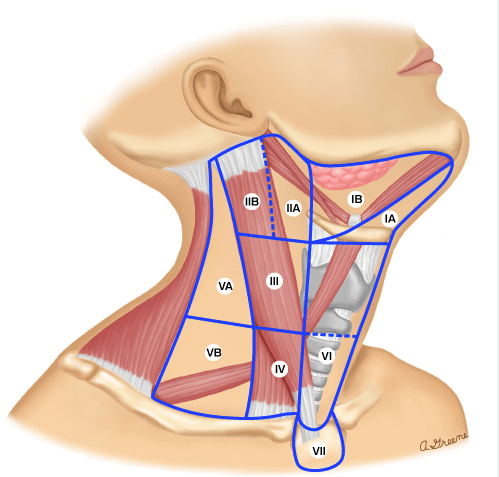
Levels of Dissection: I to III vs. I to IV:
This is the NCCN treatment algorithm for cT1 to cT2, N0 oral cavity SCC:
For the cN0 neck:
The standard END is a supraomohyoid neck dissection (SOHND) encompassing levels I to III
Both the NCCN and ASCO guidelines recommend at minimum:
Levels Ia, Ib, II, and III, with an adequate yield of ≥ 18 lymph nodes [1][2]
Two randomized trials comparing SOHND (levels I to III) versus modified radical neck dissection (levels I to V):
Showed the adequacy of SOHND, with more extensive dissection increasing morbidity (particularly shoulder dysfunction) without survival or recurrence benefit:
Only 3.7% of occult metastases were detected in levels IV and V [2]
The American Head and Neck Society review consolidates the recommendation:
Level I to III dissection in the cN0 setting, with consideration of level IV inclusion in higher-risk tumors [3]
Skip Metastasis to Level IV:
The Key Data:
The Warshavsky et al. (2019) systematic review and meta-analysis in JAMA Otolaryngology (13 studies, 1,359 patients) provides the most comprehensive data [11]:
Overall rate of level IV involvement in cN0 patients:
2.53% (95% CI, 1.64%–3.55%)
True skip metastasis rate:
Level IV positive without levels I to III involvement): 0.50% (95% CI, 0.09%–1.11%)
Subgroup by T stage:
Level IV involvement was 0% for stages I to II and 0% for stages III to IV in the skip metastasis analysis
Oral tongue subsite:
Level IV involvement was notably higher at 3.60% (95% CI, 2.09%–5.42%):
The only subsite with significant findings
A large audit of 1,004 cases:
Confirmed skip metastases to level IV were 2.2% for tongue and 1.2% for gingivobuccal primaries [12]
A 2024 study of 544 early-stage oral tongue SCC patients:
Found only 1.3% had nodal involvement of level IV or V, concluding that END of levels I to III is sufficient [13]
A recent 2026 study directly comparing outcomes of END levels I to III vs. I to IV in 120 oral tongue SCC patients found [14]:
Only 1 of 33 patients (3%) undergoing level I to IV dissection had level IV metastasis
No significant difference in regional recurrence (21.8% vs. 18.2%, p = 0.66), level IV recurrence (3.5% vs. 3%, p = 0.91), or 5-year OS (69.3% vs. 61.1%, p = 0.7)
However, one study of 111 T1 / T2 N0 oral tongue SCC patients:
Found a 6.3% occult metastasis rate to level IV:
Arguing that extended SOHND covers this risk [15]
Additionally, when levels I to III are already pN+:
The risk of level IV to V metastases rises to 9.8%:
Particularly with > 1 positive node or pN classification > pN2b [16]
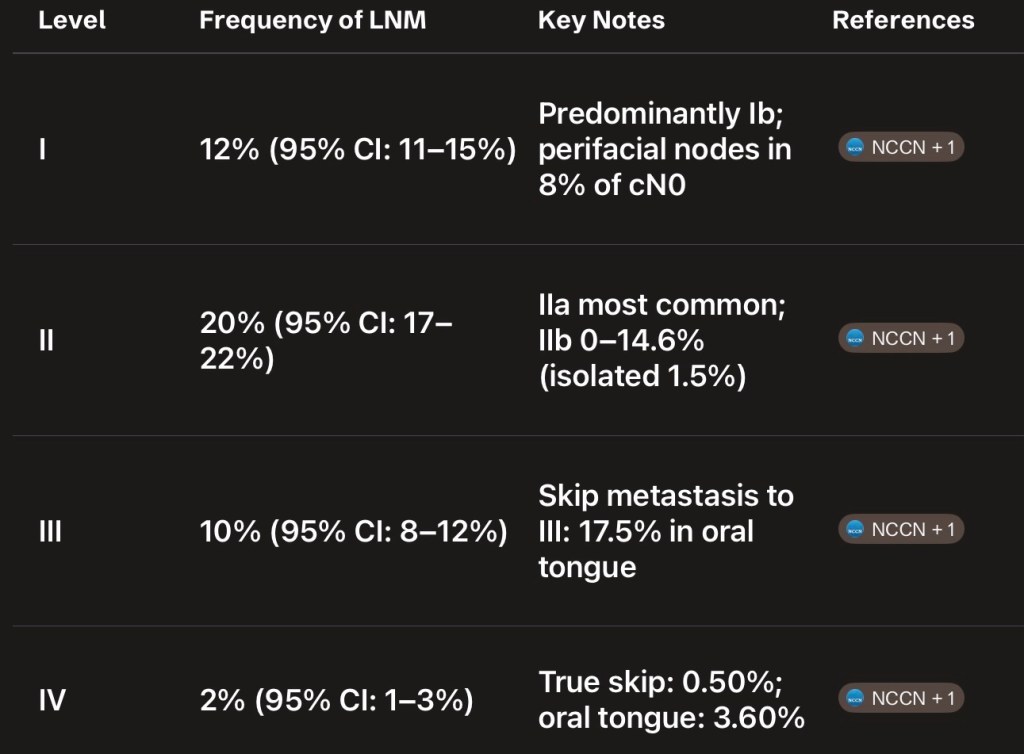
Summary of Frequency of Nodal Metastasis by Level:
A meta-analysis of 17 studies found the following frequencies of lymph node metastasis across all OSCC [17] – Figure
Clinical Synthesis:
For the cN0 neck, levels I to III dissection is the standard of care across all oral cavity subsites
The evidence does not support routine inclusion of level IV given the extremely low rate of true skip metastasis (0.50% overall)
For oral tongue SCC specifically:
The slightly higher rate of level IV involvement (3.60%) has prompted some authors to advocate for level IV inclusion:
But direct comparative studies show no survival or recurrence benefit from extending to level IV [14]
Level IV should be considered in higher-risk scenarios:
pN+ disease in levels I to III (especially multistation), greater DOI, or adverse pathologic features
For the cN+ neck:
Therapeutic dissection should include levels I to IV:
With level V considered in multistation disease [2]
References:
1. Head and Neck Cancers. National Comprehensive Cancer Network. Updated 2025-12-08.
2. Management of the Neck in Squamous Cell Carcinoma of the Oral Cavity and Oropharynx: ASCO Clinical Practice Guideline. Koyfman SA, Ismaila N, Crook D, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2019;37(20):1753-1774. doi:10.1200/JCO.18.01921.
3. Oral Cavity Cancer Surgical and Nodal Management: A Review From the American Head and Neck Society. Eskander A, Dziegielewski PT, Patel MR, et al. JAMA Otolaryngology– Head & Neck Surgery. 2024;150(2):172-178. doi:10.1001/jamaoto.2023.4049.
4. Impact of Elective Cervical Dissection on the Prognosis of Patients With Oral Squamous Cell Carcinoma cT1/T2N0: A Systematic Review and Meta-Analysis. Binda NC, Lavareze L, de Souza Vieira G, et al. Critical Reviews in Oncology/Hematology. 2025;:104982. doi:10.1016/j.critrevonc.2025.104982.
5. Depth of Invasion in Early Stage Oral Cavity Squamous Cell Carcinoma: The Optimal Cut-Off Value for Elective Neck Dissection. van Lanschot CGF, Klazen YP, de Ridder MAJ, et al. Oral Oncology. 2020;111:104940. doi:10.1016/j.oraloncology.2020.104940.
6. Elective Neck Dissection Strategies Guided by AJCC-8 Depth-of-Invasion (DOI) in cT1-T2N0 Oral Cavity Cancer-a Systematic Review. Abdul NS, Shivakumar S, Alreshaid L, et al. Cancers. 2026;18(4):697. doi:10.3390/cancers18040697.
7. Tumour Thickness as a Predictor of Nodal Metastases in Oral Cancer: Comparison Between Tongue and Floor of Mouth Subsites. Balasubramanian D, Ebrahimi A, Gupta R, et al. Oral Oncology. 2014;50(12):1165-8. doi:10.1016/j.oraloncology.2014.09.012.
8. The Relative Propensity for Regional Metastasis in Floor of Mouth Squamous Cell Carcinoma Versus Other Oral Cavity Subsites. Wicks C, Zubair F, Ogunbowale A, McMahon J. The British Journal of Oral & Maxillofacial Surgery. 2022;60(9):1276-1278. doi:10.1016/j.bjoms.2022.07.012.
9. Management of the Neck in T1 and T2 Buccal Squamous Cell Carcinoma. Nicholson OA, Van Lanschot CGF, van den Besselaar BN, et al. International Journal of Oral and Maxillofacial Surgery. 2024;53(4):259-267. doi:10.1016/j.ijom.2023.07.004.
10. What Is the Role of Elective Neck Dissection in the Management of Patients With Buccal Squamous Cell Carcinoma and Clinically Negative Neck?. Dillon JK, Villing AS, Jones RS, et al. Journal of Oral and Maxillofacial Surgery : Official Journal of the American Association of Oral and Maxillofacial Surgeons. 2019;77(3):641-647. doi:10.1016/j.joms.2018.10.021.
11. Assessment of the Rate of Skip Metastasis to Neck Level IV in Patients With Clinically Node-Negative Neck Oral Cavity Squamous Cell Carcinoma: A Systematic Review and Meta-analysis. Warshavsky A, Rosen R, Nard-Carmel N, et al. JAMA Otolaryngology– Head & Neck Surgery. 2019;145(6):542-548. doi:10.1001/jamaoto.2019.0784.
12. Nodal Yield and Topography of Nodal Metastases From Oral Cavity Squamous Cell Carcinoma – An Audit of 1004 Cases Undergoing Primary Surgical Resection. Roy P, Mallick I, Arun I, et al. Oral Oncology. 2021;113:105115. doi:10.1016/j.oraloncology.2020.105115.
13. Risk Factors and Impact of Occult and Skip Metastasis in Early-Stage Oral Tongue Squamous Cell Carcinoma. Yang X, Xiang W, Sun Y, et al. Clinical Oral Investigations. 2024;28(9):510. doi:10.1007/s00784-024-05897-8.
14. The Prognostic Significance of Elective Level 4 Neck Dissection in Oral Tongue Cancer. Yosefof E, Edri N, Ritter A, et al. Journal of Surgical Oncology. 2026;133(4):459-464. doi:10.1002/jso.70191.
15. How Adequate Is Supraomohyoid Neck Dissection for Node-Negative Oral Tongue Squamous Cell Carcinoma?. Sharma R, Singh N, Joshi KD, Sr A, Patrikar S. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2025;:S1010-5182(25)00102-7. doi:10.1016/j.jcms.2025.03.006.
16. In Vivo Probability of Metastases in Levels IV-V in Oral Squamous Cell Carcinoma With a cN0/pN+ Situation in Levels I-Iii. Haas L, Mischkowski RA, Knape U, Król KM, Sakkas A. In Vivo (Athens, Greece). 2025 Nov-Dec;39(6):3437-3444. doi:10.21873/invivo.14141.
17. Frequency of Lymph Node Metastases at Different Neck Levels in Patients With Oral Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. Yu YF, Cao LM, Li ZZ, et al. International Journal of Surgery (London, England). 2025;111(1):1285-1300. doi:10.1097/JS9.0000000000001953.
A meta-analysis of 17 studies found the following frequencies of lymph node metastasis across all OSCC [17]#Arrangoiz #Doctor #Surgeon #SurgicalOncologist #HeadandNeckSurgeon #CancerSurgeon #Miami #MSMC #MountSinaiMedicalCenter #Mexico
Byers RM, Weber RS, Andrews T, McGill D, Kare R, Wolf P. Frequency and therapeutic implications of “skip metastases” in the neck from squamous carcinoma of the oral tongue. Head Neck. 1997 Jan;19(1):14-9. doi: 10.1002/(sici)1097-0347(199701)19:1<14::aid-hed3>3.0.co;2-y. PMID: 9030939.
Background:
Supraomohyoid neck dissection (Levels I, II, III):
Is an adequate operation for the elective treatment of the neck for patients with oral cavity cancer
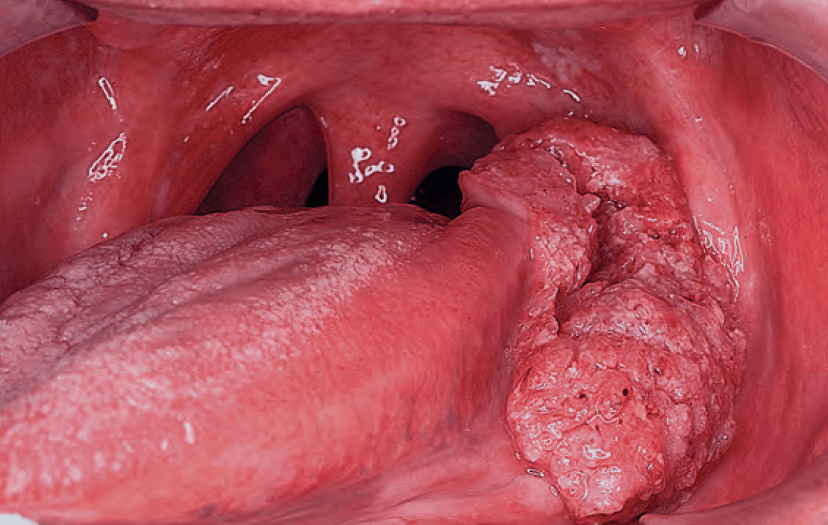
Squamous cell carcinoma of the oral tongue:
Metastasize to clinically negative nodes:
In 20% to 30% of patients:
These nodes usually are located in:
Levels I to III
Methods:
The medical records of 277 previously untreated patients with squamous cell carcinoma of the oral tongue were reviewed between the years 1970 and 1990
All patients had a glossectomy and neck dissection as part of their initial treatment
Patients were evaluated as to the findings in their neck
The following group of patients were included:
Patients who had level III nodes positive, without disease in levels I and II
Patients with disease in level IV
Patients with disease in level IIB or IIIB
Patients who were electively dissected and whose neck did not demonstrate any pathologically involved nodes:
But level IV was not included in the dissection and the patient subsequently developed pathologically positive nodes in level IV
Results:
Of all patients:
15.8% had either level IV metastasis as the only manifestation of disease in the neck or the level III node was the only node present without disease in level I to II
Conclusion:
The usual supraomohyoid neck dissection is inadequate for a complete pathologic evaluation of all the nodes at risk for patients with squamous carcinoma of the oral tongue
This may create a dilemma in determining whether postoperative radiotherapy is necessary
Consequently, all patients with squamous cell carcinoma of the oral tongue should have levels I to IV nodes (Extended Supraomohyoid Neck Dissection) removed:
If an elective neck dissection is part of their initial therapy
Here is an expanded summary of Baratz et al., “Neoadjuvant Immunotherapy and Chemoimmunotherapy Regimens in Head and Neck Cancer: A Systematic Review and Meta-Analysis,” published online in JAMA Otolaryngology–Head & Neck Surgery on March 12, 2026
Why this paper matters:
Neoadjuvant immunotherapy in resectable HNSCC:
Has been attractive because:
It may treat micrometastatic disease early
Exploit the intact tumor-immune microenvironment before surgery
It may potentially improve pathologic response without delaying definitive treatment
What has been unclear is whether immunotherapy alone or chemoimmunotherapy is more effective
This meta-analysis addresses that question by pooling the available prospective data in resectable, treatment-naive HNSCC
Objective:
The investigators aimed to:
Summarize the efficacy of neoadjuvant chemoimmunotherapy in HNSCC
Compare outcomes of chemoimmunotherapy vs immunotherapy alone:
Before definitive surgery in locoregionally advanced resectable HNSCC
Methods:
This was a librarian-led systematic review and meta-analysis performed according to PRISMA methodology
The authors searched MEDLINE, EMBASE, Cochrane Central, Cochrane Database of Systematic Reviews, and Scopus from database inception through October 2024
They included prospective interventional trials in resectable, treatment-naive HNSCC that had completed accrual and reported pathologic response and / or RECIST response data
Two investigators independently performed study screening and extraction
The main outcomes were:
Major pathologic response (MPR)
Complete pathologic response (CPR)
Complete radiographic response (CR):
By RECIST 1.1
Secondary outcomes included:
1-year overall survival
Toxicity
The pooled analysis used a binary random-effects model, with heterogeneity reported as I²
Study population:
The meta-analysis included 23 studies with a total of 751 patients. Of these:
357 patients (47%) received chemoimmunotherapy
102 patients (14%) received dual-agent immunotherapy
292 patients (39%) received single-agent immunotherapy
The pooled cohort was predominantly male (77%) with an age range of 27 to 87 years
Main findings:
Pathologic response:
Strongly favored chemoimmunotherapy
The most important finding was:
The marked gradient in pathologic response across regimens:
Pooled MPR + CPR rates were:
66% for chemoimmunotherapy 95% CI 58%-73%
18% for dual-agent immunotherapy 95% CI 6%–29%
6% for single-agent immunotherapy 95% CI 3%–9%
This is the key take-home point:
Adding chemotherapy to immunotherapy:
Was associated with substantially higher pathologic response rates than immunotherapy alone
Clinically, this matters because in head and neck cancer:
Pathologic response has increasingly been explored as an early signal of antitumor activity and a possible surrogate for longer-term benefit:
Although it is not yet a fully validated surrogate for survival in this setting
That distinction is important when interpreting these results
The paper shows better tumor kill in the surgical specimen:
But it does not yet prove that patients live longer because of the neoadjuvant regimen:
That is why the authors call for phase 3 trials
Short-term survival looked promising across groups, but differences were not definitive:
Across the included studies, 1-year overall survival ranged:
88% to 96% with single-agent immunotherapy
88% to 96% with dual-agent immunotherapy
88% to 100% with chemoimmunotherapy
These ranges suggest that all three strategies can be delivered with good short-term outcomes in selected patients:
However, because these were mainly early-phase, non-comparative studies with heterogeneous populations and follow-up:
The survival data should be viewed as hypothesis-generating, not practice-defining
Toxicity was higher than dual immunotherapy, but not prohibitive:
Among studies reporting adverse events, grade 3 to 5 adverse events occurred in:
29% of patients receiving single-agent immunotherapy
3% with dual-agent immunotherapy
17% with chemoimmunotherapy
These numbers need cautious interpretation because toxicity reporting was not uniform across studies, and the denominators were limited to reporting studies rather than all pooled patients:
Still, the overall message is that chemoimmunotherapy increased efficacy while maintaining an acceptable:
Though not trivial, toxicity burden in selected surgical candidates.
Authors’ conclusion:
The authors concluded that neoadjuvant chemoimmunotherapy:
Was associated with higher pathologic and radiographic response rates than immunotherapy alone in locoregionally advanced resectable HNSCC, and that these findings support the need for head-to-head phase 3 trials
How to interpret this as a head and neck oncologic surgeon:
Strengths:
This study has several strengths:
It focuses specifically on resectable, treatment-naive HNSCC:
Which is the clinically relevant population for neoadjuvant decision-making
It includes only prospective interventional studies
It separates single-agent, dual-agent, and chemoimmunotherapy approaches rather than lumping all neoadjuvant immunotherapy together
It uses outcomes surgeons and multidisciplinary teams care about:
Pathologic response, radiographic response, survival, and toxicity
Important limitations:
The paper is very useful, but it does not settle the question of standard of care
The biggest limitations are:
Most included studies were phase 1 / 2, small, and often single-arm
There was likely substantial clinical heterogeneity:
Primary site, stage, PD-L1 status, regimen, number of cycles, and adjuvant treatment strategies
The outcome driving the signal is primarily pathologic response:
Not mature event-free survival or overall survival
Cross-trial comparisons may exaggerate differences:
Because these were not randomized head-to-head comparisons
Toxicity and imaging response reporting were not fully standardized
So the paper supports promise:
Not final proof
Practical clinical implications:
For a practicing surgeon:
This meta-analysis suggests that chemoimmunotherapy is currently the most active neoadjuvant immune-based strategy in resectable HNSCC:
At least if the endpoint is pathologic response
If a center is considering neoadjuvant treatment within a trial or highly selected multidisciplinary framework:
The data support prioritizing chemoimmunotherapy over immunotherapy alone when the goal is maximizing preoperative tumor regression
At the same time, these data do not mean every resectable oral cavity, larynx, or oropharynx patient:
Should routinely receive neoadjuvant chemoimmunotherapy outside a protocol
The field is moving quickly, and the editorial accompanying this paper emphasizes that these results arrive in the context of KEYNOTE-689:
The first phase 3 randomized study to establish perioperative immunotherapy as a standard-of-care option in locally advanced resectable HNSCC:
While also warning that enthusiasm should be balanced with caution as these strategies enter broader practice
Bottom line:
This meta-analysis is one of the clearest pooled signals so far that in resectable locoregionally advanced HNSCC, neoadjuvant chemoimmunotherapy produces substantially higher pathologic response rates than immunotherapy alone
The benefit signal is strong for tumor response, short-term survival appears encouraging, and toxicity seems manageable in selected patients:
But the evidence base is still dominated by early-phase studies, so phase 3 randomized data remain essential before universal adoption
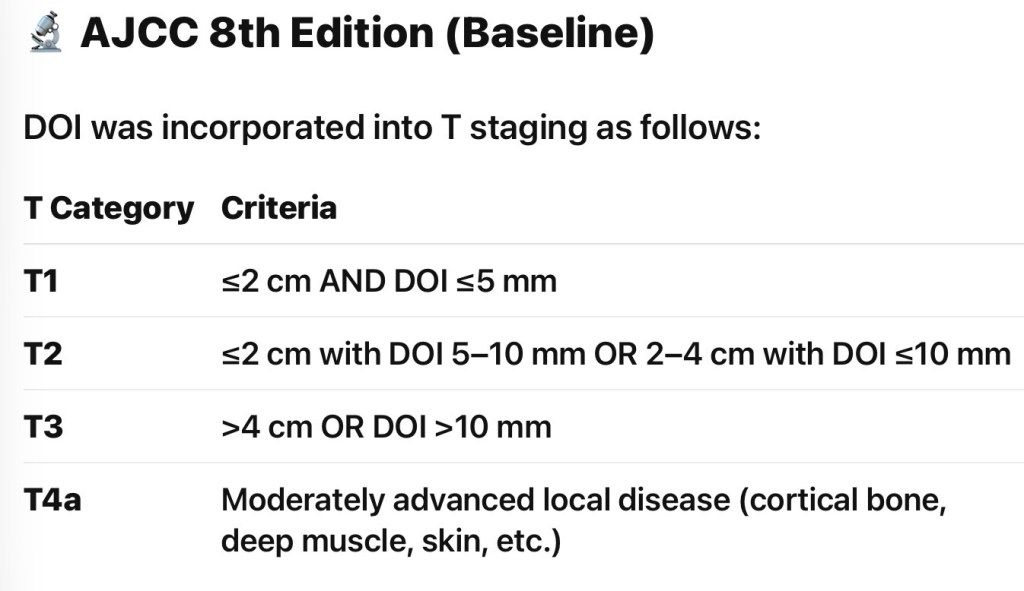
As published by the AJCC and UICC is widely accepted
In its most recent revision (eighth edition of the AJCC Staging Manual):
Depth of invasion (DOI):
Is added to the surface dimensions and local extent of the tumor:
As the required parameters for primary tumor staging in the oral cavity
Depth of invasion and surface dimensions are the parameters required for T staging of oral cancer
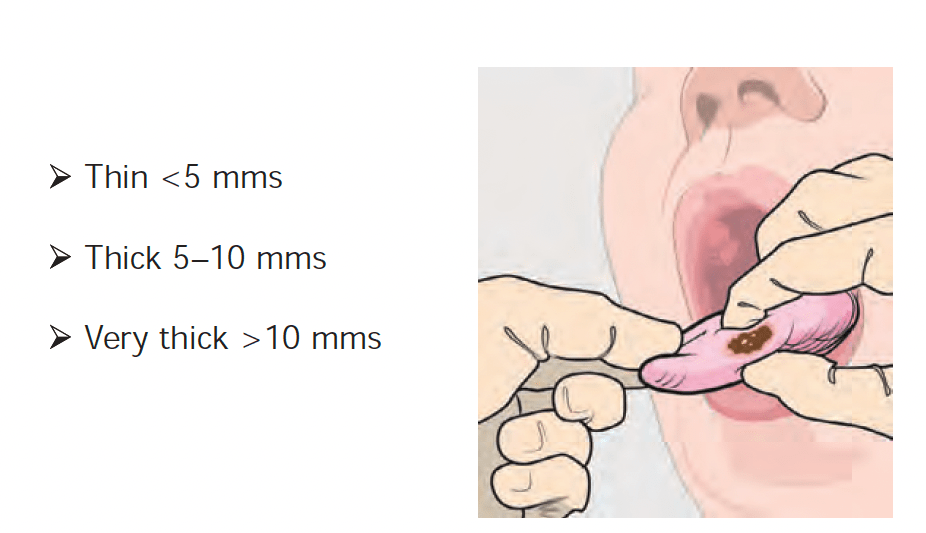
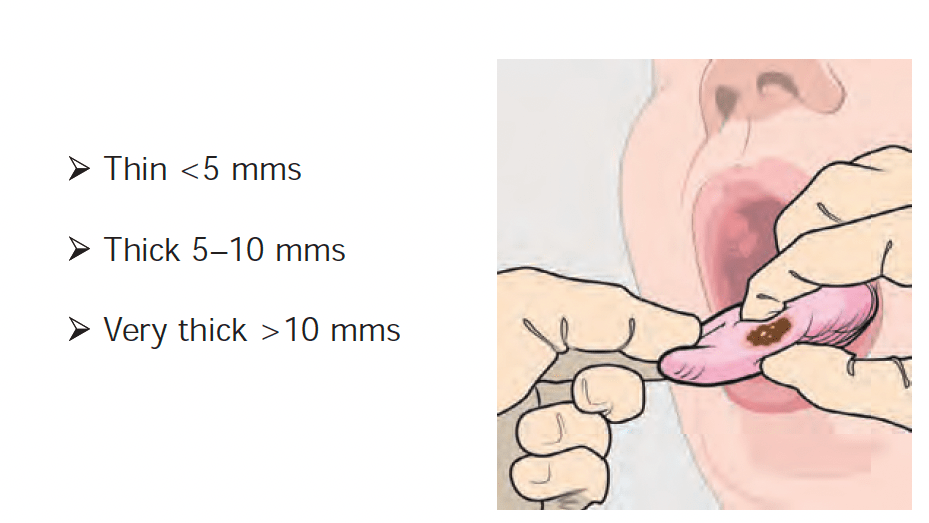
Accurate assessment of DOI by clinical examination is not possible:
However, the staging system stratifies DOI by 5 mm increments, and thus clinical estimates of DOI can be categorized into:
Thin (less than 5 mm)
Thick (5 to 10 mm)
Very thick (greater than 10 mm)
By palpation to assign clinical T stage
Primary tumors of the oral cavity are categorized as thin, thick, and very thick by palpation
The stage distribution of patients with squamous cell carcinoma of the oral cavity at the Memorial Sloan Kettering Cancer Center in New York is shown in the graph:
Stage distribution for squamous cell carcinoma of the oralcavity (MSKCC data 1985 to 2015)
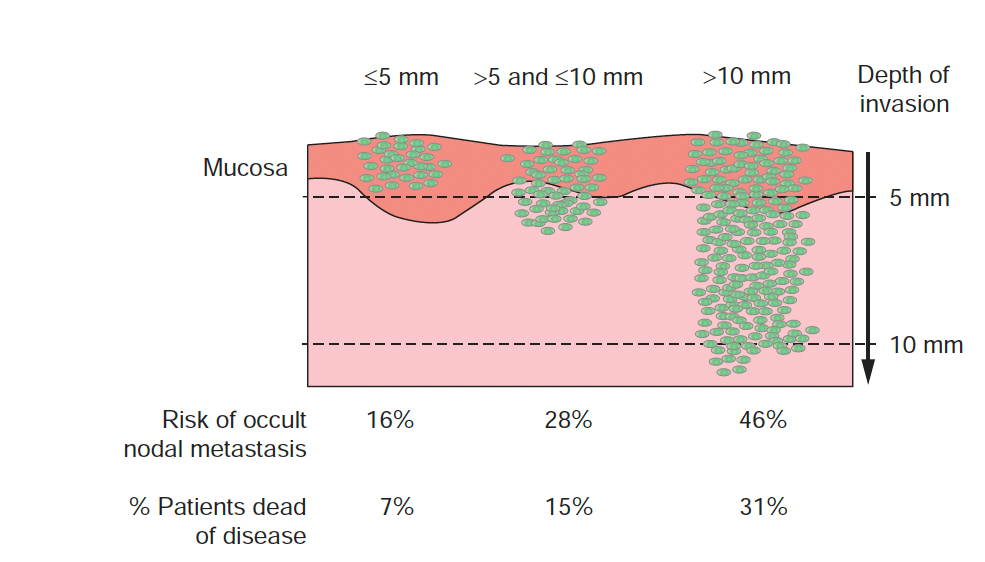
The most important histologic feature of the primary tumor:
That affects selection of treatment and eventual prognosis:
Is its depth of invasion (DOI)
Thin and superficially invasive lesions:
Have a lower risk of regional lymph node metastasis
Are highly curable
Offer an excellent prognosis
Thicker lesions that deeply infiltrate the underlying soft tissues:
Have a significantly increased incidence of regional lymph node metastasis and an adverse impact on prognosis
The risk of lymph node metastasis and survival rates in relation to the DOI of the primary lesion for T1 and T2 squamous carcinomas of the oral tongue and floor of mouth are shown in Figure:
Although it would be ideal to know the exact DOI of the lesion before surgical intervention, having that information before surgical excision and histopathologic examination of the primary tumor is not possible
In general, however, estimate of DOI by assessing thickness of the lesion as appreciated by palpation:
Is a reasonably good indicator of deeply invasive lesions versus superficial lesions:
To estimate the extent of soft tissue and / or bone resection for the primary lesion and to decide on the need for elective dissection of the regional lymph nodes at risk in a clinically negative neck
Primary tumors of the oral cavity are categorized as thin,thick, and very thick by palpation
Several retrospective studies have identified DOI of the primary tumor:
As an important determinant of prognosis:
Thus DOI is now included in T staging of primary tumors of the oral cavity
The incidence of occult nodal metastasis in the clinicallynegative neck for patients and disease-specific survival for patients withT1 and T2 oral carcinoma in relation to depth of invasion (DOI). (Memorial Sloan Kettering Cancer Center data, 1985 to 2015).
Depth of invasion (DOI) is the vertical depth of tumor invasion:
Measured from the basement membrane of the adjacent normal mucosa to the deepest point of invasion:
It is not the same as “tumor thickness”
DOI is now a core determinant of T category in AJCC 8th and 9th oral cavity SCC:
AJCC 8 DOI cut points (oral cavity):
T1:
≤ 2 cm and DOI ≤ 5 mm
T2:
≤ 2 cm with DOI > 5 to 10 mm OR > 2 to 4 cm with DOI ≤ 10 mm
T3:
DOI >10 mm (or tumor > 4 cm)
Clinical implication:
A small “T1 by size” lesion can become T2 / T3 purely based on DOI:
Changing risk counseling and neck strategy
Risk of occult nodal metastasis vs DOI (tongue and floor of mouth):
Big picture (consistent across studies):
DOI is one of the strongest predictors of occult cervical lymph node metastasis (CLNM) in cN0 oral cavity SCC
A commonly used operative decision threshold is:
DOI ~ 3 to 4 mm:
But subsite matters, and FOM often carries higher nodal risk at the same DOI
Practical DOI “risk bands” used in tumor boards
Evidence supporting ≥ 4 mm as an elective neck dissection (END) trigger (early OCSCC):
Multiple analyses suggest DOI ≥ 4 mm is an effective cutoff where END improves regional control / survival compared with observation in early-stage OCSCC
Recent work continues to evaluate / validate a 4 mm threshold, acknowledging imperfect sensitivity / specificity
Meta-analytic evidence shows higher lymph node metastasis (LNM) risk when DOI > 4 mm (RR ~2.18 in one large study, alongside other adverse pathologic factors)
Floor of mouth nuance:
At the same DOI:
FOM cancers may metastasize more frequently than tongue cancers in some datasets:
Implying that a single universal DOI cutoff across all subsites can be overly simplistic
Prognosis vs DOI (local control, survival, and upstaging):
DOI correlates with:
Higher probability of nodal metastasis:
Including occult disease
Worse disease-specific outcomes:
It is sufficiently prognostic that it was incorporated into AJCC 8 edition T staging
DOI > 10 mm is particularly important because it upstages to pT3 (even if tumor is small in surface dimension):
Reflecting its association with advanced / aggressive behavior
Key point for counseling:
DOI is not just a “neck decision tool”:
It is a global biologic aggressiveness marker and a staging variable
Elective neck management in cN0 tongue / FOM SCC:
Guideline-consistent approach:
NCCN guidance (summarized in literature):
Consider elective neck dissection (END) in early oral cavity SCC when DOI exceeds ~3 mm (often framed as “consider END”)
Many institutions operationalize:
Tongue:
END commonly at ≥ 4 mm
FOM:
Lower threshold and / or stronger lean toward END due to higher nodal propensity in several series
END vs sentinel lymph node biopsy (SLNB) vs observation:
Elective Neck Dissection (END):
Typical for cN0 early tongue / FOM:
Selective neck dissection levels I to III ± IV based on institutional practice, DOI, and risk factors:
Benefit is maximizing regional control and avoiding “salvage neck failure” biology
Sentinel Lymph Node Biopsy (SLNB):
Valid alternative to END for T1 to T2 cN0 oral cavity SCC in experienced centers:
Especially when trying to reduce morbidity
Practical pearl:
SLNB is most attractive when DOI is low / intermediate and imaging is negative:
But your workflow must support reliable mapping / pathology
Observation:
Reasonable primarily for very thin lesions (e.g., ≤ 2 mm) without other high-risk features and with reliable follow-up
Remember:
DOI cutoffs have imperfect test characteristics:
A “thin” tumor can still metastasize
A pragmatic surgeon algorithm (tongue + floor of mouth, cN0):
Pre-op:
High-quality exam + imaging
Estimate DOI if possible:
US / MRI can help in some settings
If DOI likely > 10 mm (or bulky lesion):
Treat the neck (END)
If DOI 4 to 10 mm:
Strong default to END (levels I to III) or SLNB if program is robust