Consensus Recommendations – Early Breast Cancer
- ER-Positive / HER2-Negative Disease:
- Genomic Testing:
- Strong support for multigene assays (Oncotype DX, MammaPrint, etc.) in:
- Node-negative disease
- 1 to 3 positive nodes:
- Especially postmenopausal:
- In premenopausal patients with 1 to 3 nodes → chemotherapy often still favored even with low genomic risk
- Especially postmenopausal:
- Genomic Testing:
- Chemotherapy:
- Postmenopausal:
- N1 (1 to 3 nodes), low genomic risk:
- Chemotherapy can be omitted
- N1 (1 to 3 nodes), low genomic risk:
- Premenopausal:
- N1 disease:
- Chemotherapy generally recommended:
- Ovarian suppression contribution acknowledged but not universally accepted as replacement
- Chemotherapy generally recommended:
- N1 disease:
- Postmenopausal:
- Ovarian Function Suppression (OFS):
- Recommended in:
- High-risk premenopausal patients
- Node-positive disease AI + OFS preferred over tamoxifen alone in higher-risk settings
- Recommended in:
- CDK4/6 Inhibitors:
- Abemaciclib recommended in:
- High-risk node-positive (monarchE-like criteria)
- Ribociclib:
- Data discussed but not yet fully standard globally
- Abemaciclib recommended in:
- HER2-Positive Early Breast Cancer:
- Neoadjuvant Therapy:
- Standard for:
- Tumors ≥ 2 cm
- Node-positive disease
- Preferred regimen:
- Taxane + dual anti-HER2 (trastuzumab + pertuzumab)
- Standard for:
- Residual Disease After Neoadjuvant Therapy:
- T-DM1 (KATHERINE data) remains standard
- Duration of Trastuzumab:
- 12 months remains consensus standard
- 6 months acceptable only in select lower-risk or toxicity cases
- De-escalation:
- Small node-negative HER2+ (< 2 cm):
- TH regimen acceptable (APT-like approach)
- Ongoing interest in response-adapted therapy
- Small node-negative HER2+ (< 2 cm):
- Neoadjuvant Therapy:
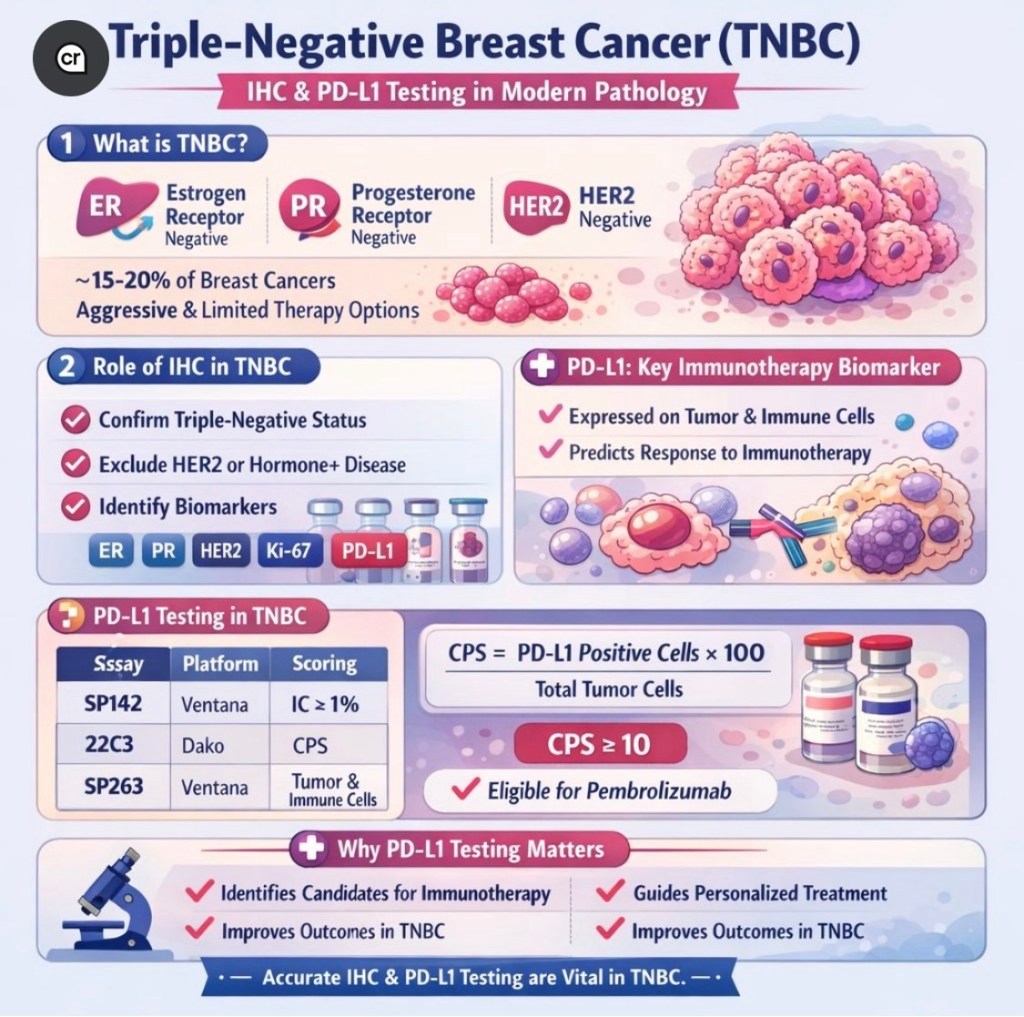
- Triple-Negative Breast Cancer (TNBC):
- Neoadjuvant Therapy:
- Standard:
- Anthracycline + taxane backbone
- Addition of pembrolizumab:
- Supported in stage II to III
- Standard:
- Residual Disease:
- Continue pembrolizumab:
- KEYNOTE-522 strategy
- Capecitabine considered if no prior immunotherapy
- Continue pembrolizumab:
- BRCA-Mutated:
- Adjuvant olaparib recommended:
- OlympiA criteria
- Adjuvant olaparib recommended:
- Neoadjuvant Therapy:
- Axillary Management:
- Clinically Node-Negative:
- Sentinel lymph node biopsy (SLNB) standard
- 1 to 2 Positive Sentinel Nodes (Upfront Surgery):
- Omission of ALND supported if:
- Undergoing breast-conserving therapy Whole-breast RT planned – ACOSOG Z0011 principles upheld
- Omission of ALND supported if:
- After Neoadjuvant Therapy:
- If cN+:
- ycN0:
- SLNB acceptable if ≥ 3 nodes retrieved + dual tracer
- Residual nodal disease → ALND still recommended in most settings
- ycN0:
- If cN+:
- Clinically Node-Negative:
- Radiation Therapy:
- Hypofractionation:
- Standard for most patients
- Ultra-hypofractionation (FAST-Forward-like) widely accepted
- Omission of RT:
- May be considered in:
- Age ≥ 70
- Small ER+ tumors
- Planned endocrine therapy
- May be considered in:
- Hypofractionation:
- Regional Nodal Irradiation:
- Recommended in:
- Node-positive disease
- High-risk biology
- Recommended in:
- De-escalation Themes:
- Avoid overtreatment in:
- Low-risk luminal A disease
- Elderly / frail patients
- Tailor treatment based on:
- Biology > anatomy alone
- Genomic profiling
- Patient preference
- Avoid overtreatment in:
- Liquid Biopsy & MRD:
- ctDNA promising but:
- Not yet standard for treatment decision:
- Still investigational for escalation / de-escalation
- Not yet standard for treatment decision:
- ctDNA promising but:
- Germline Mutation Carriers
- BRCA1/2:
- Consider bilateral mastectomy (case-dependent)
- Adjuvant olaparib in high-risk early disease
- PALB2 increasingly treated similarly to BRCA in high-risk scenarios
- BRCA1/2:
- Artificial Intelligence and Imaging:
- MRI not routine for all early-stage patients
- PET-CT not recommended for stage I routine staging
- AI emerging for:
- Risk stratification
- Imaging interpretation
- Treatment personalization
- Key Global Themes of St. Gallen 2025:
- Precision > escalation Biology-driven treatment
- Safe de-escalation when supported by data
- Increased use of CDK4/6 inhibitors and immunotherapy in early disease
- Continued minimization of axillary surgery