👉The EORTC Trial 10801 was a randomized multicenter trial that compared breast-conserving therapy with MRM for patients with invasive breast cancer less than 5 cm in diameter.
👉At 10 years, there was no difference between the two groups in OS or in distant metastasis-free rates.
👉Locoregional recurrence at 10 years was 12% for the mastectomy group and 20% for the breast-conserving therapy group.
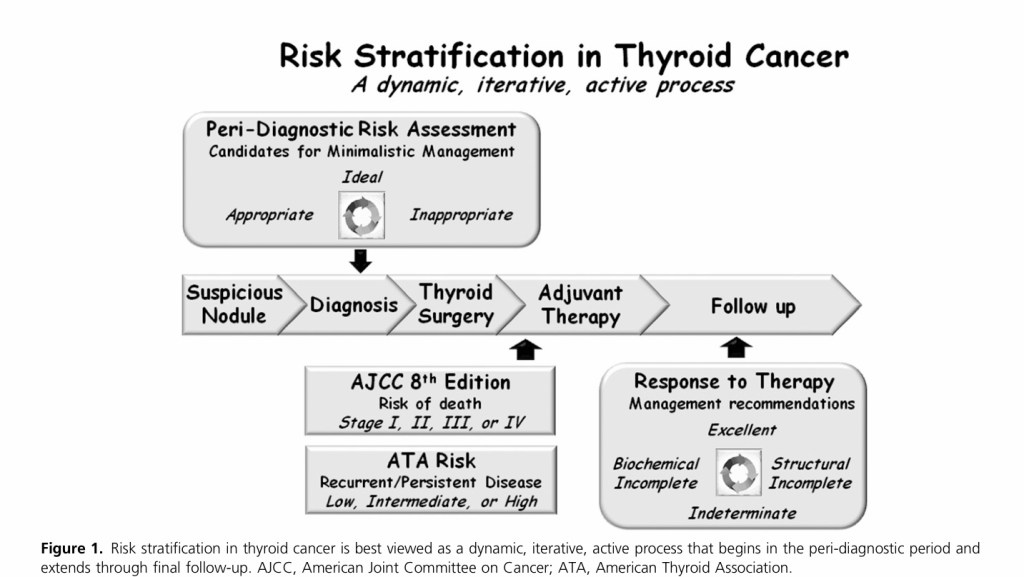
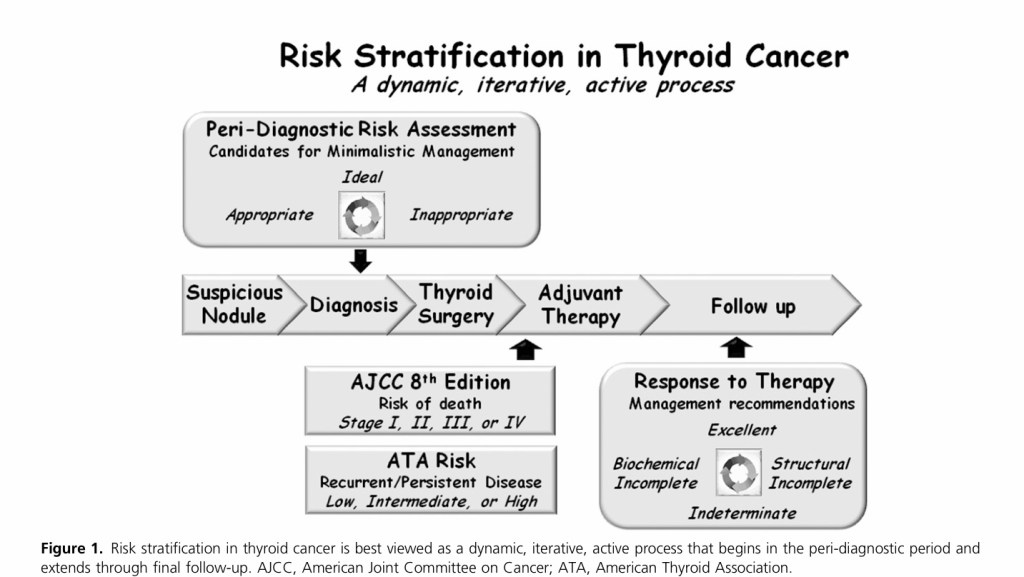
👉The modern view of risk stratificationbegins with the identification of a suspicious nodule (peri-diagnostic period) and continues through the phases of diagnosis, treatment, adjuvant therapy, and follow-up.
👉From a practical standpoint, postoperatively, we use the eighth edition of the American Joint Committee on Cancer/tumor node metastasis (AJCC/TNM) staging system to predict disease-specific mortality and the American Thyroid Association (ATA) risk stratification system to predict the risk of recurrent or persistent disease.
👉These initial risk estimates are then modified over time using the descriptions from the ATA guidelines to define the patients response to therapy at any point during follow-up, as excellent (no evidence of persistent / recurrent disease), biochemically incomplete [abnormal thyroglobulin (Tg) or rising Tg antibodies in the absence of identifiable structural disease], structurally incomplete (structural evidence of persistent / recurrent disease), or indeterminate (nonspecific findings that cannot be confidently classified as benign or malignant).
👉These modified risk estimates are then used to plan ongoing management.
👉Recently, the move toward deferred intervention (active surveillance) of very low-risk thyroid cancers and a more minimalistic approach to thyroid surgery has expanded the risk-stratification horizon to include not only the intraoperative and postoperative time periods but also the peri-diagnostic time frame that begins with the detection of a suspicious thyroid nodule.
👉In this peri-diagnostic period, it is important to identify low-risk thyroid cancers that may be eligible for either an active surveillance management approach (with or without cytological confirmation) or for a minimalistic surgical intervention, such as thyroid lobectomy without neck dissection.
👉Conversely, it is equally important to identify, in the peri-diagnostic period, those patients who would be most likely to benefit from more aggressive initial interventions that could include total thyroidectomy, with or without prophylactic or therapeutic neck dissection, radioactive iodine treatment, external beam radiation, or upfront systemic therapy.
👉The MILAN I trial compared 701 patients with invasive breast cancer up to 2 cm in size without clinically positive axillary lymph nodes and randomized them into those who received Halsted mastectomy and those who received quadrantectomy plus axillary dissection and radiotherapy.
👉A recent analysis of the trial showed no differences in OS between the two study groups.
It is presumed to be between 2 to 14 days after exposure, with most cases occurring within 5 days after exposure.
👉The spectrum of illness severity
Most infections are self limiting.
COVID-19 tends to cause more severe illness in elderly population or in patients with underlying medical problems.
As per the report from Chinese center for disease control and prevention that included approximately 44,500 confirmed infections with an estimation of disease severity:
Mild illness was reported in 81% patients
Severe illness was reported in 14% patients:
Definition of severe illness:
Hypoxemia
Greater than 50% lung involvement on imaging within 24 to 48 hours
Critical Disease was reported in 5% patients:
Definition of critical disease:
Respiratory failure
Shock
Multi-organ dysfunction syndrome
Overall case fatality rate was:
Between 2.3% to 5%
👉Age affected
• Mostly middle aged (>30 years) and elderly. • Symptomatic infection in children appears to be uncommon, and when it occurs, it is usually mild
👉Clinical Presentation
In a study describing 1099 patients with COVID-19 pneumonia in Wuhan, the most common clinical featuresat the onset of illness were:
Fever in 88%
Dry cough in 67%
Fatigue in 38%
Dyspnea in 18.7%
Myalgias in 14.9%
Pneumonia appears to be the most common and severe manifestation of infection:
In this group of patients breathing difficulty developed after a median of five days of illness.
Acute respiratory distress syndrome:
Developed in 3.4% of patients.
Other symptoms
Headache
Sore throat
Rhinorrhea
Gastrointestinal symptoms
About 80% of confirmed COVID-19 cases:
Suffer from only mild to moderate disease
Nearly 13% have severe disease:
Dyspnea
Respiratory frequency ≥ 30/minute
Blood oxygen saturation ≤ 93%
PaO2/FiO2 ratio less than 300
Lung infiltrates of greater than 50% of the lung filed within 24 to 48 hours
Critical illness is seen in approximately 6% of the cases:
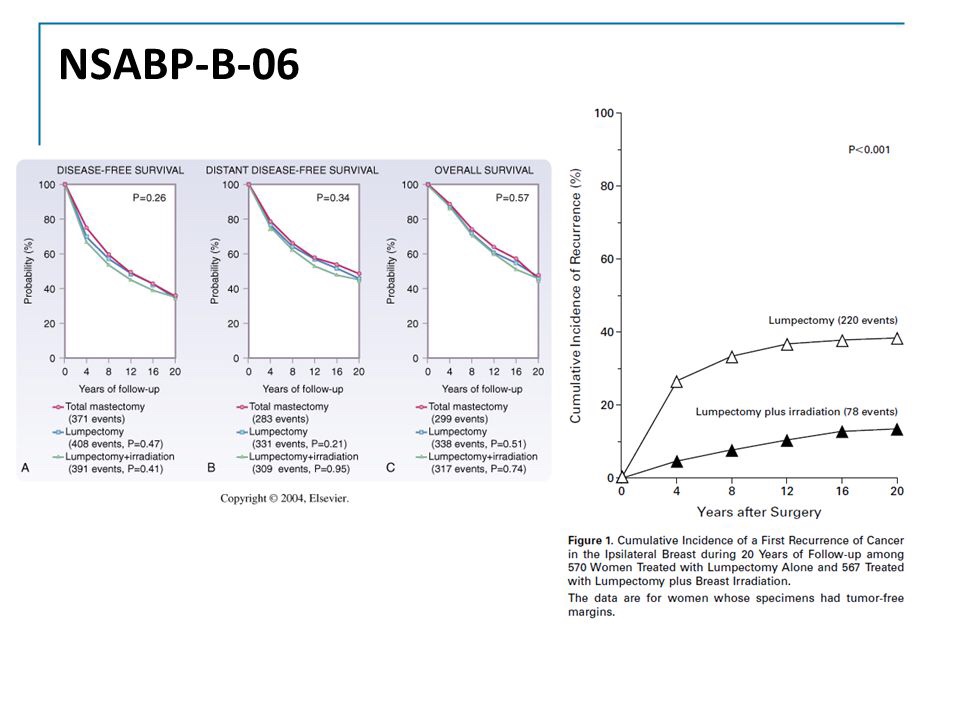
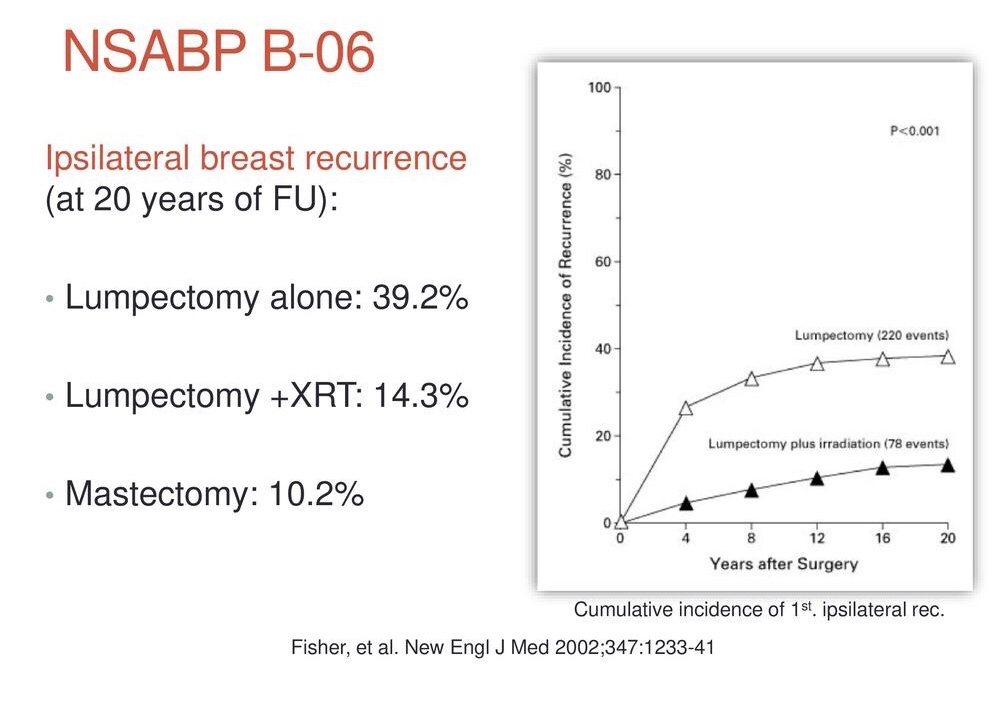
👉The NSABP B-06, Phase III Trial Total Mastectomy/Axillary Dissection vs Segmental Mastectomy/Axillary Dissection with or without Radiotherapy for Potentially Curable Breast Carcinoma.
👉Compared lumpectomy and axillary node dissection with or without breast irradiation with modified radical mastectomy (MRM) in patients with tumors 4 cm or less in greatest diameter.
👉After 20 years of follow-up, there are no observed differences in OS, or distant disease-free survival between the MRM group and the groups treated with breast-conserving surgery (BCS), with or without radiation.
👉The hazard ratio (HR) for death with BCS alone was 1.05 (95% confidence interval [CI], 0.90–1.23; P=0.51).
👉The HR for death with BCS plus radiation was 0.97 (95% CI, 0.83–1.14; P=0.74).
👉These are comparable to MRM.
👉The results of this trial demonstrating equivalent survival between the two surgical optionsestablish BCS as a viable surgical option for most patients with invasive breast cancer.
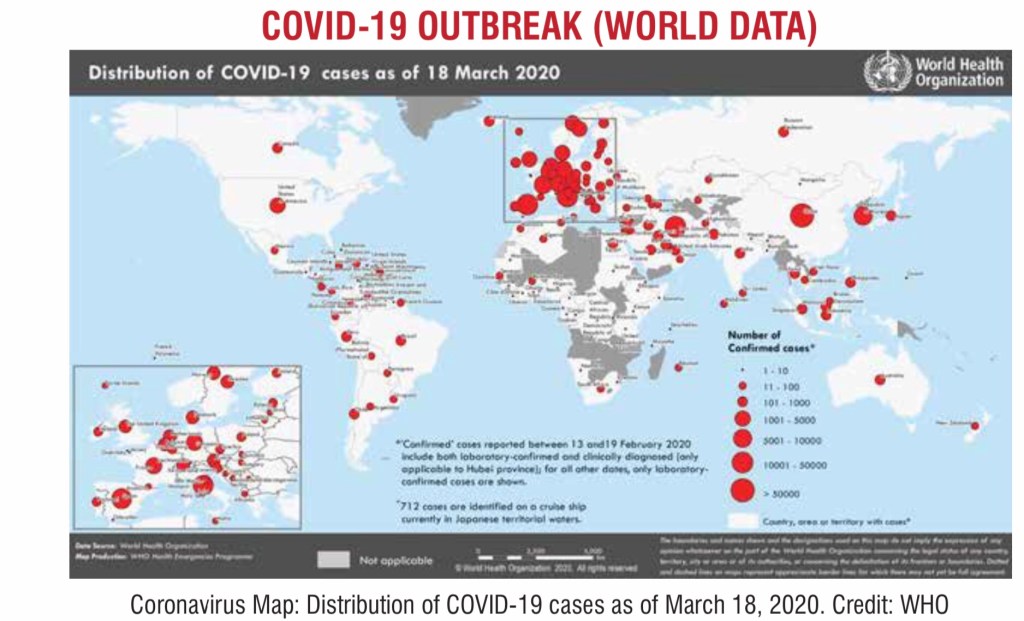
👉Since the first reports of cases from Wuhan, at the end of 2019, more than 80,000 COVID-19 cases have been reported in China; including all laboratory-confirmed cases as well as clinically diagnosed cases in the Hubei Province.
👉Increasing numbers of cases have also been reported in other countries across all continents except Antarctica.
👉The rate of new cases outside of Chinahas outpaced the rate in China which led world health organization (WHO) to declare COVID-19 as a pandemic.
👉Our understanding of the mode of transmission is currently incomplete.
👉Epidemiologic investigation in Wuhan at the beginning of the outbreak identified an initial association with a seafood market where most patients had worked or visited.
👉The seafood market also sold live rabbits, snakes and other animals.
👉The initial concept was that the virus originated from snakes, however later studies proved that it had more similarity with bats.
👉However, as the outbreak progressed, person-to-person transmission through droplets and fomites became the primary mode of transmission.
👉How does Person-to-person transmission occur?
👉Droplet transmission:
The virus is released in the respiratory secretions when an infected person coughs, sneezes or talks.
These droplets can infect others if they make direct contact with the mucous membranes.
Infection can also occur by touching an infected surface and followed by eyes, nose or mouth.
Droplets typically do not travel more than six feet (about two meters) and do not linger in the air.
However, given the current uncertainty regarding transmission mechanisms, airborne precautions are recommended routinely in some countries and in the setting of specific high risk procedures.
Patients are thought to be most contagious when they are symptomatic.
Some spread might be possible before symptoms appear, but this is not thought to be a common occurrence.
Other possible modes of transmission:
It may be possible that a person can get COVID-19 by touching a surface or object that has the virus on it and then touching their own mouth, nose, or possibly their eyes, but this is not thought to be the main way the virus spreads.
One study suggested that the virus may also be present in feces and could contaminate places like toilet bowls and bathroom sinks:
But the researchers noted the possibility of this being a mode of transmission needs more research.
In February a Chinese newborn was diagnosed with the new coronavirus just 30 hours after birth:
The baby’s mother tested positivebefore she gave birth.
It is unclear how the disease was transmitted – in the womb, or after birth.
Recently in London another newborn was tested positive for the coronavirus, marking what appears to be the second such case as the pandemic worsens.
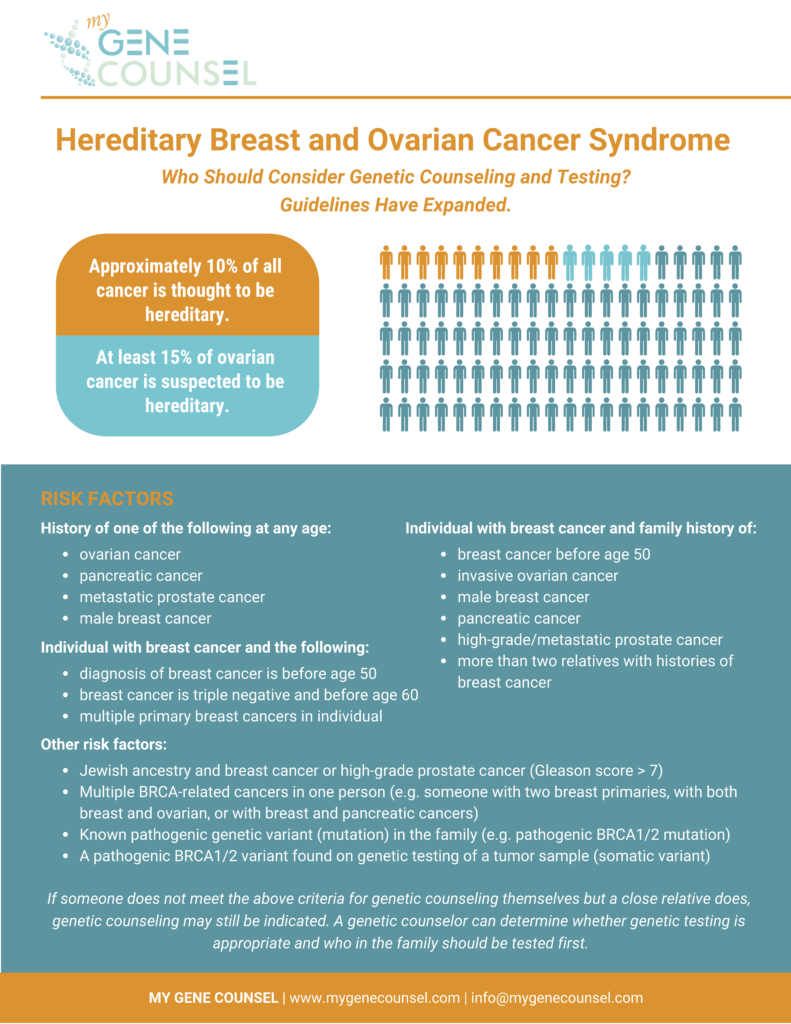
👉The National Comprehensive Cancer Network (NCCN) guidelines support genetic counseling for any woman diagnosed with early-onset breast cancer.
👉The current definition of early onset is age less than or equal to 50 year.
👉In addition, these guidelines support genetic counseling for any woman diagnosed with triple-negative breast cancer who is age 60 or younger.
👉This is because pathologic BRCA1 gene mutations are associated with basal-type triple-negative breast cancer.
👉The results of a genetic test would directly inform estimation of ipsilateral breast tumor recurrence risk with breast conservation, contralateral breast cancer risk, and risk for other cancers, such as ovarian cancer.
👉Genetic testing can be inexpensive depending on the provider.
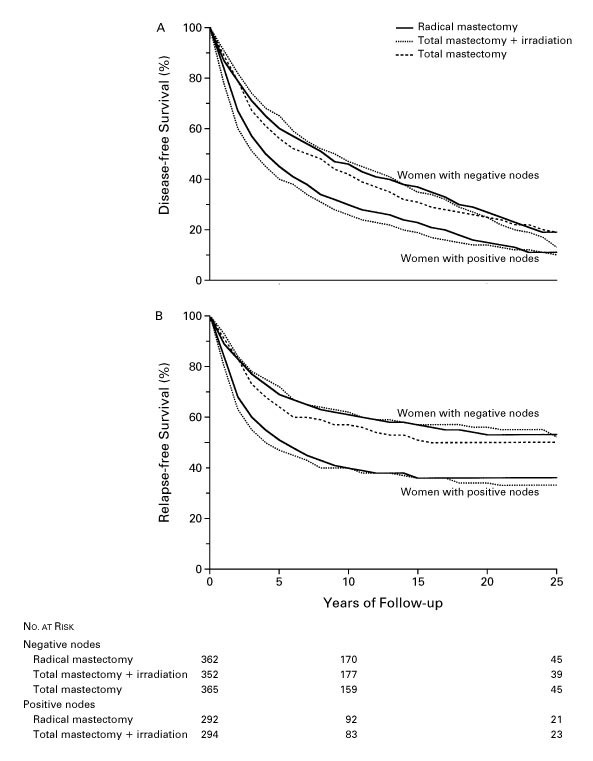
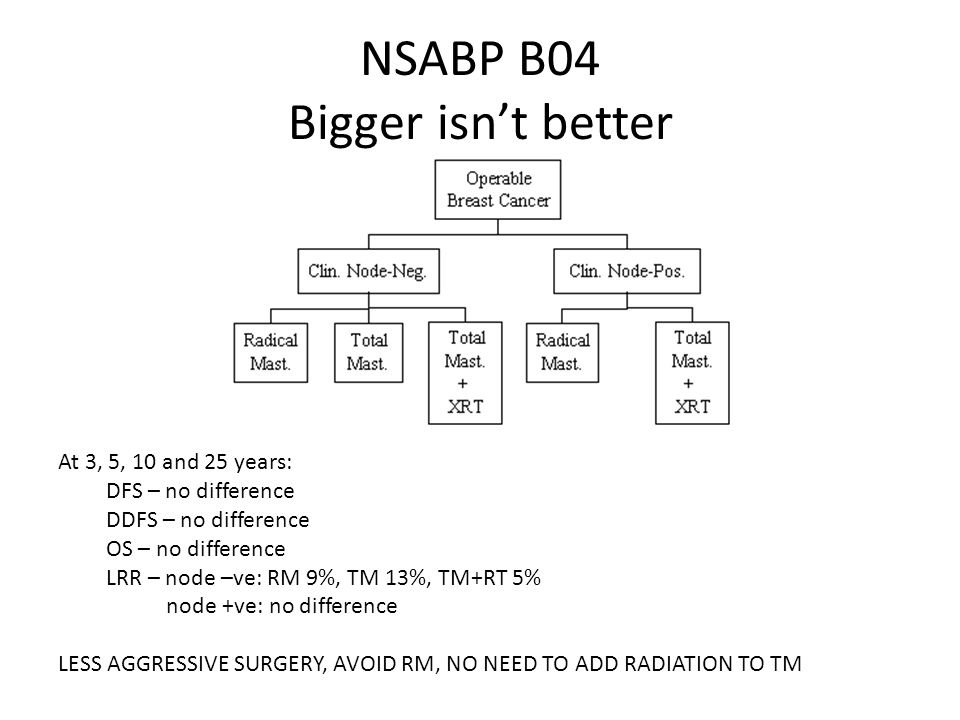
👉The NSABP B-04, A Protocol for the Evaluation of Radical Mastectomy (RM) and Total Mastectomy (TM) With and Without Radiation in the Primary Treatment of Cancer of the Female Breast.
👉It enrolled 1079 patients with clinically node-negative disease, and randomized them to RM, TM plus local-regional axillary irradiation, or TM alone.
👉In a parallel trial, 586 patients with clinically node-positive disease were randomized to RM or TM plus radiation.
👉After 25 years of follow-up, the study showed no significant difference in long-term outcome between clinically node-negative patients who received RM and those who received TM plus radiation, or between clinically node-positive patients who received RM and those who received TM with nodal irradiation.
👉When comparing the hazard ratio for death within the two arms, the results show no survival advantage from RM.
👉In patients with clinically node-negative disease, pathologic examination of the mastectomy specimen revealed that 40% of the patients had pathologically positive nodes.
👉However, because the axillary failure rate in the TM alone arm was only 19%, we are led to conclude that occult axillary disease may not always progress into clinically overt disease.
👉The similar overall survival (OS) among the three arms in this trial also indicates that an axillary dissection in this trial would be largely prophylactic, and the outcome would not be compromised should the dissection be deferred until there is clinical evidence of a diseased axilla.