- The first generation of larynx preservation chemotherapy trials:
- Appeared in the 1990s:
- They randomized patients into surgery and radiotherapy or to induction chemotherapy cycles of cisplatin / 5FU:
- Patients who responded to chemotherapy then received radiotherapy:
- With possible salvage surgery
- Patients who responded to chemotherapy then received radiotherapy:
- If they did not respond to the chemotherapy:
- They received surgery and postoperative radiotherapy
- They randomized patients into surgery and radiotherapy or to induction chemotherapy cycles of cisplatin / 5FU:
- Generally, the results of these studies showed:
- No significant difference in survival:
- Between the two treatment arms
- No significant difference in survival:
- The larynx was preserved in:
- 56% of patients undergoing the experimental chemoradiotherapy arm
- Appeared in the 1990s:
- In 2000, Pignon et al:
- Published a meta-analysis of the first generation of laryngeal preservation chemoradiotherapy trials:
- They included T3 laryngeal and hypopharyngeal cancers
- There was no statistically significant difference in overall survival:
- However, it is important to note:
- That there was a trend to benefit from surgery:
- Hazard ratio 1.19 intervals (0.97–1.46)
- Surgery ± radiotherapy:
- Resulted in overall survival of 45%:
- Compared to an overall survival from chemoradiotherapy of:
- 39%
- Compared to an overall survival from chemoradiotherapy of:
- Resulted in overall survival of 45%:
- 56% of those who survived with chemoradiotherapy:
- Managed to avoid laryngectomy:
- Giving an overall laryngectomy survival rate of:
- 23% at five years
- Giving an overall laryngectomy survival rate of:
- Managed to avoid laryngectomy:
- Patients treated with chemoradiotherapy:
- Had almost double the local recurrence rate:
- But less distant metastases than the patients treated with surgery
- Had almost double the local recurrence rate:
- Analysis of laryngeal cancer patients separately from hypopharyngeal cancer patients:
- Showed that laryngeal cancer patients in the surgical arm:
- Demonstrated a risk reduction of 32%:
- This suggests that advanced laryngeal tumors would be better treated with surgery than chemoradiotherapy:
- On the other hand, hypopharyngeal cancer patients showed no difference in survival between the two modalities of treatment
- Showed that laryngeal cancer patients in the surgical arm:
- That there was a trend to benefit from surgery:
- However, it is important to note:
- Published a meta-analysis of the first generation of laryngeal preservation chemoradiotherapy trials:
- The meta-analysis showed that the overall survival benefit from chemotherapy in addition to radiotherapy:
- Was 4% at five years
- Concomitant chemotherapy:
- Resulted in an 8% overall survival benefit:
- Compared to a 4% overall survival benefit from neoadjuvant chemoradiotherapy
- Resulted in an 8% overall survival benefit:
- Adjuvant chemoradiotherapy:
- Resulted in no overall survival benefit
- These findings have resulted in the adoption of concomitant chemoradiotherapy as the standard regimen for delivery of chemotherapy when treating laryngeal and pharyngeal cancers:
- Recently, an update of this meta-analysis confirmed an overall survival effect of 6.5% for concomitant chemoradiotherapy
- References:
- The Department of Veterans Affairs Laryngeal Cancer Study Group. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. New England Journal of Medicine 1991; 324: 1685–90.
- Pignon JP, Bourhis J, Domenge C, Designé L. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of Chemotherapy on Head and Neck Cancer. Lancet 2000; 355: 949–55.
- Pignon JP, le Maítre A, Maillard E et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiotherapy and Oncology 2009; 92: 4–14.
- Forastiere AA, Goepfert H, Maor M et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. New England Journal of Medicine 2003; 349: 2091–8.
Blog
Management of the Axilla in the Setting of Neoadjuvant Therapy for Breast Cancer
- Management of the axilla continues to evolve in the setting of neoadjuvant therapy
- Sentinel lymph node biopsy (SLNB) in clinically node-negative patients after neoadjuvant chemotherapy;
- Is feasible and accurate:
- A recent systematic review reported a pooled identification rate of:
- 96% and false negative rate of 6%
- These data do not differ from studies evaluating SLNB in early breast cancer without neoadjuvant chemotherapy
- 96% and false negative rate of 6%
- A recent systematic review reported a pooled identification rate of:
- Is feasible and accurate:
- Neoadjuvant chemotherapy can result in:
- Downstaging of the axilla
- Performing the SLNB after chemotherapy:
- Decreases the rate of finding a positive sentinel lymph node and subsequent axillary dissection
- The ACOSOG / Alliance Z1071 trial involved patients with initially node-positive disease and sought to determine the false negative rate for sentinel lymph node surgery following neoadjuvant chemotherapy in this group of patients:
- The false negative rate for the entire cohort was 12%:
- But on additional analysis, retrieval of at least two sentinel nodes and the previously biopsied node:
- Was associated with a false negative rate of 6.8%:
- Therefore, marking the biopsied node with a clip and documenting excision at time of SLNB is recommended
- Was associated with a false negative rate of 6.8%:
- But on additional analysis, retrieval of at least two sentinel nodes and the previously biopsied node:
- The false negative rate for the entire cohort was 12%:
- References:
- Geng C, Chen X, Pan X, Li J. The feasibility and accuracy of sentinel lymph node biopsy in initially clinically node-negative breast cancer after neoadjuvant chemotherapy: a systematic review and meta-analysis. PLoS One.2016;11(9):e0162605.
- Hunt KK, Yi M, Mittendorf EA et al. Sentinel lymph node surgery after neoadjuvant chemotherapy is accurate and reduces the need for axillary dissection in breast cancer patients. Ann Surg. 2009;250(4):558-566.
- Boughey JC, Suman VJ, Mittendorf EA, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (Alliance) clinical trial. JAMA. 2013;310(14):1455-1461.
- Boughey JC, Ballman KV, Le-Petross HT et al. identification and resection of clipped node decreases the false-negative rate of sentinel lymph node surgery in patients presenting with node-positive breast cancer (T0-T4, N1-N2) who receive neoadjuvant chemotherapy: results from ACOSOG Z1071 (Alliance). Ann Surg.2016;263(4):802-807.

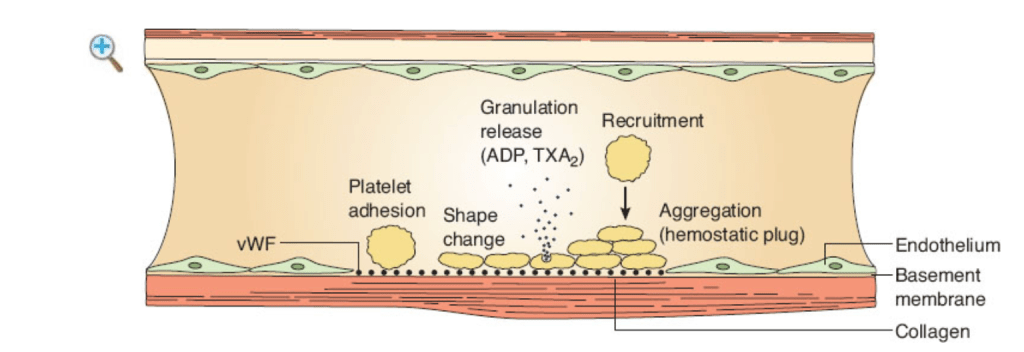
Primary Hemostasis
- The sequence (seconds → minutes):
- Vascular injury and vasoconstriction:
- Neurogenic reflex + endothelin:
- Transient narrowing:
- Slows flow and exposes subendothelial collagen and vWF
- Transient narrowing:
- Neurogenic reflex + endothelin:
- Platelet adhesion (to the wound):
- vWF anchored on exposed collagen binds GP Ib-IX-V on platelets (high-shear arterial beds):
- Platelet membrane glycoprotein Ib–IX–V complex:
- The major von Willebrand factor (vWF) receptor:
- That mediates initial platelet adhesion:
- At sites of vascular injury (especially high-shear arteries)
- That mediates initial platelet adhesion:
- The major von Willebrand factor (vWF) receptor:
- Platelet membrane glycoprotein Ib–IX–V complex:
- Direct collagen binding via GP Ia/IIa (α2β1) and GP VI:
- Complements adhesion
- vWF anchored on exposed collagen binds GP Ib-IX-V on platelets (high-shear arterial beds):
- Activation and shape change:
- Cytoskeleton rearranges:
- Discoid → spiky:
- ↑ surface area:
- Phosphatidylserine flips outward
- ↑ surface area:
- Discoid → spiky:
- Platelets synthesize / release mediators:
- Dense granules:
- ADP, ATP, Ca²⁺, serotonin
- Alpha granules:
- vWF, fibrinogen, factor V, fibronectin, P-selectin, PDGF, TGF-β
- TxA₂ is generated via:
- COX-1 (aspirin target)
- Dense granules:
- Cytoskeleton rearranges:
- Recruitment (amplification):
- ADP → P2Y12/P2Y1, TxA₂ (TP receptor), thrombin (PAR-1 / PAR-4):
- Amplify activation on nearby platelets
- Ca²⁺ is essential for signaling and integrin activation
- ADP → P2Y12/P2Y1, TxA₂ (TP receptor), thrombin (PAR-1 / PAR-4):
- Aggregation (hemostatic plug formation):
- Activated GP IIb/IIIa (αIIbβ3) undergoes conformational change:
- Fibrinogen bridges adjacent platelets:
- Primary hemostatic plug
- Fibrinogen bridges adjacent platelets:
- Leukocytes tether via P-selectin:
- Adding stability
- Handoff to secondary hemostasis (minutes):
- Tissue factor (injured cells) plus factor VII:
- Activate factor X :
- Factor X plus factor V:
- Convert prothrombin (factor II) to thrombin:
- Converts fibrinogen to fibrin polymer:
- Factor XIII crosslinks fibrin:
- Stabilizing the platelet plug
- Factor XIII crosslinks fibrin:
- Converts fibrinogen to fibrin polymer:
- Convert prothrombin (factor II) to thrombin:
- Factor X plus factor V:
- Activate factor X :
- Tissue factor (injured cells) plus factor VII:
- Activated GP IIb/IIIa (αIIbβ3) undergoes conformational change:
- Vascular injury and vasoconstriction:
- Why surgeons care (pattern recognition):
- Primary (platelet) defects:
- Mucocutaneous bleeding, oozing from raw surfaces, petechiae, immediate post-incision bleeding
- PT / PTT often normal
- Secondary (coagulation) defects:
- Delayed re-bleeding, deep tissue / hematoma, hemarthrosis
- Primary (platelet) defects:
- Drugs and diseases mapped to the steps:
- Adhesion:
- ↓ vWF (von Willebrand disease) → poor GP Ib-vWF “tether”:
- DDAVP can ↑ endothelial vWF release (Type 1 vWD, some qualitative defects)
- ↓ vWF (von Willebrand disease) → poor GP Ib-vWF “tether”:
- Activation:
- Aspirin / NSAIDs → block COX-1 → TxA₂ (qualitative dysfunction)
- Uremia, hypothermia, acidosis, hemodilution / CPB:
- Global platelet dysfunction
- DDAVP helps in uremia
- Recruitment:
- P2Y12 inhibitors (clopidogrel, prasugrel, ticagrelor) blunt ADP signaling
- Aggregation:
- Gp IIb/IIIa antagonists (eptifibatide/tirofiban) block fibrinogen bridging
- Glanzmann thrombasthenia (GP IIb/IIIa deficiency):
- Severe aggregation defect
- Bernard–Soulier (GP Ib deficiency):
- Adhesion failure; giant platelets
- Adhesion:
- Practical peri-op numbers (rules of thumb):
- Platelet count targets (institutional policies vary):
- Most non-neurosurgical / non-ocular operations:
- ≥ 50k/µL
- Neuraxial, intracranial, posterior eye:
- ≥ 80 to 100k/µL
- Ongoing microvascular free-flap or diffuse oozing often needs:
- > 75 to 100k/µL and intact function
- Most non-neurosurgical / non-ocular operations:
- Apheresis platelets:
- Typically ↑ count by ~ 30 to 50k/µL in a 70-kg adult
- Coordinate any antiplatelet interruption with cardiology (especially recent stents):
- If drugs cannot be stopped, plan local / topical strategies and consider point-of-care testing
- Platelet count targets (institutional policies vary):
- OR playbook for platelet-type bleeding:
- Pre-op:
- Focused history (mucosal bleeding, easy bruising), meds (aspirin, P2Y12), renal function
- Consider PFA-100/VerifyNow/TEG-PlateletMapping if results will change management
- Intra-op:
- Local control:
- Meticulous pressure, bipolar, vessel loops; topical hemostats (thrombin, gelatin sponge, oxidized cellulose, collagen matrix, fibrin sealant)
- Antifibrinolytics:
- Tranexamic acid (IV / topical) particularly helpful on mucosal fields (head and neck, oral cavity)
- Maintain normothermia, ionized Ca²⁺, pH > 7.2; avoid hemodilution
- If on aspirin / P2Y12 with urgent bleeding:
- Platelet transfusion can overcome irreversible blockade (earlier works better for aspirin than ticagrelor); weigh thrombosis risk
- DDAVP for vWD Type 1 or uremic dysfunction (watch Na⁺; tachyphylaxis after 1 to 2 doses)
- Local control:
- Post-op:
- Control blood pressure, avoid NSAIDs, continue local antifibrinolytics when helpful (e.g., pledgets / mouthwash in mucosal cases), and reassess platelet count / function if oozing persists
- Pre-op:
- Quick differentials when the field won’t dry:
- Normal PT / PTT, low platelets or recent antiplatelet use → primary hemostasis problem
- Prolonged PT / PTT, normal platelets → secondary hemostasis issue (think tissue factor pathway, anticoagulants)
- Everything “normal,” but diffuse oozing → platelet dysfunction (uremia, hypothermia, CPB, meds) ± hyperfibrinolysis (consider TXA, fibrinogen / cryoprecipitate guided by TEG/ROTEM)

Normal Coagulation and Normal Anticoagulation
- Normal coagulation (hemostasis):
- Three initial responses to vascular injury:
- Vasoconstriction:
- Neurohumoral + endothelin
- Platelet adhesion / activation / aggregation:
- Primary hemostasis
- Thrombin generation:
- That leads to fibrin clot formation:
- Secondary hemostasis NCBI+1
- That leads to fibrin clot formation:
- Vasoconstriction:
- Three initial responses to vascular injury:
- Primary hemostasis – what actually happens:
- Adhesion:
- VWF bridges exposed subendothelial collagen to platelet GPIb-IX-V (high shear)
- Collagen also signals via:
- GPVI and α2β1 (GPIa/IIa) NCBI+1
- Activation + secretion:
- Shape change
- Dense granule:
- ADP and TxA₂ amplify recruitment
- Surface phosphatidylserine (PF3) flips out:
- Creating a catalytic platform for coagulation enzymes NCBI
- Aggregation:
- Inside-out signaling activates:
- αIIbβ3 (GPIIb/IIIa)
- Fibrinogen (and later fibrin) bridges adjacent platelets:
- Platelet plug NCBI+1
- Inside-out signaling activates:
- Key receptors to remember:
- ADP → P2Y12 / P2Y1
- TxA₂ → TP
- Thrombin → PAR-1 / PAR-4(and also binds GPIbα) NCBI+2PubMed+2
- Secondary hemostasis – complexes and convergence:
- Tenase complexes:
- Extrinsic:
- Tissue factor (TF) from injured cells – factor VIIa:
- Plus Ca²⁺, membrane:
- Activates factor X
- Plus Ca²⁺, membrane:
- Tissue factor (TF) from injured cells – factor VIIa:
- Intrinsic:
- Exposed collagen + prekallikrein + HMW Kininigen = Factor XII:
- Activate Factor XI:
- Activate factor IXa – then add factor VIIIa:
- Plus Ca²⁺, membrane:
- Powerfully activates factor X (major amplifier)
- Plus Ca²⁺, membrane:
- Activate factor IXa – then add factor VIIIa:
- Activate Factor XI:
- Exposed collagen + prekallikrein + HMW Kininigen = Factor XII:
- Factor X:
- Is the common convergence point NCBI+1
- Prothrombinase complex (correct name for what forms on platelets):
- Factor Xa + factor Va + Ca²⁺ + anionic phospholipid (PF3):
- Converts prothrombin (factor II) to thrombin (factor IIa) NCBI
- Thrombin – central protease (know these):
- Converts fibrinogen → fibrin,
- Thrombin – central protease (know these):
- Converts prothrombin (factor II) to thrombin (factor IIa) NCBI
- Activates factor V, factor VIII, factor XI, factor XIII
- Strongly activates platelets via PAR-1 / PAR-4
- When bound to thrombomodulin:
- Activates protein C (anticoagulant pathway) NCBI+1
- Factor Xa + factor Va + Ca²⁺ + anionic phospholipid (PF3):
- Factor XIII:
- A transglutaminase that crosslinks fibrin and incorporates α2-antiplasmin into the clot:
- Producing stability and resistance to fibrinolysis NCBI
- A transglutaminase that crosslinks fibrin and incorporates α2-antiplasmin into the clot:
- Extrinsic:
- Tenase complexes:
- Adhesion:
- Fibrin’s role with platelets:
- Fibrin(ogen) binds αIIbβ3, linking platelets and stabilizing the plug as fibrin polymerizes and is cross-linked Haematologica
- Normal anticoagulation (checks and balances)
- Antithrombin (AT-III):
- Key serpin that neutralizes:
- Thrombin (IIa), IXa, Xa, XIa, XIIa
- Key serpin that neutralizes:
- Heparin / Heparan sulfate:
- Accelerates AT-III activity dramatically (clinical basis of UFH /LMWH) NCBI+1
- Protein C / Protein S (vitamin K–dependent):
- Thrombin – thrombomodulin on endothelium:
- Activates protein C:
- Which (with protein S cofactor) proteolytically inactivates Va and VIIIa (not fibrinogen)
- Activates protein C:
- Thrombin – thrombomodulin on endothelium:
- TFPI (tissue factor pathway inhibitor):
- Endothelium-derived inhibitor:
- That inactivates factor Xa and, in an factor Xa – dependent manner:
- Shuts down TF – FVIIa:
- The dominant brake on the initiation phase
- Shuts down TF – FVIIa:
- That inactivates factor Xa and, in an factor Xa – dependent manner:
- Protein S enhances TFPIα’s factor Xa inhibition:
- Nuance:
- TFPI does not simply “inhibit factor X”; it inhibits factor Xa and the TF – FVIIa complex NCBI+2ASA Journals+2
- Nuance:
- Endothelium-derived inhibitor:
- Endothelial antithrombotic tone (nice to remember):
- PGI₂, NO, and CD39 (ecto-ADPase) limit platelet activation
- Heparan sulfate potentiates AT
- Antithrombin (AT-III):
- Fibrinolysis (clot removal):
- tPA / uPA (primarily from endothelium) convert plasminogen → plasmin:
- Preferentially on fibrin-rich surfaces
- Plasmin:
- Degrades fibrin and fibrinogen → FDPs (D-dimer reflects cross-linked fibrin breakdown) NCBI+1
- Major inhibitors / regulators:
- PAI-1 (± PAI-2):
- Inhibit tPA / uPA
- α2-antiplasmin:
- Neutralizes plasmin and is cross-linked to fibrin by factor XIII
- TAFI (activated by thrombin – thrombomodulin) trims C-terminal lysines from fibrin, reducing plasminogen / tPA binding and slowing lysis NCBI+2PubMed+2
- PAI-1 (± PAI-2):
- tPA / uPA (primarily from endothelium) convert plasminogen → plasmin:
Management of Locally Advanced Laryngeal Carcinoma
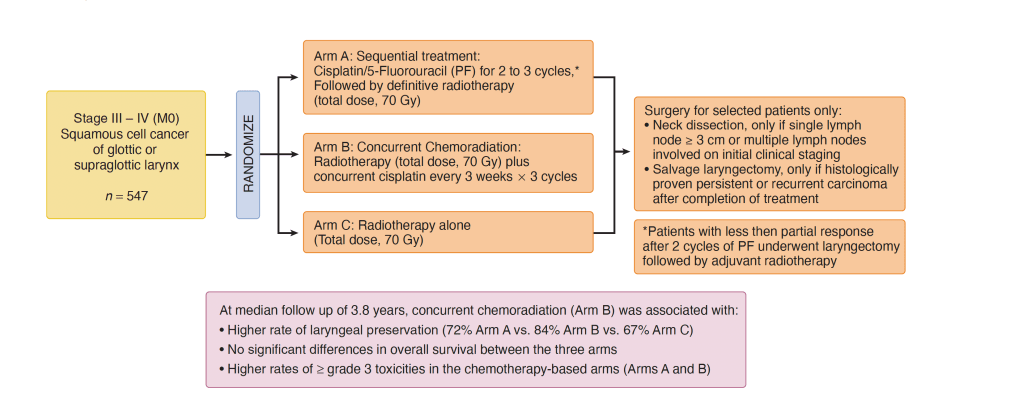
- The intergroup Radiation Therapy Oncology Group (RTOG 91–11) trial for advanced larynx cancer established:
- Concurrent bolus cisplatin with radiation as a standard of care
- I mentioned that the study was open to patients with squamous cell carcinoma of the glottic or supraglottic larynx:
- Patients with T1 disease or large-volume T4 disease were excluded
- Patients were randomly assigned to one of three larynx preservation strategies:
- Induction cisplatin plus 5-FU followed by radiotherapy
- Radiotherapy with concurrent cisplatin
- Radiotherapy alone
- I mentioned that the dose of radiotherapy to the primary tumor and clinically positive nodes was:
- 70 Gy in all treatment groups
- Severe or life-threatening mucositis in the radiation field was:
- Almost twice as common in the concurrent treatment group compared with either the radiotherapy alone group or the sequential treatment group
- The primary endpoint of the study was:
- Preservation of the larynx
- The rate of laryngeal preservation was:
- 84% for patients receiving radiotherapy with concurrent cisplatin versus 72% or patients receiving induction chemotherapy followed by radiation and 67% for patients receiving radiation therapy alone:
- At a median follow-up of 3.8 years
- 84% for patients receiving radiotherapy with concurrent cisplatin versus 72% or patients receiving induction chemotherapy followed by radiation and 67% for patients receiving radiation therapy alone:
- Distant metastases were reduced:
- In patients who received either concurrent chemoradiotherapy or induction chemotherapy followed by radiotherapy compared with patients who received radiotherapy alone
- Overall survival:
- Was not significantly different among the three treatment groups
- The lack of an overall survival difference between the three groups:
- May be due to the contribution of salvage laryngectomy in all groups, as well as a 2% increase in the incidence of death that may have been related to treatment in the concurrent chemoradiotherapy group compared with the other two treatment groups:
- It is important to recognize that the primary endpoint of the study was larynx preservation:
- Not overall survival
- It is important to recognize that the primary endpoint of the study was larynx preservation:
- May be due to the contribution of salvage laryngectomy in all groups, as well as a 2% increase in the incidence of death that may have been related to treatment in the concurrent chemoradiotherapy group compared with the other two treatment groups:
- The current standard of care for larynx preservation remains:
- Concurrent high-dose cisplatin and radiation for patients who fit the eligibility criteria that were used in RTOG 91–11
chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349:2091–2098.)
Molecular Subtypes of Breast Cancer
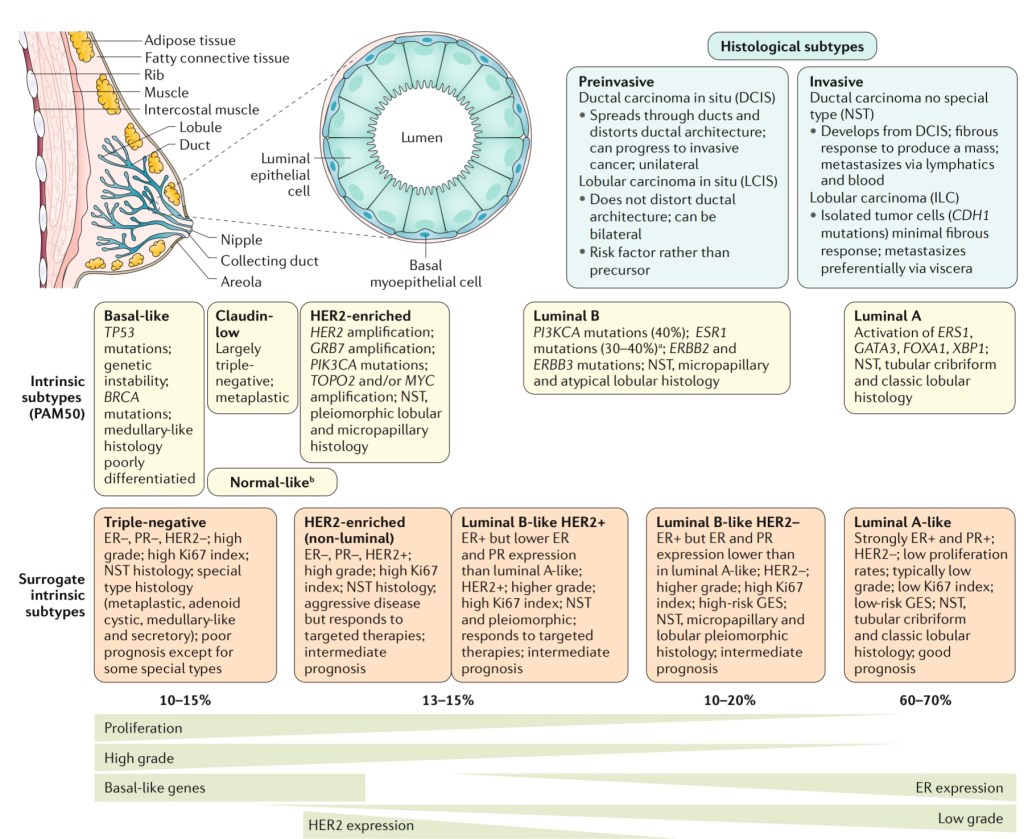
- Perhaps one of the most striking advances in breast cancer management and understanding:
- Came with the molecular profiling of breast cancer:
- Characterizing four distinct subtypes:
- Based on the landmark paper by Perou et al., in 2000
- Characterizing four distinct subtypes:
- Came with the molecular profiling of breast cancer:
- These define tumor biology and correlate with outcome and are broadly described as:
- Luminal A, luminal B, human epidermal growth factor receptor 2 (HER2)-enriched, and basal like:
- According to the most common profiles for each subtype:
- However, not all tumors within each subtype contain all features
- According to the most common profiles for each subtype:
- Luminal A, luminal B, human epidermal growth factor receptor 2 (HER2)-enriched, and basal like:
- The estrogen receptor (ER), progesterone receptor (PR), and HER2 receptor:
- Are used as surrogates to approximate these subtypes and guide clinical care and management decisions
- Luminal A:
- Most (80% to 85%) of breast cancers express the estrogen receptor (ER-positive) and / or the progesterone receptor (PR+) (75% to 80%) but not HER2:
- These cancers tend to be more indolent than other subtypes
- Luminal A tumors are associated with the most favorable prognosis:
- Particularly in the short term:
- In part because expression of hormone receptors:
- Is predictive of a favorable response to hormonal therapy
- In part because expression of hormone receptors:
- Particularly in the short term:
- Most (80% to 85%) of breast cancers express the estrogen receptor (ER-positive) and / or the progesterone receptor (PR+) (75% to 80%) but not HER2:
- Luminal B:
- These breast cancers are ER-positive and / or PR+:
- They are further defined by either:
- HER2 amplification, or high Ki-67 (an indicator of cellular proliferation)
- They are further defined by either:
- They tend to have higher grade and more aggressive features than luminal A breast cancers
- These breast cancers are ER-positive and / or PR+:
- HER2-enriched:
- These breast cancers produce excess HER2 and do not express hormone receptors
- These cancers tend to grow and spread more aggressively than other breast cancers and are associated with poorer short-term prognosis compared to ER-positive breast cancers:
- However, the recent widespread use of targeted therapies for HER2-positive cancers:
- Has reversed much of the adverse prognostic impact of HER2 overexpression:
- With 40% to 70% of women achieving a pathologic complete response to combination chemotherapy and targeted anti-HER2 therapies
- Has reversed much of the adverse prognostic impact of HER2 overexpression:
- However, the recent widespread use of targeted therapies for HER2-positive cancers:
- Basal like:
- These tumors are more biologically aggressive:
- They are typically characterized by the lack of the ER, PR, and HER2 receptor
- These cancers are often found in:
- Premenopausal women
- Those with a BRCA1 gene mutation
- They are nearly two times more common:
- In Black women than White women in US
- The majority (> 70%) of triple negative breast cancers:
- Fall into the basal-like subtype
- Triple negative breast cancers:
- Have a poorer short-term prognosis than other breast cancer types:
- In part because there are currently no targeted therapies for these tumors:
- However, a proportion of these tumors are very chemosensitive, exhibiting a pathologic complete response in up to a third of patients
- In part because there are currently no targeted therapies for these tumors:
- Furthermore, several molecular subtypes of triple negative breast cancer have been described:
- These may provide further insights into the varying biologic response and assist in development of therapeutic targets in addition to chemotherapy
- Have a poorer short-term prognosis than other breast cancer types:
- These tumors are more biologically aggressive:
Staging of the Axilla Following Neoadjuvant Chemotherapy
- As reported by Veronesi in 1999:
- 737 patients were randomized to either undergo Halsted mastectomy or extended mastectomy with IM node dissection
- After 30 years of follow-up:
- There was no difference in overall survival or disease-specific survival:
- For the patients eligible with T1, T2, T3, N0, and N1 disease:
- Who underwent IM node dissection vs. no IM dissection
- For the patients eligible with T1, T2, T3, N0, and N1 disease:
- There was no difference in overall survival or disease-specific survival:
- A 2019 retrospective review of 95 breast cancer patients with clinically detected IM nodes (IMNs) at diagnosis:
- Were treated with surgery and radiation, with median follow-up of 43 months:
- 77 received neoadjuvant chemotherapy:
- With IMN normalization in 67.5%
- Partial IMN response in 24.6%
- 77 received neoadjuvant chemotherapy:
- The 5-year IMN failure-free survival, disease-free survival, and overall survival were:
- 96%, 70%, and 84%, respectively
- IMN failure-free survival:
- Was significantly affected by:
- Resection margin status
- Size of IMN
- Receipt of IMN boost radiation
- Was significantly affected by:
- IMN failure-free survival:
- Were treated with surgery and radiation, with median follow-up of 43 months:
- A recently published meta-analysis in the Annals of Surgery found that axillary staging following neoadjuvant chemotherapy:
- Is best performed with a combination approach of sentinel lymph node biopsy (SLNB) with excision of the pre-chemotherapy-marked positive node:
- With a false negative rate of 2% to 4%:
- The identification rate was 100%
- With a false negative rate of 2% to 4%:
- Is best performed with a combination approach of sentinel lymph node biopsy (SLNB) with excision of the pre-chemotherapy-marked positive node:
- ACOSOG Z1071:
- Reported an overall false negative rate of 12.6% when SLNB was performed after neoadjuvant chemotherapy with documented node-positive disease prior to treatment:
- The false-negative rate decreased to 6.8%:
- When both sentinel node(s) and the clipped node were retrieved at the time of surgery
- Reported an overall false negative rate of 12.6% when SLNB was performed after neoadjuvant chemotherapy with documented node-positive disease prior to treatment:
- References:
- Veronesi U, Marubini E, Mariani L, Valagussa P, Zucali R. The dissection of internal mammary nodes does not improve the survival of breast cancer patients. 30-year results of a randomised trial. Eur J Cancer. 1999;35(9):1320-1325.
- Kim J, Chang JS, Choi SH, et.al. Radiotherapy for initial clinically positive internal mammary nodes in breast cancer. Radiat Oncol J. 2019;37(2):91-100.
- Simons JM, van Nijnatten TJA, van der Pol CC, Luiten EJT, Koppert LB, Smidt ML. Diagnostic accuracy of different surgical procedures for axillary staging after neoadjuvant systemic therapy in node-positive breast cancer: a systematic review and meta-analysis. Ann Surg. 2019;269(3):432-442.
- Boughey JC, Ballman KV, Le-Petross HT, et al. Identification and resection of clipped node decreases the false-negative rate of sentinel lymph node surgery in patients presenting with nodepositive breast cancer (T0-T4, N1-N2) who receive neoadjuvant chemotherapy: results from ACOSOG Z1071 (Alliance). Ann Surg. 2016;263(5):802-807.

RTOG 91-11: Landmark Organ-Preservation Trial in Advanced Laryngeal Cancer
- Design and Arms:
- Population:
- 547 patients with stage III to IV (cT2 bulky to cT4) resectable squamous cell carcinoma of the larynx(supraglottic or glottic):
- Who were candidates for total laryngectomy
- 547 patients with stage III to IV (cT2 bulky to cT4) resectable squamous cell carcinoma of the larynx(supraglottic or glottic):
- Population:
- Randomization (3 arms):
- Induction PF → RT (Control):
- Three cycles cisplatin 100 mg / m² day 1 + 5-FU 1 g/m²/day × 5, followed by definitive RT (66 to 76 Gy) for responders
- Concurrent CRT:
- RT (70 Gy) + cisplatin 100 mg / m² q3wk ×3
- RT Alone:
- 70 Gy definitive radiation
- Induction PF → RT (Control):
- Primary endpoint:
- Laryngectomy-free survival (LFS) and larynx preservation without loss of overall survival (OS)

- Interpretation:
- Concurrent cisplatin-RT produced the highest larynx-preservation rate and superior laryngectomy-free survival compared with both RT alone and induction PF
- No OS advantage for any arm:
- Survival curves overlapped
- Long-Term and Late Toxicities (Forastiere et al., JCO 2013 update):
- Non–cancer deaths:
- Cardiopulmonary, treatment-related:
- More frequent in the concurrent CRT arm after year 5
- Cardiopulmonary, treatment-related:
- Late swallowing dysfunction and chronic aspiration:
- Higher with CRT
- Highlights need for lifelong surveillance and aggressive supportive care:
- Speech / swallow therapy
- Pulmonary monitoring
- Non–cancer deaths:
- Clinical Application:
- Standard of care for organ preservation:
- Definitive RT + high-dose cisplatin (100 mg / m² q3wk ×3):
- For patients who are surgical candidates but wish to avoid total laryngectomy and are cisplatin-eligible
- Requires baseline audiogram, renal function, and performance status assessment
- Definitive RT + high-dose cisplatin (100 mg / m² q3wk ×3):
- Alternatives:
- For cisplatin-ineligible patients:
- Cetuximab-RT or carboplatin-based CRT:
- With the understanding of lower organ-preservation rates
- Cetuximab-RT or carboplatin-based CRT:
- For cisplatin-ineligible patients:
- Standard of care for organ preservation:
Cisplatin-Ineligible Unresected Disease – Most Guideline – Concordant Radiation (RT) Partner?
- Cisplatin-ineligible unresected disease:
- Most guideline-concordant RT partner:
- Cetuximab
- Most guideline-concordant RT partner:
- Anchor trials and what they show:
- Proof that EGFR antibody + RT beats RT alone:
- Establishes cetuximab as a curative RT partner
- Bonner et al., NEJM 2006; 5-yr update 2010:
- In locoregionally advanced, unresected HNSCC, adding cetuximab to definitive RT over RT alone improved:
- Locoregional control:
- Median 24.4 months vs 14.9 months:
- HR 0.68, p=0.005 over RT alone
- Median 24.4 months vs 14.9 months:
- Overall survival:
- Median 49.0 months vs 29.3 months:
- HR 0.74, p=0.03 over RT alone
- Median 49.0 months vs 29.3 months:
- This occured without excess severe mucositis
- Locoregional control:
- This is the randomized dataset that legitimized cetuximab as a radiosensitizer when chemotherapy can’t be given:
- In locoregionally advanced, unresected HNSCC, adding cetuximab to definitive RT over RT alone improved:
- Proof that substituting cetuximab for cisplatin is harmful in HPV+ OPSCC:
- So only use when truly ineligible
- Trials:
- RTOG-1016 (Lancet 2019):
- RT + cetuximab failed non-inferiority vs RT + cisplatin
- It produced worse OS and PFS in HPV-positive OPSCC
- Investigators conclude cisplatin remains the standard for eligible patients:
- De-ESCALaTE HPV (Lancet 2019):
- Similarly showed inferior OS and higher recurrence with cetuximab – RT vs cisplatin – RT:
- Ending the practice of “de-escalation by substitution”
- Similarly showed inferior OS and higher recurrence with cetuximab – RT vs cisplatin – RT:
- RTOG-1016 (Lancet 2019):
- Attempts to replace cetuximab in the cisplatin-ineligible setting haven’t beaten it:
- NRG-HN004 (2024):
- In patients contraindicated for cisplatin, RT + durvalumab:
- Did not improve outcomes over RT + cetuximab:
- Cetuximab – RT remained the reference:
- Did not improve outcomes over RT + cetuximab:
- In patients contraindicated for cisplatin, RT + durvalumab:
- NRG-HN004 (2024):
- Proof that EGFR antibody + RT beats RT alone:
- Guideline through-line (how this translates to practice):
- NCCN (2025):
- For definitive management when cisplatin is contraindicated:
- For example:
- Renal dysfunction, grade ≥ 2 SNHL, significant neuropathy
- RT + cetuximab is a listed option:
- Substitution for convenience or “de-escalation”;
- Is not recommended given RTOG-1016 / De-ESCALaTE trials;
- Substitution for convenience or “de-escalation”;
- For example:
- For definitive management when cisplatin is contraindicated:
- NCCN (2025):
- Practical takeaways for your pathway:
- Most guideline – concordant partner when cisplatin is off the table:
- Cetuximab with RT:
- Supported by the only randomized trial showing benefit over RT alone (Bonner) PubMed
- Cetuximab with RT:
- Do not swap out cisplatin in HPV+ disease unless truly ineligible:
- Expect worse survival with substitution PubMed+1
- If cetuximab isn’t feasible:
- Severe infusion reactions:
- Some centers use carboplatin – based CRT (often AUC 1–2 weekly ± partner):
- But high-level randomized evidence with RT is limited relative to cetuximab:
- Data are mainly retrospective / phase II (Guideline nuances vary by site and risk) Cancer Treatment Reviews
- But high-level randomized evidence with RT is limited relative to cetuximab:
- Some centers use carboplatin – based CRT (often AUC 1–2 weekly ± partner):
- Severe infusion reactions:
- Most guideline – concordant partner when cisplatin is off the table:
- Bottom line:
- In cisplatin-ineligible, unresected HNSCC:
- RT + cetuximab remains the most evidence-based, guideline-aligned radiosensitizer:
- Chosen because it improves outcomes vs RT alone:
- While trials show it must not replace cisplatin in eligible HPV+ patients
- Chosen because it improves outcomes vs RT alone:
- RT + cetuximab remains the most evidence-based, guideline-aligned radiosensitizer:
- In cisplatin-ineligible, unresected HNSCC:

Diffusely Invasive Breast Cancer
- Diffusely invasive carcinoma:
- Has a mammographic appearance of diffuse architectural distortion:
- Usually involving a large area, often larger than a lobe:
- With no central tumor mass and no calcifications:
-
- It sometimes has the appearance of a “spider’s web” as shown in the Image
- Usually involving a large area, often larger than a lobe:
- Has a mammographic appearance of diffuse architectural distortion:

- The diffusely infiltrating cancer:
- Forms concave contours with the surrounding fat in a manner similar to normal fibroglandular tissue (Images)

- The imaging findings of diffusely infiltrating breast cancer are strikingly different:
- From the imaging findings of breast cancers originating either from the terminal ductal lobular units (TDLUs) or the lactiferous ducts:
-
- Suggesting that it may have a different site of origin
- It has been recently proposed that diffusely infiltrating breast cancers:
- May originate from mesenchymal stem cells (progenitors):
- Through a complex process of both:
- Epithelial-mesenchymal transformation and more frequently, mesenchymal-epithelial transformation
- Through a complex process of both:
- May originate from mesenchymal stem cells (progenitors):
- The clinical presentation:
- Is typically a recently detected, extensive, firm lesion:
- Often appearing as an interval cancer following a previous mammogram which was interpreted as normal
- Is typically a recently detected, extensive, firm lesion:
- On clinical breast examination:
- The cancer does not have a distinct tumor mass or focal skin retraction seen in other cancers:
- But rather an indistinct “thickening” and eventually a shrinkage of the breast.
- The cancer does not have a distinct tumor mass or focal skin retraction seen in other cancers:
- In order to make the diagnosis before the development of a palpable mass and a decrease in size of the breast:
- The radiologist and breast surgeon must have a high level of suspicion and a thorough knowledge of the underlying pathophysiology
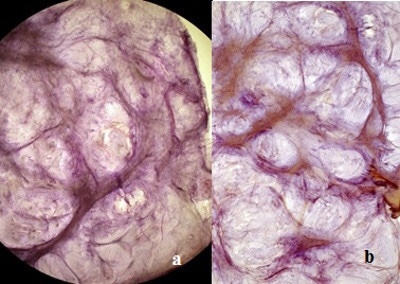
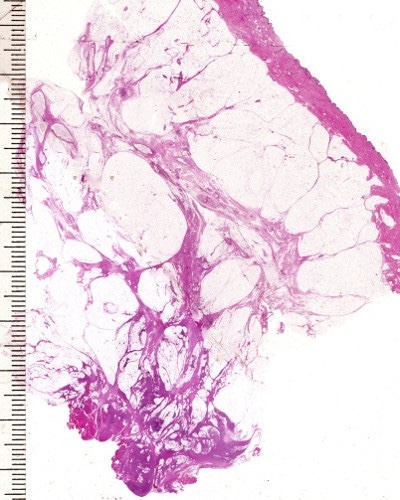
- The subgross (3D) histopathology images show how growth of the mesenchymal tissue:
- Distorts the normal, harmonious connective tissue framework:
- By causing nonuniform thickening of the fine sheets of connective tissue (Images):
- Distorts the normal, harmonious connective tissue framework:
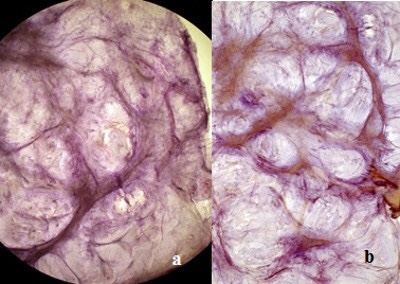
- The predominance of mesenchyme in the diffusely infiltrating breast malignancy:
- Allows it to be imaged with greater sensitivity by ultrasound than by mammography:
-
-
- The thin sheets or veils of tissue reflect the ultrasound waves:
- But are relatively easily penetrated by x-rays
- The thin sheets or veils of tissue reflect the ultrasound waves:
-
-
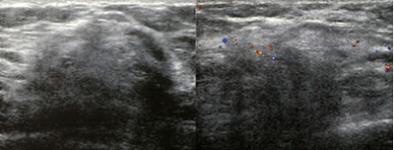
- The structural / architectural distortion:
-
- While difficult to detect mammographically:
- Is readily detectable on 2-mm thick coronal sections of automated breast ultrasound (Image)
- While difficult to detect mammographically:

- The 2-mm thick multi-slice series demonstrate the extensive architectural distortion, corresponding to the 3D histology:
- The hypoechoic changes can also usually be seen on hand held ultrasound, Image:
- The growth pattern and cell type of diffusely invasive breast cancer:
- Is very similar to that of diffuse gastric carcinoma (linitis plastica), and both of these diseases can be associated with:
- A deleterious mutation in the CDH1 gene:
- Which is located on chromosome 16q22 and codes for e-cadherin protein (Image):
- A deleterious mutation in the CDH1 gene:
- Is very similar to that of diffuse gastric carcinoma (linitis plastica), and both of these diseases can be associated with:

- CDH1 was initially known as a susceptibility gene for diffuse gastric cancer (linitis plastica)
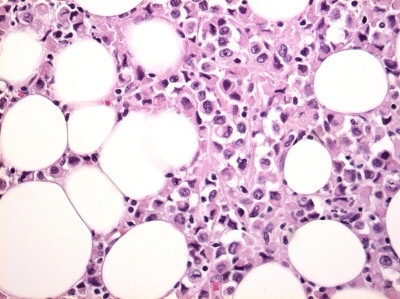
- The histopathologic characteristics of diffuse gastric cancer:
- Show similarities with e-cadherin negative:
- Diffusely infiltrating breast cancer (infiltrating “lobular” carcinoma)
- The neoplastic cells permeate the mucosa and wall as scattered individual signet-ring cells or small clusters of cells in an infiltrative growth pattern
- Show similarities with e-cadherin negative:
- Since there are no TDLUs in the stomach:
- If the similar cells in both conditions associated with CDH1 have a common origin, it could not be a TDLU:
-
- Raising the possibility that they could result from mesenchymal cell transformation in both organs

👉Rodrigo Arrangoiz MS, MD, FACS, FSSO cirujano oncology y cirujano de mamá de en Mount Sinai Medical Center:
-
Es experto en el manejo del cáncer de mama

👉Es miembro de la American Society of Breast Surgeons:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


