- It is clear that patients with pathologically negative sentinel lymph nodes:
- Do not require completion ALND:
- But the management of patients with ITCs and micrometastatic disease in sentinel lymph nodes:
- Has extensively been debated
- But the management of patients with ITCs and micrometastatic disease in sentinel lymph nodes:
- Do not require completion ALND:
- Micrometastatic disease is defined as:
- Tumor deposits spanning:
- 0.2 mm to 2.0 mm:
- Within lymph nodes
- 0.2 mm to 2.0 mm:
- Tumor deposits spanning:
- ITCs are:
- Groupings of cells not greater than 0.2 mm or 200 cells:
- In a single lymph node cross section
- Groupings of cells not greater than 0.2 mm or 200 cells:
- According to the American Joint Committee on Cancer (AJCC) staging guidelines:
- Patients with ITCs are N0(i+)
- Patients with micrometastases in one to three axillary lymph nodes are N1mi
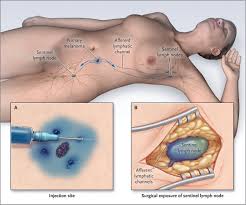
- ACOSOG Z0010:
- Is one of the largest trials to prospectively evaluate the significance of small metastases in sentinel nodes
- Hematoxylin and eosin (H&E) tumor-free sentinel nodes:
- From patients with early breast cancer were evaluated in a central laboratory with:
- Immunohistochemistry (IHC)
- From patients with early breast cancer were evaluated in a central laboratory with:
- Micrometastatic or ITC disease:
- Was found in 11% of 3,326 sentinel lymph nodes
- With a median follow-up of 6.3 years:
- Occult sentinel lymph node metastases:
- Were not associated with differences in overall survival, disease-free survival, or recurrence:
- When compared with patients with IHC-negative lymph nodes
- Were not associated with differences in overall survival, disease-free survival, or recurrence:
- Occult sentinel lymph node metastases:
- A subset analysis of NSABP-32:
- Looked retrospectively at patients with occult metastatic disease:
- Including patients with micrometastatic or isolated tumor cells
- In patients who were sentinel node negative:
- 16% had occult metastases detected on further evaluation:
- 11% of occult metastases were isolated tumor-cell clusters, 4% were micrometastases, and less than 1% of patients had macrometastatic deposits seen on additional sectioning of the lymph node
- 16% had occult metastases detected on further evaluation:
- Log-rank tests indicated that patients with occult metastasis:
- Had worse overall survival (95% versus 96%), disease-free survival (87% versus 89%), and distant disease-free interval (90% versus 93%):
- When compared with patients without occult metastases
- Although statistically significant:
- These differences were not felt to be clinically relevant
- Had worse overall survival (95% versus 96%), disease-free survival (87% versus 89%), and distant disease-free interval (90% versus 93%):
- There was no improvement in overall or disease-free survival:
- When patients with occult metastasis underwent completion ALND
- Looked retrospectively at patients with occult metastatic disease:
#Arrangoiz #CancerSurgeon #BreastSurgeon #SurgicalOncologist #BreastExpert #BreastCancer #SLNM #SLNB #SentinelLymphNodeBiopsy #Surgeon #Teacher #MSMC #MountSinaiMedicalCenter #Miami #Mexico