My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
The lifetime risk of breast cancer for women with deleterious BRCA1 mutations is 40% to 80% and the risk is slightly lower for BRCA2 carriers.
Mastectomy is the most effective prophylactic surgical measure to prevent the development of breast cancer; it reduces a woman’s risk by approximately 90% because a small amount of breast tissue must remain on the skin flaps for viability.
Women with BRCA1 mutations also have an approximate 40% lifetime risk of developing ovarian cancer, and bilateral salpingo-oophorectomy is recommended for prophylaxis.
Removal of the fallopian tubes with the ovaries is recommended because the risk of fallopian tube cancers is slightly higher for mutation carriers.
Oophorectomy does not completely eliminate the risk of abdominal epithelial cancers that behave like and are nearly indistinguishable from ovarian cancer.
In BRCA mutation carriers, there is a greater risk of primary peritoneal carcinoma, which behaves and is treated like ovarian cancer.
The patient should have bilaterial salpingo-oophorectomy once she has had her children or by age 40 years if she has not had children.
It is not recommended to wait until age 60 years to have this procedure, as ovarian cancer usually develops at a younger age.
The National Comprehensive Cancer Network (NCCN) recommendations for use of breast MRI for women with hereditary breast and ovarian cancer syndrome are annual screening with mammography, and breast MRI at alternating 6-month intervals.
MRI is not a substitute for mammography, however, as the modalities are complementary in BRCA-positive mutation carriers.
References:
Bradbury AR, Dignam JJ, Ibe CN, et al. How often do BRCA mutation carriers tell their young children of the family’s risk for cancer? A study of parental disclosure of BRCA mutations to minors and young adults. J Clin Oncol. 2007;25:3705-3711.
Hartmann LC, Schaid DJ, Woods JE, et al. Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer. N Engl J Med. 1999;340:77-84.
Hemel D, Domcheck SM. Breast cancer predisposition syndromes. Hematol Oncol Clin North Am. 2010;24:799-814.
Kauff ND, Domchek SM, Friebel TM, et al. Risk-reducing salpingo-oophorectomy for the prevention of BRCA1- and BRCA2-associated breast and gynecologic cancer: a multicenter, prospective study. J Clin Oncol. 2008;26:1331-1337.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology Genetic/Familial High-Risk Assessment: Breast and Ovarian. Available at http://www.nccn.org.
Patients that are Her2 / Neu-positive disease and a positive lymph node will need systemic chemotherapy in combination with Her2 / Neu-directed immunotherapy.
Neoadjuvant treatment is preferred, as this can downstage the disease, making her a candidate for lumpectomy and targeted axillary node dissection rather than conventional axillary node dissection.
The patient will need systemic chemotherapy in the form of docetaxel /carboplatin or adriamycin / cyclophosphamide in addition to Her2-directed therapies.
21-gene assay is used to predict benefit from systemic chemotherapy in women who have hormone receptor positive, Her2/neu-negative breast cancer.
References
National Comprehensive Cancer Network (NCCN) Guidelines 2017 – Breast Cancer Kuehn T, Bauerfeind I, Fehm T, Fleige B, Hausschild M, Helms G, Lebeau A, Liedtke C, von Minckwitz G, Nekljudova V, Schmatloch S, Schrenk P, Staebler A, Untch M. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): a prospective, multicentre cohort study. Lancet Oncol. 2013 Jun;14(7):609-18.
👉The primary application of ThyroSeq is to provide accurate cancer diagnosis in thyroid nodules with indeterminate FNA cytology
👉Indeterminate FNA cytology encompasses diagnostic categories III, IV, and V of the Bethesda System for Reporting Thyroid Cytopathology
👉Uncertain and variable risk of cancer in these nodules hampers clinical management of these patients
👉ThyroSeq stratifies thyroid nodules with indeterminate cytology into those that are most likely benign and can frequently be followed by observation and those that have a high probability of being cancer or pre-cancer, which in most cases need surgical management
Largest prospective double-blind multicenter study of any commercially available molecular test
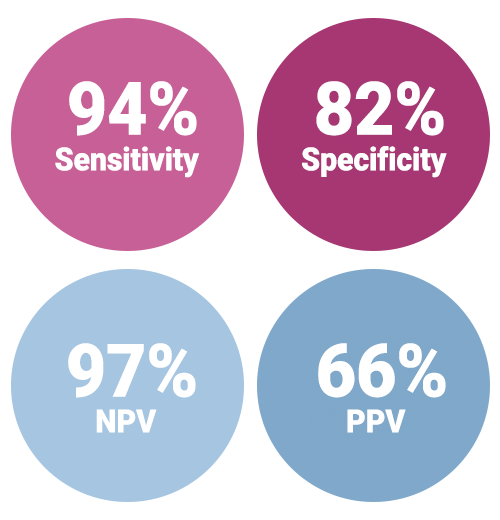
Highest NPV (97%) and PPV (66%) among well validated tests
Highest reduction in diagnostic surgery:
Allowing avoidance of surgery for up to 61% of all Bethesda III / IV nodules
82% of indeterminate nodules with benign pathology
Reliable detection of all types of thyroid tumors including Hurthle cell cancer
Reports probability of cancer and predicted risk of cancer recurrence:
Empowering individualized patient management
Test performance in Bethesda III and IV thyroid nodules
👉Clinical validation of ThyroSeq v3 performed in the recently completed prospective double-blind multicenter international study (ClinicalTrials.gov identifier NCT02352766)
👉Patients were enrolled in the study at 10 medical centers, nine located in the U.S. and one in Singapore
👉Totally, 782 patients with one or more thyroid nodules sampled by FNA ( 1013 samples ) were enrolled
👉Of those, 257 FNA samples from 234 patients had Bethesda III to V cytology, underwent surgery, and had FNA samples sufficient for molecular analysis
👉These 257 FNA samples comprised a final validation set that determined ThyroSeq v3 performance. The study had no post-unblinding sample exclusion
👉Performance of ThyroSeq v3 in the prospective double-blind multicenter study was recently published in JAMA Oncology. (Steward, DL et al. JAMA Oncol. 2018.)
👉In this multicenter study, clinical performance of ThyroSeq v3 was validated in all main types of thyroid cancer, including Hurthle cell (oncocytic) cancer
👉In fact, the study included 10 Hurthle cell carcinomas, 34 Hurthle cell adenomas, and 5 hyperplastic nodules with Hurthle cell predominance
👉The performance of ThyroSeq v3 allowed to detect all Hurthle cell carcinomas (sensitivity, 100%; 95%CI:69.2-100%), with all 5 hyperplastic nodules with Hurthle cell predominance classified as Negative, and overall test specificity of 66.7% (95%CI: 49.8-80.9%).
👉In the study, the majority of nodules with false-positive test results were clonal neoplasms and not hyperplastic nodules
👉There were five missed cancers that were all intrathyroidal and low stage
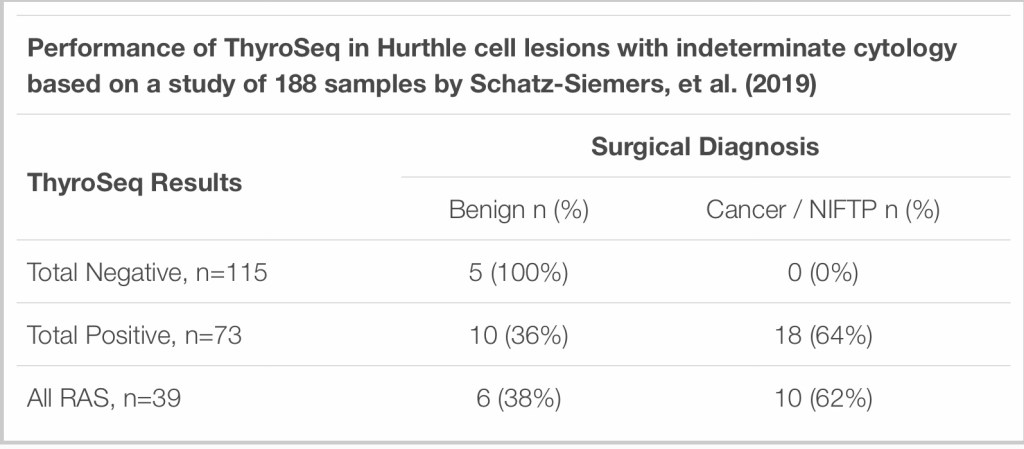
👉Additionally, ThyroSeq performance in Hurthle cell lesions was assessed in an independent study from NYU that included 188 indeterminate Hurthle cell predominant thyroid FNAs that had ThyroSeq v2/v3 results
👉Surgical follow up was available for 33 cases:
The study found that the majority of cases (61%) were negative by ThyroSeq, meaning ThyroSeq had a 61% negative call rate in Hurthle cell lesions in this study
Five of the ThyroSeq-negative cases went for surgery and all were benign on histology:
Which means ThyroSeq had 100% NPV for Hurthle cell lesions that went to surgery in this study
28 samples were ThyroSeq-positive and went for surgery with 18 diagnosed as cancer or NIFTP on final histology:
Meaning ThyroSeq had a 64% PPV for cancer / NIFTP in Hurthle cell nodules in this study.
👉Detection of other lesions:
In addition to the high accuracy in detecting all main types of thyroid cancer in nodules with indeterminate cytology:
ThyroSeq is able to reliably identify rare types of thyroid cancer (medullary thyroid carcinoma) and non-thyroid nodules such as parathyroid nodules
In the clinical validation study, ThyroSeq correctly identified one medullary thyroid carcinoma and one metastatic renal carcinoma
Also, ThyroSeq GC correctly detected all 13 parathyroid lesions, all 15 medullary thyroid carcinomas, and all 20 nonthyroidal samples in the analytical validation study of the test
Detection of parathyroid lesions by ThyroSeq was validated in an independent study
👉How diagnostic performance of ThyroSeq compares with other tests – ThyroSeq v3 GC compared to Afirma GSC
👉According to the ThyroSeq clinical validation study supplemental table above, reported in JAMA Oncology, ThyroSeq GC has a benign call rate of 61%, as compared to the Afirma GSC rate of 54%, which indicates that ThyroSeq allows more patients to safely avoid diagnostic surgeries
👉Additionally, ThyroSeq GC has a higher negative call rate for histologically benign nodules with indeterminate cytology (82%) than Afirma GSC (68%). This means that patients with nodules that have indeterminate cytology but are histologically benign would avoid diagnostic surgery with ThyroSeq GC more often than with Afirma GSC.
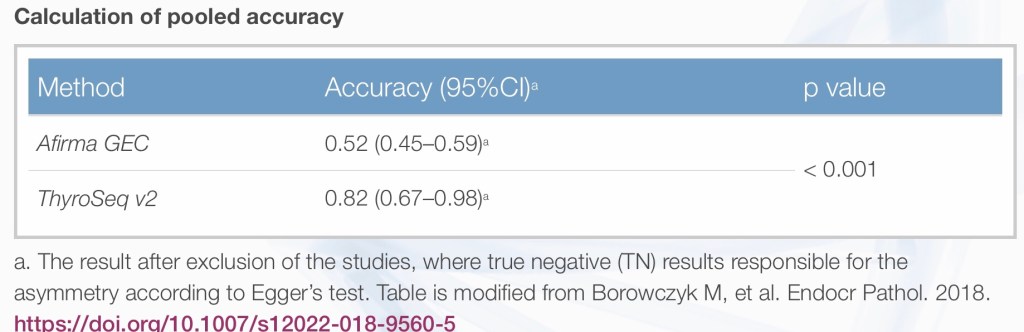
👉ThyroSeq v2 compared to other tests
In a review reported in JAMA Otolaryngology–Head & Neck Surgery, the performance of ThyroSeq v2 was compared with two other available tests based on the primary validation studies, showing that out of all tests:
ThyroSeq had best PPV and NPV in both Bethesda III and IV cytology nodules
Which allowed more patients to avoid diagnostic surgery
An independent review study that analyzed data from studies of ThyroSeq v2 and Afirma GEC found that ThyroSeq had “significantly higher specificity and accuracy with an acceptable sensitivity so that it has the potential for use as an all-round test of malignancy of thyroid nodules.”
The superiority of ThyroSeq v2 is demonstrated in the study data below.
The hallmarks of inflammatory breast cancer include warmth, edema, and erythema encompassing more than half of her breast.
Although inflammatory breast cancer is largely a clinical diagnosis, a skin punch biopsy revealing dermal lymphatic invasion confirms the diagnosis even in the absence of any obvious breast mass.
The standard treatment at this time involves neoadjuvant chemotherapy, modified radical mastectomy followed by postmastectomy radiation therapy.
Additional adjuvant systemic therapy is also administered based on the characteristics of the cancer (hormone receptor positive disease will receive hormonal therapy and HER2(+) disease anti-HER2-based therapy.
References
Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, 20th ed. Ch. 34: Diseases of the Breast.
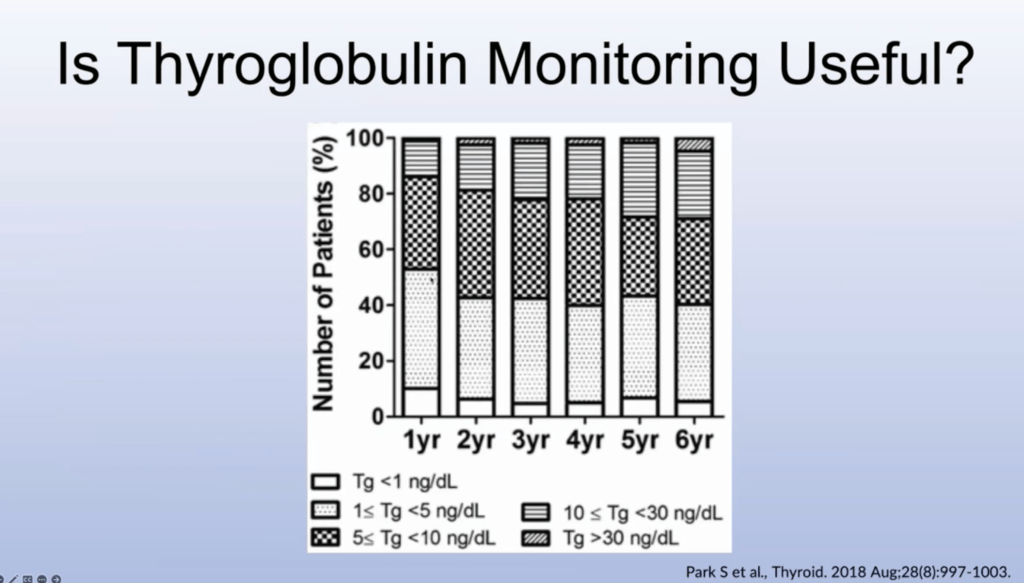
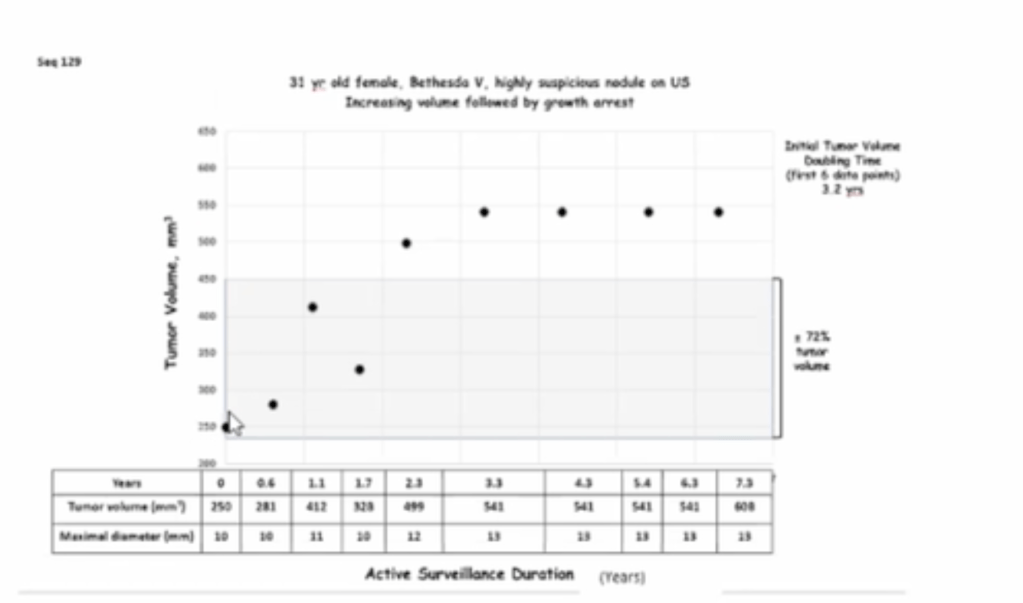
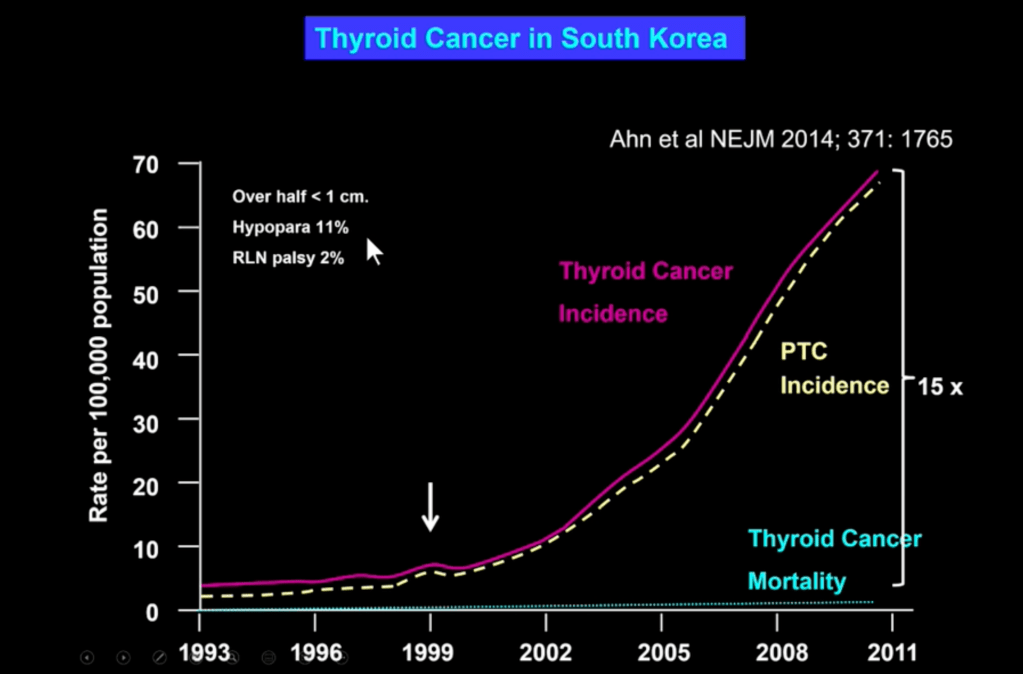
In 1999 in South Korea Screening Ultrasound Were Offered at a very affordable price. The incidence went up 15 fold making thyroid cancer the most common malignancy in women but mortality remained stable. This increase was PTC smaller than 1 cm