👉The primary application of ThyroSeq is to provide accurate cancer diagnosis in thyroid nodules with indeterminate FNA cytology
👉Indeterminate FNA cytology encompasses diagnostic categories III, IV, and V of the Bethesda System for Reporting Thyroid Cytopathology
👉Uncertain and variable risk of cancer in these nodules hampers clinical management of these patients
👉ThyroSeq stratifies thyroid nodules with indeterminate cytology into those that are most likely benign and can frequently be followed by observation and those that have a high probability of being cancer or pre-cancer, which in most cases need surgical management

👉ThyroSeq Clinical Validation Study Overview:
- Reported in the premiere medical journal – JAMA Oncology (Steward, DL et al. JAMA Oncol. 2018.)
- Largest prospective double-blind multicenter study of any commercially available molecular test
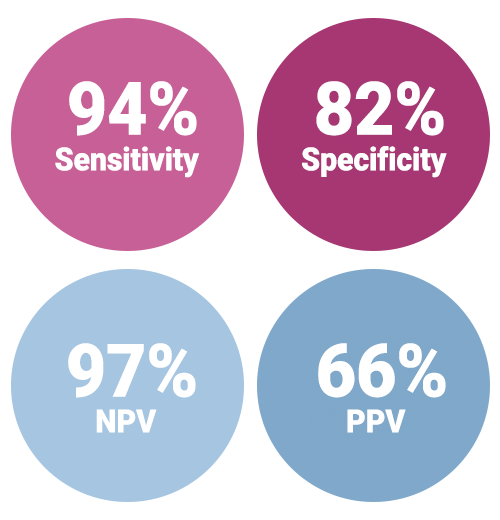
- Highest NPV (97%) and PPV (66%) among well validated tests
- Highest reduction in diagnostic surgery:
- Allowing avoidance of surgery for up to 61% of all Bethesda III / IV nodules
- 82% of indeterminate nodules with benign pathology
- Reliable detection of all types of thyroid tumors including Hurthle cell cancer
- Reports probability of cancer and predicted risk of cancer recurrence:
- Empowering individualized patient management
👉Clinical validation of ThyroSeq v3 performed in the recently completed prospective double-blind multicenter international study (ClinicalTrials.gov identifier NCT02352766)
👉Patients were enrolled in the study at 10 medical centers, nine located in the U.S. and one in Singapore
👉Totally, 782 patients with one or more thyroid nodules sampled by FNA ( 1013 samples ) were enrolled
👉Of those, 257 FNA samples from 234 patients had Bethesda III to V cytology, underwent surgery, and had FNA samples sufficient for molecular analysis
👉These 257 FNA samples comprised a final validation set that determined ThyroSeq v3 performance. The study had no post-unblinding sample exclusion

👉Performance of ThyroSeq v3 in the prospective double-blind multicenter study was recently published in JAMA Oncology. (Steward, DL et al. JAMA Oncol. 2018.)
👉In this multicenter study, clinical performance of ThyroSeq v3 was validated in all main types of thyroid cancer, including Hurthle cell (oncocytic) cancer
👉In fact, the study included 10 Hurthle cell carcinomas, 34 Hurthle cell adenomas, and 5 hyperplastic nodules with Hurthle cell predominance
👉The performance of ThyroSeq v3 allowed to detect all Hurthle cell carcinomas (sensitivity, 100%; 95%CI:69.2-100%), with all 5 hyperplastic nodules with Hurthle cell predominance classified as Negative, and overall test specificity of 66.7% (95%CI: 49.8-80.9%).
👉In the study, the majority of nodules with false-positive test results were clonal neoplasms and not hyperplastic nodules
👉There were five missed cancers that were all intrathyroidal and low stage
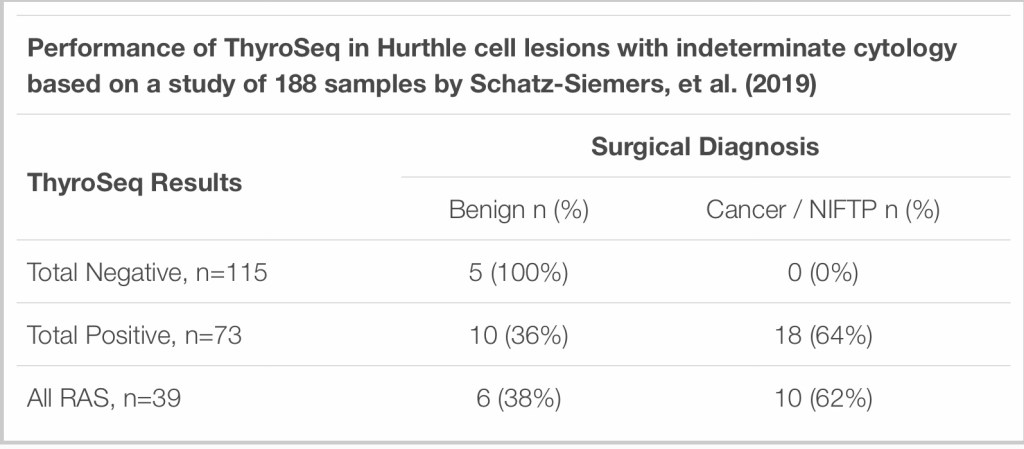
👉Additionally, ThyroSeq performance in Hurthle cell lesions was assessed in an independent study from NYU that included 188 indeterminate Hurthle cell predominant thyroid FNAs that had ThyroSeq v2/v3 results
👉Surgical follow up was available for 33 cases:
- The study found that the majority of cases (61%) were negative by ThyroSeq, meaning ThyroSeq had a 61% negative call rate in Hurthle cell lesions in this study
- Five of the ThyroSeq-negative cases went for surgery and all were benign on histology:
- Which means ThyroSeq had 100% NPV for Hurthle cell lesions that went to surgery in this study
- 28 samples were ThyroSeq-positive and went for surgery with 18 diagnosed as cancer or NIFTP on final histology:
- Meaning ThyroSeq had a 64% PPV for cancer / NIFTP in Hurthle cell nodules in this study.
👉Detection of other lesions:
- In addition to the high accuracy in detecting all main types of thyroid cancer in nodules with indeterminate cytology:
- ThyroSeq is able to reliably identify rare types of thyroid cancer (medullary thyroid carcinoma) and non-thyroid nodules such as parathyroid nodules
- In the clinical validation study, ThyroSeq correctly identified one medullary thyroid carcinoma and one metastatic renal carcinoma
- Also, ThyroSeq GC correctly detected all 13 parathyroid lesions, all 15 medullary thyroid carcinomas, and all 20 nonthyroidal samples in the analytical validation study of the test
- Detection of parathyroid lesions by ThyroSeq was validated in an independent study
👉How diagnostic performance of ThyroSeq compares with other tests – ThyroSeq v3 GC compared to Afirma GSC

👉According to the ThyroSeq clinical validation study supplemental table above, reported in JAMA Oncology, ThyroSeq GC has a benign call rate of 61%, as compared to the Afirma GSC rate of 54%, which indicates that ThyroSeq allows more patients to safely avoid diagnostic surgeries
👉Additionally, ThyroSeq GC has a higher negative call rate for histologically benign nodules with indeterminate cytology (82%) than Afirma GSC (68%). This means that patients with nodules that have indeterminate cytology but are histologically benign would avoid diagnostic surgery with ThyroSeq GC more often than with Afirma GSC.
👉ThyroSeq v2 compared to other tests
- In a review reported in JAMA Otolaryngology–Head & Neck Surgery, the performance of ThyroSeq v2 was compared with two other available tests based on the primary validation studies, showing that out of all tests:
- ThyroSeq had best PPV and NPV in both Bethesda III and IV cytology nodules
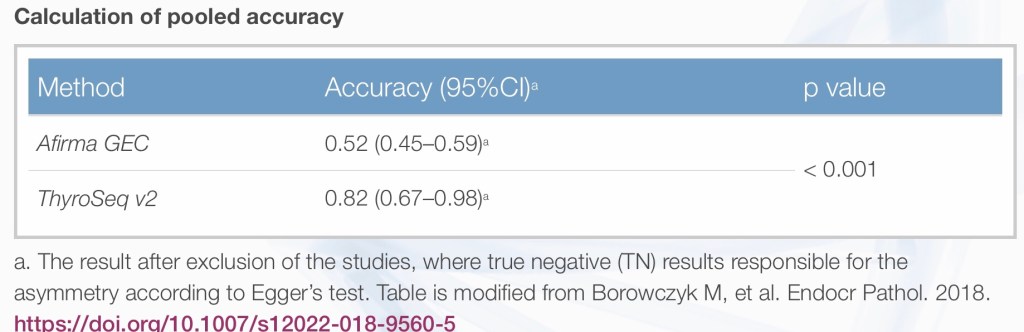
- According to an independent study performed at UCLA, ThyroSeq v2 specificity was superior to that of Afirma GEC:
- Which allowed more patients to avoid diagnostic surgery
- An independent review study that analyzed data from studies of ThyroSeq v2 and Afirma GEC found that ThyroSeq had “significantly higher specificity and accuracy with an acceptable sensitivity so that it has the potential for use as an all-round test of malignancy of thyroid nodules.”
- The superiority of ThyroSeq v2 is demonstrated in the study data below.
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #CancerSurgeon #HeadandNeckSurgeon #ThyroidNodules #Thyroseq

