My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
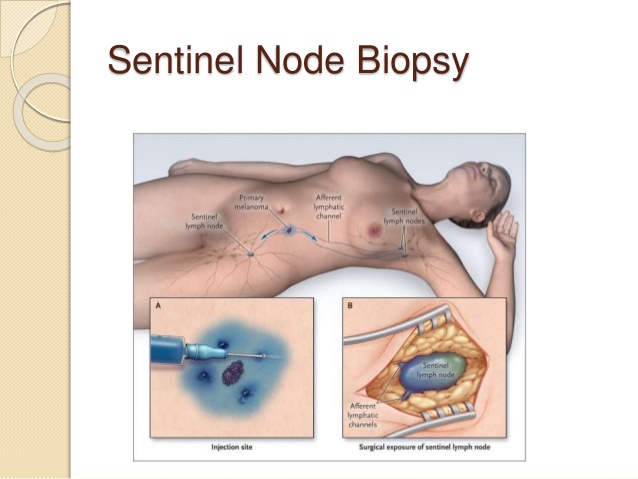
The overall significant complication rate from sentinel lymph node dissection reported from the ACOSOG Z0010 trial:
Was low:
With 32% of patients reporting at least one surgical side effect and less than 1% of patients requiring hospitalization
The most common surgical side effect was:
Axillary paresthesia:
Affecting 307 (8.6%) of 3,573 patients
Allergic reaction:
Was reported in less than 1%:
Related to the administration of lymphazurin blue dye
Lymphedema in 7%
Brachial plexus injury in less than 1% of patients
Only one anaphylactic reaction to blue dye was reported
References
Hunt KK, Ballman KV, McCall LM, Boughey JC, Mittendorf EA, Cox CE, et al. Factors associated with local-regional recurrence after a negative sentinel node dissection: results of the ACOSOG Z0010 trial. Ann Surg. 2012;256(3):428-436.
Boughey JC, Hunt KK. The ACOSOG experience. In: Kuerer HM, ed. Kuerer’s Breast Surgical Oncology. New York, NY: McGraw-Hill Companies; 2010:517-530.
Phase III Total Mastectomy / Axillary Dissection vs. Segmental Mastectomy / Axillary Dissection with or without Radiotherapy for Potentially Curable Breast Carcinoma:
Compared total mastectomy with lumpectomy alone and lumpectomy with irradiation in patients with tumors 4 cm or less in greatest diameter
All patients had an axillary lymph node dissection (ALND)
This trial, along with 5 other randomized prospective trials:
Was instrumental in establishing lumpectomy plus radiation therapy as the preferred treatment for women with early stage, operable breast cancer, as compared to mastectomy
After 20 years of follow-up:
There were no observed differences in:
Overall survival, or distant disease-free survival:
Between the total mastectomy group and the lumpectomy groups, with or without radiation:
The hazard ratio (HR) for death with lumpectomy alone was 1.05 (95% confidence interval [CI] 0.90–1.23; P=0.51)
The HR for death with lumpectomy plus radiation was 0.97 (95% CI, 0.83–1.14; P=0.74):
Which were comparable to total mastectomy
NSABP B-04:
Enrolled clinically node-negative patients and randomized them to radical mastectomy (RM), total mastectomy (TM) plus radiation, or TM alone
NSABP B-17:
Compared lumpectomy alone to lumpectomy plus breast radiation:
In patients with localized ductal carcinoma in situ (DCIS)
NSABP B-32:
Assigned clinically node-negative patients to either sentinel lymph node (SLN) resection plus ALND (group 1) or to SLN resection alone with ALND only if the SLNs were positive (group 2)
NSABP protocol B-43:
Aims to evaluate the effect of trastuzumab on local recurrence in patients with HER2-positive DCIS treated with lumpectomy and whole-breast irradiation
References:
Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347(16):1233-1241.
Fisher B, Montague E, Redmond C, Barton B, Borland D, Fisher ER, et al. Comparison of radical mastectomy with alternative treatments for primary breast cancer: a first report of results from a prospective randomized clinical trial. Cancer. 1977;39(6 Suppl):2827-2839.
Mamounas EP, Wickerham DL, Fisher B, Geyer CE, Julian TB, Wolmark N. The NSABP experience. In: Kuerer HM, ed. Kuerer’s Breast Surgical Oncology. New York, NY: McGraw-Hill Companies; 2010:475-508.
Fisher B, Dignam J, Wolmark N, Mamounas E, Constantino J, Poller W, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. JClin Oncol. 1998;16(2):441-452.
Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, Constantino JP, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 Randomized Phase 3 Trial. Lancet Oncol. 2010;11(10):927-933.
Siziopilou KP, Anderson SJ, Cobleigh MA, Julian TB, Arthur DW, Zheng P, et al. Preliminary results of centralized HER2 testing in ductal carcinoma in situ (DCIS): NSABP B-43. Breast Cancer Res Treat. 2013;142(2):415-421.
The 21-gene recurrence-score assay (e.g., Oncotype DX, Genomic Health):
Is one of several commercially available gene-expression assays:
That provide prognostic information:
In hormone-receptor-positive breast cancer
The assay originally set cut points for:
Low risk at a recurrence score less than 18
Intermediate risk at 18 to 30
High risk at greater than 30
It is predictive of chemotherapy benefit:
When the recurrence score (RS) is high (greater than 26) and
It is prognostic for very low rates of distant recurrence:
2% at 10 years:
When the RS is low (less than 10)
The TAILORx prospective randomized clinical trial:
Was completed to determine whether chemotherapy is beneficial for women with an intermediate RS of 11 to 25:
The cutoffs for this trial were adjusted to ensure all patients in the intermediate range who may benefit were included
At 9 years of follow-up:
The endocrine therapy only and the chemo-endocrine therapy group had similar rates of invasive disease-free survival:
83.3% vs. 84.3% respectively
The endocrine therapy alone was noninferior to chemoendocrine therapy:
For all patients in the intermediate RS study group (RS 11 to 25)
The two groups also had similar outcomes in freedom from disease recurrence at a distant or locoregional sites:
However, the chemotherapy benefit for invasive disease-free survival varied with the combination of recurrence score and age (P=0.004):
With some benefit of chemotherapy found in women 50 years old or younger with an RS of 16 to 25:
In women less than 50 receiving chemotherapy:
Demonstrated a lower rate of distant recurrence than endocrine therapy if RS was:
16 to 20 (percentage-point difference, 0.8 at 5 years and 1.6 at 9 years) or 21 to 25 (percentage-point difference, 3.2 at 5 years and 6.5 at 9 years):
Overall survival however remained similar
For this reason, researchers conclude that the 21-gene assay can identify women with ER+ early-stage breast cancer:
Who may be spared chemotherapy if they are over 50 years old with an RS of 25 or lower:
As well as women 50 years or younger with RS of 15 or lower
References:
Sparano JA, Gray RJ, Makower DF, Pritchard K, Albain KS, Hayes DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med. 2018;379(2):111-121
Management of the nodal basins in a patient with drainage to both an epitrochlear and axillary or a popliteal and inguinal nodal pattern:
Warrants SLN biopsy of both basins and attention to each basin based on the SLN status of that respective basin
It is not possible, based on lymphoscintigraphy:
To determine whether the proximal lymphatic basins drain the primary tumor site through lymphatic channels that are separate from those that drain to the distal nodal basin
If found to have a positive sentinel lymph node:
Current management of the regional lymph node basin(s):
Have shifted towards observation by ultrasound as compared to completion lymph node dissection:
This shift in treatment paradigm was influenced by two randomized control trials:
MSLT II and DeCOG-SLT:
Both of which demonstrated no improved in survival in sentinel lymph node positive patients who underwent immediate completion lymph node dissection as compared to observation
Additionally, referral for adjuvant immunotherapy or targeted therapy:
Should be considered as recent evidence has demonstrated improvement in disease free survival:
Among resectable stage III melanoma patients that went on to receive adjuvant therapy
If unable to undergo close observation:
The appropriate next step is completion lymphadenectomy of all involved nodal basins:
Complete axillary dissection including all lymph nodes in levels 1, 2, and 3 along with the nodes superior to the axillary vein and superficial to the axillary artery and brachial plexus along with all of the nodal tissue along the subscapular musculature is the standard of care for patients with melanoma
Unlike the situation with breast cancer, adjuvant radiation and chemotherapy are not uniformly used and does is not a substitute for appropriate surgical therapy
References:
Bilimoria KY, Balch CM, Bentrem DJ, et al. Complete lymph node dissection for sentinel node-positive melanoma: assessment of practice patterns in the United States. Ann Surg Oncol. 2008;15:1566-1576.
Gershenwald JE, Andtbacka R, Prieto V, et al. Microscopic tumor burden in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma. J ClinOncol. 2008;26:4296-4303.
Pollock RE, Curley SA, Ross MI, et al, eds. Advanced Therapy in Surgical Oncology. Hamilton, Ontario, Canada: BC Decker; 2008.
Several trials have evaluated different approaches to improve outcomes beyond those achieved with one year of trastuzumab:
Five major studies include:
HERA trial:
Extending the duration of trastuzumab to 2 years
ALTTO trial:
Administration of lapatinib, a tyrosine kinase inhibitor, to trastuzumab
BETH trial (NSABP-B44):
Addition of bevacizumab, an anti-angiogenic agent, to trastuzumab
ExteNET trial:
Subsequent addition of neratinib, a tyrosine-kinase inhibitor, for 1 year
APHINITY trial (BIG 4-11):
Addition of pertuzumab to transtuzumab, for 1 year
The ExteNET and APHINITY:
Showed benefit with the additional therapy
HERceptin Adjuvant (HERA) trial:
An international, multicenter, phase 3 randomized trial:
Of 5,102 women with HER2-positive early breast cancer
After completing all primary therapy (including, surgery, chemotherapy, and radiotherapy as indicated):
Patients were randomly assigned to receive trastuzumab for 1 or 2 years, or to the observation group
Primary endpoint:
Was disease-free survival
Results reported that one year of adjuvant trastuzumab after chemotherapy for patients with HER2-positive early breast cancer:
Significantly improved long-term disease-free survival, compared with observation:
While two years of trastuzumab had no additional benefit
ALTTO (Adjuvant Lapatinib And / Or Trastuzumab Treatment Optimization) Study:
Was the first trial to test the hypothesis that dual anti-HER2 blockade could further improve survival outcomes of patients with HER2-positive early breast cancer compared with adjuvant trastuzumab
The study compared the efficacy of the addition of lapatinib to trastuzumab (sequentially after completion of 12 weeks of trastuzumab or concurrently with 52 weeks of trastuzumab) vs. trastuzumab alone for 1 year
Adjuvant treatment that included lapatinib:
Did not significantly improve survival compared with trastuzumab alone and added toxicity
NSABP B-44, also known as the BETH Study (Treatment of HER2 Positive Breast Cancer With Chemotherapy Plus Trastuzumab vs. Chemotherapy Plus Trastuzumab Plus Bevacizumab):
Was a phase 3 study evaluating the addition of bevacizumab, a vascular endothelial growth factor (VEGF-A) to trastuzumab
Patients were randomized to 1 of 4 treatment arms in 2 cohorts:
Cohort 1:
The nonanthracycline regimen TCH (docetaxel, carboplatin, and trastuzumab [Herceptin]) or TCH plus bevacizumab
Cohort 2:
Anthracycline-based therapy with T-FEC-H (docetaxel, fluorouracil, epirubicin, cyclophosphamide, plus trastuzumab) with or without bevacizumab
The study concluded that the addition of bevacizumab (Avastin) to adjuvant chemotherapy:
Did not improve invasive disease-free survival or overall survival in patients with high-risk HER2-positive breast cancer
BETH also demonstrated that the non–anthracycline-containing chemotherapy arm:
Was as effective in prolonging survival as the anthracycline-containing arm
Neratinib after trastuzumab-based adjuvant therapy in HER2-positive breast cancer (ExteNET) Trial:
Is a multicenter, randomized, phase 3 trial designed to investigate extended adjuvant therapy with neratinib
Patients received 1 year of extended adjuvant therapy with neratinib:
An irreversible pan-HER tyrosine kinase inhibitor:
Administered after chemotherapy and trastuzumab
The results showed that 1 year of neratinib:
Significantly improved 5-year invasive disease-free survival without increasing the risk of long-term toxicity
APHINITY trial (BIG 4-11):
A randomized comparison of chemotherapy (C) plus trastuzumab (T) plus placebo versus chemotherapy plus trastuzumab (T) plus pertuzumab (P) as adjuvant therapy in patients with HER2-positive early breast cancer
In previous neoadjuvant trials, pertuzumab significantly prolonged progression free and overall survival and increased pathologic complete response (pCR) rates when added to trastuzumab and chemotherapy
They investigated the role of pertuzumab when added to trastuzumab after surgery and chemotherapy in the adjuvant setting:
A small benefit in favor of the combination was observed, which was more pronounced in node-positive patients
References
Cameron D, Piccart-Gebhart MJ, Gelber RD, Proctor M, Goldhirsch A, de Azambuja E, et al. 11 years’ follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: final analysis of the HERceptin Adjuvant (HERA) trial. Lancet. 2017;389(10075):1195-1205.
Piccart-Gebhart M, Holmes E, Baselga J, de Azambuja E, Dueck AC, Viale G, et al. Adjuvant lapatinib and trastuzumab for early human epidermal growth factor receptor 2-positive breast cancer: results from the randomized phase III adjuvant lapatinib and/or trastuzumab treatment optimization trial. J Clin Oncol.2016;34(10):1034-1042.
Slamon DL, Swain SM, Buyse M, Martin M, Geyer CE. Primary results from BETH, a phase 3 controlled study of adjuvant chemotherapy and trastuzumab ± bevacizumab in patients with HER2-positive, node-positive, or high-risk node-negative breast cancer [Abstract]. Cancer Res. 2013;73(suppl 24): S1-03.
Martin M, Holmes FA, Ejlertsen B, Delaloge S, Moy B, Iwata H, et al. Neratinib after trastuzumab-based adjuvant therapy in HER2-positive breast cancer (ExteNET): 5-year analysis of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2017;18(12):1688-1700.
von Minckwitz G, Procter M, de Azambuja E, Zardavas D, Benyunes M, Viale G, et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer. N Engl J Med. 2017;377(2):122-131.
The treatment paradigm for melanoma patients with a positive SLN:
Has undergone a dramatic evolution in recent years
Historically, completion lymph node dissection (CLND) was considered the standard of care for patients found to have micrometastatic disease in the SLN:
However, two recent trials sought to investigate the efficacy of immediate CLND:
The DECOG-SLT and MSLT-II trials were multicenter randomized control trials:
That randomly assigned melanoma patients with sentinel-node metastasis to either immediate CLND versus observation by nodal ultrasound
In the DECOG-SLT trial:
477 patients were enrolled
At three years, the study reported no difference in distant metastasis-free survival:
77% versus 74.9%, HR 1.03; p=0.87 between the observation group and CLND group
At three years, the study reported no difference in overall survival:
81.7% versus 81.2%, HR 0.96; p=0.87 between the observation group and CLND group
Similarly, in the larger MSLT-II trial:
Where 1,755 patients were evaluated
The study found that immediate CLND did not improve melanoma-specific survival when compared to patients that underwent observation:
86% versus 86%; p=0.42
If, however, patients are unable or unwilling to undergo close surveillance:
Completion lymph node dissection can be considered
Which includes clearance of nodal tissue within the femoral triangle
These nodes are accessed via either an oblique incision below or a lazy incision crossing through the inguinal crease:
Flaps are made superiorly several centimeters above the inguinal ligament, laterally to the anterior superior iliac spine (ASIS) and proceeding along the lateral border of the sartorius to the apex of the femoral triangle, and medially along the adductor longus to the pubic symphisis:
All nodal tissue within these landmarks and around the femoral vessels is taken:
With effort to preserve the lateral femoral cutaneous nerve:
As it runs below the ASIS and superior to the sartorius
The saphenous vein may be sacrificed if gross nodal disease precludes safe dissection of nodal tissue circumferentially:
However, preservation can be performed with theoretical benefits in preventing lymphedema
Depending on the extent of tissue resection and the health of overlying skin, a sartorius transposition flap can be made to cover the femoral vessels
Several centers advocate intraoperative assessment by frozen section of Cloquet’s node:
The lowest iliac node located within the femoral canal:
To determine whether immediate or delayed deep (iliac/obturator) node dissection is warranted:
However, the clinical adaptation of this technique is variable:
Sole excision of Cloquet’s node without further superficial inguinal node dissection is not standard of care
References:
Al-Refaie WB, Ross MI. Inguinal lymphadenectomy for malignant melanoma. Operative Techniques in General Surgery, 2006. WB Saunders, Philadelphia, PA.
Faries MB, Thompson JF, Cochran AJ, et al: Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma. N Engl J Med 376:2211-2222, 2017
Leiter U, Stadler R, Mauch C, et al: Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG-SLT): a multicentre, randomised, phase 3 trial. Lancet Oncol 17:757-767, 2016
Essner R, Scheri R, Kavanagh M, et al. Surgical management of the groin lymph nodes in melanoma in the era of sentinel node dissection. Arch Surg. 2006;141:877-882.
Jacobs LK, Balch CM, Coit DG. Inguinofemoral iliac/obturator, and popliteal lymphadenectomy in patients with melanoma. In: Balch CM, Houghton AN, Sober AJ, Soong S-J (eds.) Cutaneous Melanoma. 5th ed. St. Louis: Quality Medical Publishing; 2009:457-470.
Tsao H, Atkins M, Sober AJ. Management of cutaneous melanoma. N Engl J Med. 2004;998-1012.
Begins with the documentation of limb measurements:
For both arms or legs:
Using either volume displacement or circumferential measurement:
All extremities must be measured at multiple points.
Increased physical activity:
Has proven to decrease lymphedema symptoms
Compression sleeve:
Should be 30 to 40 mm Hg of compression
There are several microsurgery techniques:
That have proven to improve lymphedema symptoms
References:
Gershenwald JE, Scolyer RA, Hess KR, et al. Melanoma Staging: Evidence-Based Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual. CA Cancer J Clin. 2017; 67(6): 472-492.
Wong SL, Balch CM, Hurley P, et al. Sentinel lymph node biopsy for melanoma: American Society of Clinical Oncology and Society of Surgical Oncology joint clinical practice guideline. J Clin Oncol. 2012; 30 (23): 2912-8.
Faries MB, Thompson JF, Cochran AJ, et al. Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma. N Engl J Med. 2017; 376(23): 2211-2222.
A multi-institution, prospective randomized trial from participating Cancer Care Ontario Centers:
Was performed from 1993 to 1996
The study sought to determine whether accelerated hypofractionated whole-breast irradiation (WBI) was as effective as conventional 5-week fractionation
Included in the study were women who received:
Breast-conserving surgery (BCS) for invasive breast cancer with clear surgical margins and negative axillary nodes
Participants were randomly assigned to receive WBI either at the standard dose of 50.0 Gy in 25 fractions over 35 days (control group), or at a dose of 42.5 Gy in 16 fractions over 22 days (hypofractionated-radiation group)
The control group included:
612 patients and the hypofractionation group had 622 patients
Results from this study indicated that the Canadian regimen was not inferior to the standard 5-week treatment regimen for women who received BCS for invasive breast cancer with clear surgical margins and negative axillary nodes
The risk of local recurrence at 10 years was:
6.7% in the control group and 6.2%in the hypofractionated group
Cosmesis at 10 years was found to be comparable between the two groups:
With good or excellent outcomes for 71.3% of women in the control group and 69.8% in the hypofractionated-radiation group
There was also no difference between the two groups in overall survival and no increase in cardiac-related deaths was seen in the hypofractionated group
References
1. Whelan TJ, Pignol J-P, Levine MN, Julian JA, MacKenzie R, Parpia S, et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med. 2010;362(6):513-520.
Breast cancer is a growing global health care issue in older women
The incidence of breast cancer has risen steadily in most European countries between 1990 and 2002:
In women aged 70 years or older
In several clinical trials, low-risk patients have been identified in whom the effect of postoperative whole-breast irradiation is modest:
Although these studies have been done mainly in younger patient populations:
However, in older patients, the biology of breast cancer might be less aggressive:
In view of the increased proportion of hormone receptor-positive tumors in this age group
Postoperative whole-breast radiotherapy remains the standard of care:
For most patients treated by breast-conserving surgery, irrespective of age and other risk factors:
However, little evidence exists for the role of postoperative radiotherapy in older patients after breast-conserving surgery and adjuvant endocrine treatment:
Because many trials, historically, excluded patients older than age 70 years
Extrapolation of the results of trials in younger patients to older patients might not be valid:
Particularly because of the competing risks of comorbidities in older patients
Data for the effect of age on local recurrence after breast-conserving surgery have been conflicting:
In some trials, ipsilateral breast tumor recurrence falls with increasing age or no effect is seen:
However, patients older than 65 years (and particularly those older than 75 years) were not well represented in any of these trials
Since tamoxifen with or without adjuvant radiotherapy reduces the risk of tumor recurrence:
The investigators of the PRIME II trial designed a randomized controlled trial in a group of older, low-risk, node-negative women with invasive breast cancer after breast-conserving surgery and adjuvant endocrine treatment to assess the effect omission of whole-breast irradiation has on local control
Methods:
Participants:
They performed a phase 3 randomized controlled trial at 76 specialist cancer centres and district or regional hospitals in four countries (the UK, Greece, Australia, and Serbia)
They recruited women aged 65 years or older with breast cancer who had undergone breast-conserving surgery and pathological axillary staging (ipsilateral four-node lower axillary node sample, sentinel node biopsy, or axillary node clearance)
Eligibility criteria were:
T1 to T2 (up to 3 cm, longest dimension); N0; M0; hormone receptor-positive (estrogen receptor, progesterone receptor, or both); clear excision margins (≥ 1 mm); no axillary involvement on histological examination (pN0); and receiving adjuvant hormone treatment (we permitted neoadjuvant hormonal treatment)
Staging investigations included full blood count, liver function tests, and chest radiography
They required re-excision margins to be 1 mm or greater, but we did not request the actual final measurement because this value can be difficult for the pathologist to estimate
All patients had to be fit for treatment and follow-up (as assessed by the participating centre) and able and willing to give informed consent
They did not request details of specific performance status nor formal documentation of comorbidities
Patients’ tumors could have grade 3 histological features or lymphovascular invasion, but not both
They excluded patients if they were younger than 65 years at the time pathological results were issued or if they had a history of previous in-situ or invasive breast cancer of either breast
We also excluded women with current or previous malignant disease within the past 5 years, other than non-melanomatous skin cancer or carcinoma in situ of the cervix
We did not record HER2 status in these patients because this marker was not routinely assessed at the start of the trial
The PRIME II study protocol received UK national ethics (MREC) approval on Sept 24, 2001
All patients gave written informed consent before randomization
Follow-up is ongoing and will end at the 10-year anniversary of the last randomized patient
Randomization and masking:
We randomly allocated patients to either whole-breast radiotherapy or no radiotherapy in a 1:1 ratio using a computerized randomization service
Randomization was by block permutation, stratified by center, with a block size of four
Once a patient had provided informed consent, a research nurse familiar with the trial contacted the central independent randomization service (Information Services Division Scotland, Edinburgh, UK) by telephone; a trial identifier was generated and treatment was assigned
The assignment was confirmed by a fax sent to both the registering center and the trial manager
They could not mask participants to the treatment being given
However, no evidence was present in the trial identifier to indicate to which treatment the patient had been allocated; therefore, during follow-up and data analysis, researchers were unaware of patients’ allocation unless they specifically looked for it
Procedures:
The total radiotherapy dose, number of fractions, and overall treatment time was administered according to local practice in every center:
However, we provided a guideline for dose fractionation of 40 to 50 Gy(2.66–2.00 Gy per fraction in 15 to 25 fractions) over 3 to 5 weeks at megavoltage irradiation to the breast
They permitted a breast boost with electrons of 10 to 15 Gy at appropriate energy or an iridium implant (eg, 20 Gy to 85% reference isodose)
Guidelines on radiotherapy included some form of immobilization, a planned target volume of the whole breast (margin of 1 cm), and all patients being simulated to establish the volume of lung irradiated (maximum lung thickness no greater than 3 cm)
They specified that the peripheral lymphatic system was not to be irradiated
They stated that a minimum of one transverse outline, taken at the central axis of the tangential fields, was to be taken
All fields were to be treated with megavoltage irradiation, with wedged fields so that dose homogeneity did not vary by more than 10%
They indicated that doses were to be prescribed to the reference point at or close to the center of the target volume (ICRU-50)
For the boost volume, they specified the tumor bed with lateral margins of 2 cm and a deep margin extending down to the underlying muscle
They indicated tamoxifen (20 mg daily for 5 years) as the standard adjuvant endocrine treatment, but we allowed other forms of adjuvant and neoadjuvant endocrine treatment
Follow-up was for 10 years and consisted of annual clinic visits, examination and mammography for at least 5 years, and, beyond this time, either a clinic visit or a phone call to the patients’ primary health care doctor to ascertain their health status, in addition to follow-up mammography
Outcomes:
The primary endpoint was ipsilateral breast tumor recurrence
Secondary endpoints were:
Regional recurrence, contralateral breast cancer, distant metastases, disease-free survival, and overall survival
They defined ipsilateral breast tumor recurrence as any cancer in the scar, the adjacent area in the same breast, or in a different quadrant of the same breast
They defined regional recurrence as disease in the ipsilateral axillary or supra- clavicular lymph nodes
The endpoints were not centrally assessed but based on local investigator review
Results:
Between April 16, 2003, and Dec 22, 2009, 1326 patients were randomly allocated to either:
No radiotherapy (n=668) or whole-breast radiotherapy (n=658)
Of these, 39 did not receive radiotherapy after randomization and five received radiotherapy when they had been randomly allocated to the no radiotherapy group
Another three patients did not begin endocrine treatment after randomization or stopped taking it shortly after starting
1263 patients were recruited from the UK, 22 were from Greece, 16 were from Australia, and 25 were from Serbia
Patients’ median age was 70 years (IQR 67–74)
Fewer than 10% of patients had tumors with poor estrogen receptor status
91 (16%) of 584 patients for whom radiotherapy treatment data were available received a tumor bed boost after whole-breast radiotherapy
At median follow-up of 5 years (IQR 3·84–6·05):
Actuarial ipsilateral breast tumor recurrence was 1.3% (95% C1 0·2–2·3) in women allocated whole-breast radiotherapy and 4.1% (2.4–5.7) in those assigned no radiotherapy (log-rank p=0·0002)
The hazard ratio for ipsilateral breast tumor recurrence in patients allocated to no radiotherapy was 5.19 (95% CI 1·99–13·52; p=0·0007; full data, not truncated at 5 years)
The absolute risk reduction in ipsilateral breast tumor recurrence at 5 years was 2.9% (95% CI 1·1–4·8)
The number needed to treat was calculated to be 31.8 (95% CI 27·4–55·0), which equates to an adjusted absolute risk reduction of 3.1% (95% CI 1·8–3·6) by the Altman and Andersen methodology
26 (4%) patients assigned to no radiotherapy and five (1%) women allocated to whole-breast radiotherapy had local recurrences
Of the 26 local recurrences in the no radiotherapy group:
18 women had a local recurrence only
Six had both local and regional recurrence
Two had a local recurrence with distant spread
In the radiotherapy group:
Four patients had local recurrence only
One had local and regional recurrence
They did a multivariate Cox proportional hazards analysis of local recurrence according to known risk factors for local recurrence, including:
Pathological tumor size, margin status, tumor grade, age, presence of lymphovascular invasion, estrogen receptor status, and use of radiotherapy
Progesterone receptor status was excluded from analyses because roughly 30% of data were missing in each treatment group
The only factor that predicted local recurrence was:
Omission of radiotherapy (hazard ratio 4·87, 95% CI 1·86–12·74; p=0·0013), although poor estrogen receptor status and grade 3 tumors were of borderline significance (p=0·06):
However, very few women had either of these factors (36 [3%] patients had grade 3 tumors and 120 [9%] had poor estrogen receptor status)
Overall survival at 5 years was identical in the two treatment groups (93.9%, 95% CI 91.8–96·0; p=0·34)
At 5 years, no differences between treatment groups were noted:
In regional recurrences, distant metastases, contralateral breast cancers, or new cancers
Breast cancer-free survival at 5 years was 94.5% (95% CI 92·5–96·5) in women allocated to no radiotherapy and 97.6% (96·2–99·0) in those assigned to whole-breast radiotherapy:
The difference was attributable mainly to ipsilateral breast tumor recurrence
Only 12 (13%) of 89 deaths recorded by the time of analysis were due to breast cancer, eight (16%) of 49 women assigned to no radiotherapy and four (10%) of 40 allocated to whole-breast radiotherapy
In a hypothesis-generating unplanned subgroup analysis of local recurrence by estrogen receptor score:
Local recurrence at 5 years for women in the rich estrogen receptor subgroup was lower than in the whole population:
For patients assigned no radiotherapy, 20 (3%) of 593 patients had a local recurrence compared with five (<1%) of 601 women allocated whole-breast radiotherapy:
5-year ipsilateral breast tumor recurrence was 3.3% [95% CI 1·7–4·8] and 1.2% [0·1–2·2], respectively; p=0·002
In women with poor estrogen receptor status, six (9%) of 65 women allocated no radiotherapy had local recurrence compared with none of 55 women allocated to whole-breast radiotherapy (ipsilateral breast tumor recurrence at 5 years was 10.3% [95% CI 2·5–18·2] and 0%, respectively; p=0·026); however, the number of patients in this analysis is small
Conclusion
Postoperative whole-breast radiotherapy achieved a significant but relatively small reduction in local breast recurrence at 5 years in a population of low-risk older patients with early breast cancer after breast-conserving surgery and adjuvant endocrine treatment
The only other trial in which omission of radiotherapy was investigated in a low-risk population was the CALGB 9343 trial,17,18 in which a similar 3% reduction in local recurrence at 5 years was noted with addition of radiotherapy
Our findings add to existing evidence of the safety of omitting radiotherapy after breast-conserving surgery in older patients, in whom the benefits of adjuvant radiotherapy have been controversial, and they might encourage clinicians to consider omission of radiotherapy in all or selected older women with low-risk breast cancer after breast-conserving surgery depending on the weight they and the patient give to local recurrence
Several characteristics have been identified to stratify lesions at high risk for recurrence:
These include:
Tumor size greater than 2 cm
Ulcerated
Location on the:
Lips / nose / forehead / chin and neck (H areas of the face)
Ill-defined borders
Previous radiation
Chronic scar
Immunosuppression
Recurrent tumors
Poor differentiation
Deep Clark level invasion
Presence of risk factors directs local therapy:
As lesions with no risk factors can be safely excised with 4 mm to 6 mm margins
With one or more risk factors:
Larger margins should be obtained, and 1-cm margins are recommended, if possible (given local tissue constraints)
The use of SLN biopsy for high-risk SCC has been reported in several small, single institutional reports:
However, its impact on patient outcomes has not been well defined
A highly successful alternative to standard surgical excision is Mohs micrographic surgery, performed by experienced dermatopathologists:
This involves serial resections of the tumor with real-time mapping and complete peripheral and deep pathologic evaluation to direct immediate further resection:
It has the lowest recurrence rates when compared to curettage / electrodessication, standard surgical excision, and radio therapy
Surgical excision with grossly negative margins, with immediate primary closure is inappropriate:
As the tumor’s size alone is a negative risk factor precluding smaller (4- to 6-mm) margins
References:
Brodland DG, Zitelli JA. Surgical margins for excision of primary cutaneous squamous cell carcinoma. J Am Acad Dermatol. 1992; 27:241-248.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Basal cell and squamous cell cancers. Available at: http://www.nccn.org.
Renzi C, Caggiati A, Mannooranparampil TJ, et al. Sentinel lymph node biopsy for high risk cutaneous squamous cell carcinoma: case series and review of the literature. Eur J Surg Oncol. 2007;33:364-369.
Rowe DE, Carroll RJ, Day CL Jr. Prognostic factors for local recurrence, metastasis, and survival rates in squamous cell carcinoma of the skin, ear, and lips: implications for treatment modality selection.J Am Acad Dermatol.1992;26:976-990.