My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Although many patients with hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)-negative early breast cancer:
Can be successfully treated with endocrine therapy:
A proportion are at risk of disease recurrence and death
Novel, effective treatments are needed to improve outcomes in this patient population:
Particularly for those at high risk of recurrence
Inhibitors of cyclin-dependent kinases (CDK) 4 and 6:
Have become standard of care for the adjuvant treatment of high-risk hormone receptor–positive / HER2-negative breast cancer
More than 90% of patients with breast cancer are diagnosed with early-stage disease:
Approximately 70% of whom have hormone receptor–positive / HER2-negative tumors
Standard therapy for hormone receptor–positive / HER2-negative early breast cancer:
Consists of adjuvant endocrine therapy (ie, aromatase inhibitors and / or antiestrogens) with or without ovarian suppression:
Meta-analyses have indicated that up to 20% of such patients experience disease recurrence within the first 10 years of endocrine therapy:
Including some who present with distant metastases
Risk of relapse is especially great for those with high-risk clinical or pathologic features:
Clinicopathologic features predictive of relapse for hormone receptor–positive / HER2-negative early breast cancer include:
Tumor size, grade
Nodal status
Increased Ki-67 expression level
Residual cancer burden
Genomic signature
CDK4/6 as a Therapeutic Target:
CDK4 and CDK6 are involved in regulating cell cycle progression and controlling proliferation
CDK4/6 regulation is altered in many solid tumors
CDK4/6 is often overexpressed in hormone receptor–positive breast cancers
CDK4/6 inhibitors:
Target the ATP binding site of CDK4 and CDK6:
Blocking their phosphorylation of Rb and inducing cell cycle arrest and apoptosis
These compounds differ in their structure and affinity for the ATP binding pocket of CDK4 and CDK6:
CDK4/6 inhibitors act in concert with endocrine therapy to inhibit breast cancer growth:
Providing the clinical rationale for combination therapy
Three CDK4/6 inhibitors:
Palbociclib, ribociclib, and abemaciclib:
Have been approved by the U.S. Food and Drug Administration (FDA) for the treatment of hormone receptor–positive / HER2-negative advanced or metastatic breast cancer (Table)
In phase III trials, treatment with these CDK4/6 inhibitors in combination with endocrine therapy:
Demonstrated improved progression-free survival compared to endocrine therapy alone:
Leading to their approval in this setting
In light of their benefit in advanced breast cancer, CDK4/6 inhibitors combined with endocrine therapy:
Were subsequently evaluated as adjuvant therapy for hormone receptor–positive / HER2-negative early breast cancer
Adjuvant Clinical Trials of CDK4/6 Inhibitors for Hormone Receptor–Positive/HER2-Negative Early Breast Cancer:
Three CDK4/6 inhibitors have been evaluated in combination with endocrine therapy as adjuvant therapy for hormone receptor–positive / HER2-negative early breast cancer:
Palbociclib, ribociclib, and abemaciclib
To date, only abemaciclib has demonstrated a benefit in invasive disease–free survival compared with endocrine therapy alone and is the only CDK4/6 inhibitor currently approved as adjuvant therapy:
For patients with hormone receptor–positive / HER2–negative, node-positive early breast cancer who are at high risk of recurrence and have a Ki-67 level ≥ 20%
Phase III Trials of CDK4/6 Inhibitors for Hormone Receptor–Positive/HER2-Negative Early Breast Cancer
Palbociclib:
Palbociclib therapy for hormone receptor–positive / HER2-negative early breast cancer has been studied in two phase III trials:
Although neither demonstrated a significant benefit from the addition of palbociclib to endocrine therapy
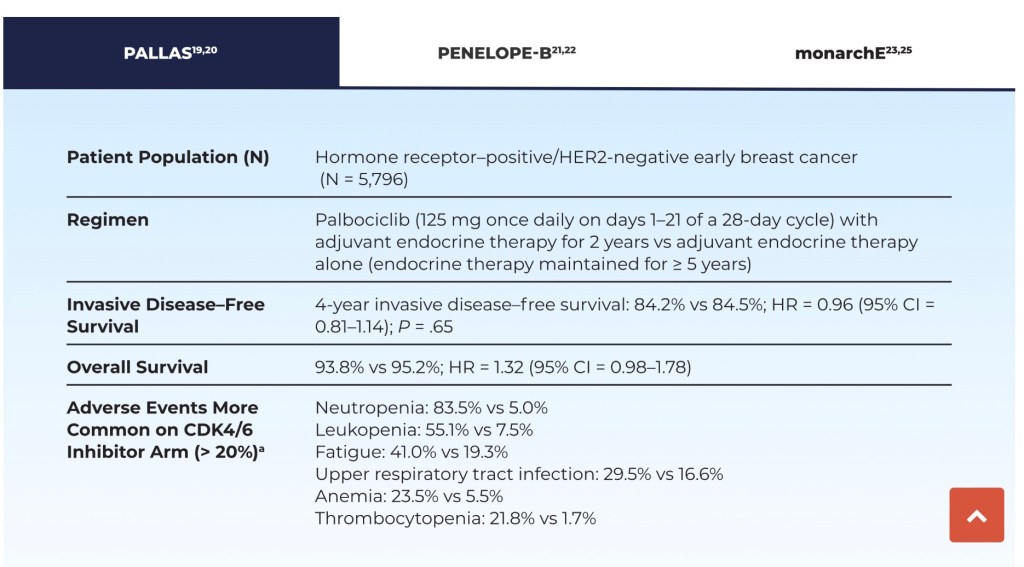
In the PALLAS study:
Patients received 2 years of palbociclib plus endocrine therapy or endocrine therapy alone as adjuvant therapy for hormone receptor–positive / HER2-negative high-risk breast cancer (with risk based on anatomic stage)
No statistically significant benefit was seen with palbociclib for 4-year invasive disease–free survival or other survival endpoints (Table)
The most common adverse events with palbociclib plus endocrine therapy were:
Leukopenia, fatigue, thrombocytopenia, anemia, upper respiratory tract infection, and alopecia:
With a significantly higher rate of grade 3/4 neutropenia with palbociclib/endocrine therapy compared with endocrine therapy alone:
61.3% vs 0.4%
Moreover, 42.2% of patients discontinued palbociclib prior to completion of the planned 2 years of therapy, mainly due to toxicity, based on protocol requirements
Palbociclib in combination with endocrine therapy:
Was also investigated in the PENELOPE-B trial in patients with hormone receptor–positive / HER2-negative breast cancer and residual invasive disease following resection and neoadjuvant chemotherapy who were at high risk of relapse (risk based on clinical pathologic staging–estrogen receptor grading)
At a median follow-up of nearly 43 months:
No significant increase was observed in estimated 3-year invasive disease–free survival or interim 3-year overall survival (Table 2)
The most common adverse events with palbociclib plus endocrine therapy were neutropenia, leukopenia, thrombocytopenia, anemia, hypocalcemia, fatigue, stomatitis, constipation, cough, and infection:
The incidence of grade 3/4 neutropenia (70% vs 1%) and leukopenia (56% vs 1%) was significantly increased on the palbociclib arm
MonarchE
Abemaciclib
The monarchE phase III trial compared treatment with abemaciclib plus endocrine therapy to endocrine therapy alone in patients with hormone receptor–positive / HER2-negative early breast cancer who were at high risk of recurrence (based on positive lymph node status, tumor size, histologic grade, and Ki-67 score ≥ 20%):
At the 27-month and 42-month follow-up analyses:
Patients had a clinically meaningful improvement in invasive disease–free survival with abemaciclib-based therapy compared with the control treatment (Table)
The abemaciclib regimen reduced the relative risk of recurrence by about 30%:
These were mostly distant recurrences:
With longer follow-up, we hope that it will also improve overall survival outcomes
The incidence of treatment-related adverse events was higher with abemaciclib (98.4% vs 88.8%):
The most common of which were diarrhea, infections, neutropenia, fatigue, leukopenia, nausea, anemia, and headache:
Grade 3/4 adverse events were also more frequent with abemaciclib (49.7% vs 16.3%), with a higher discontinuation rate during study treatment (18.5% vs 1.1%)
Results of the monarchE trial led to FDA approval of abemaciclib in combination with endocrine therapy as adjuvant therapy for high-risk patients with hormone receptor–positive / HER2-negative, node-positive early breast cancer and a Ki-67 score ≥ 20%
Both the American Society of Clinical Oncology (ASCO) and National Comprehensive Cancer Network® (NCCN) guidelines:
Indicate that abemaciclib plus endocrine therapy can be considered for treatment of patients with hormone receptor–positive / HER2-negative, node-positive early breast cancer with high risk of recurrence:
Since diarrhea (all grades) occurred in over 80% of patients on the abemaciclib arm in monarchE, patients should be educated on the risk of diarrhea and approaches for mitigation
Venous thromboembolism can also occur with abemaciclib therapy (2.3% incidence, all grades, in monarchE24):
Caution should be exerted when combining abemaciclib with tamoxifen because both agents can increase risk of thromboembolism:
If possible, an aromatase inhibitor with or without ovarian suppression should be used as the preferred endocrine partner with abemaciclib
Ribociclib
While proven effective for hormone receptor–positive / HER2-negative advanced or metastatic breast cancer:
Ribociclib has not yet conclusively demonstrated efficacy in hormone receptor–positive / HER2-negative early breast cancer, although several trials are ongoing
The phase II LEADER trial (ClinicalTrials.gov identifier NCT03285412) evaluated 1 year of continuous or intermittent ribociclib in this setting:
An interim safety analysis revealed that approximately one-third of patients discontinued ribociclib, largely within the first few months of treatment:
The most common grade ≥ 3 adverse events resulting in study discontinuation were neutropenia, alanine aminotransferase increase, and aspartate aminotransferase increase
Circulating tumor DNA (ctDNA) analysis:
Revealed a strong association between detectable ctDNA and disease recurrence
ADAPTcycle (NCT04055493) is a phase III trial:
Comparing ribociclib plus endocrine therapy to chemotherapy in patients with intermediate-risk hormone receptor–positive / HER2-negative early breast cancer (with risk determined by Oncotype DX score and response to 3 weeks of preoperative endocrine therapy)
Another phase III trial, NATALEE (NCT03701334):
Is evaluating adjuvant ribociclib and anastrozole in patients with hormone receptor–positive / HER2-negative early breast cancer
It should be noted that approved dosing differs for these three CDK4 / 6 inhibitors:
The shorter half-life of abemaciclib (18.3 hours vs 29.0–32.0 hours for palbociclib and ribociclib):
Requires twice-daily dosing to maintain steady-state concentrations:
Whereas palbociclib and ribociclib are administered daily for 3 weeks followed by 1-week rest
Dosing for palbociclib and ribociclib is based on trials in advanced or metastatic breast cancer since they are not currently approved for early breast cancer
Ki-67 Expression
Expression of the nuclear protein Ki-67 is strongly correlated with breast cancer cell proliferation
In patients with hormone receptor–positive / HER2-negative early breast cancer:
Ki-67 expression was prognostic for survival:
With higher expression levels predicting lower 5-year disease-free survival rates
Two large meta-analyses reported Ki-67 cutoffs of 19% and 25% as prognostic for poor survival:
Leading to consideration of a cutoff of ≥ 20% as prognostic for survival in patients with hormone receptor–positive breast cancer
In monarchE:
Patients with high (≥ 20%) Ki-67 expression had a clinically meaningful increased risk of developing invasive disease within 2 years compared with those with low Ki-67, with 2-year invasive disease–free survival rates of 86.1% (95% confidence interval [CI] = 83.1%–88.7%) and 92.0% (95% CI = 89.7%–93.9%), respectively
Because approval of abemaciclib as adjuvant therapy for hormone receptor–positive / HER2-negative early breast cancer was based in part on a Ki-67 score ≥ 20%:
Tumor Ki-67 expression level should be assessed when considering use of abemaciclib in this setting
Ki-67 expression should be measured using an FDA-approved test based on either immunohistochemistry (MIB-1 pharmDx) or molecular profiling (Oncotype DX 21-gene recurrence score)
Since benefit for abemaciclib was seen in patients with tumors having either low or high Ki-67:
ASCO and NCCN guidelines (in contrast to the FDA indication) suggest that adjuvant abemaciclib may be considered for all patients with hormone receptor–positive / HER2-negative early breast cancer:
Based on monarchE intent-to-treat results (which included patients with low and high Ki-67 expression)
This is based in part, based on the fact that laboratory assessment of Ki-67 can be quite variable because of differences in immunohistochemistry procedures and interpretation of scoring relative to the 20% cutoff level, which could result in some otherwise eligible patients being denied treatment
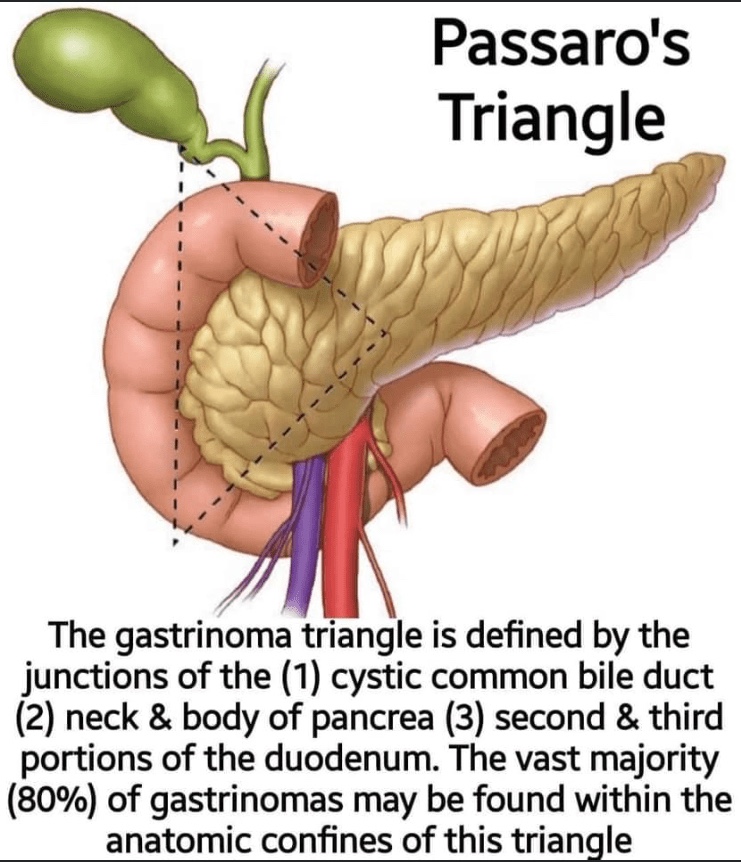
Edward Peter Passaro (1930-2017) was an American GI surgeon, who described his eponymous triangle in 1984.
👉Gastrinomas secrete supra-physiologic levels of the hormone gastrin, resulting in a clinical syndrome (Zollinger-Ellison syndrome [ZES]), whereby the hypersecretion of gastric acid results in peptic ulcer disease & diarrhea. Common locations for gastrinomas are in the pancreatic head & duodenum, although extra-anatomic tumors may arise in 5% to 15% of cases.
👉The gastrinoma triangle, defined by the junctions of the (1) cystic duct and common bile duct (2) neck & body of the pancreas, and (3) second & third portions of the duodenum, therefore encompasses the majority of gastrinomas
👉Pancreatic gastrinomas comprise 25% of all gastrinomas, & most (50% to 88%) arise in the duodenum, most often in the first portion of the duodenum. There is a predilection for males with ZES; approximately 20% of cases occur in association with MEN-1, and the remaining 80% are sporadic.
The Multicenter Selective Lymphadenectomy Trial 2 (MSLT-2):
Was recently published in June 2017:
Which evaluated completion lymphadenectomy versus observation following positive sentinel lymph node biopsies for metastatic melanoma
There was no significant difference:
In disease-specific survival among the two treatment groups
Key limitations to the study were:
That it mostly included patients with a low burden of disease (% nodal involvement, largest metastatic focus, and number of positive nodes) in their sentinel lymph nodes
The study has limited median follow-up:
43 months
Furthermore, it is important to note that there was a significant difference in disease-free survival between groups and that subjects in the study did not receive contemporary systemic therapy
Debate remains for which subset of patients would benefit most from completion lymphadenectomy:
However, it is reasonable for most of these patients to be observed closely with:
Nodal ultrasounds:
Every 4 months for the first 2 years
Every 6 months for years 3 to 5
Then annually.
References:
Faries MB, Thompson JF, Cochran AJ, et al. Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma. N Engl J Med. 2017; 376(23): 2211-2222.
Was a phase 3 clinical trial that randomized postmenopausal women with ER+ DCIS (n = 3,104) to either 5 years of anastrozole or tamoxifen following breast-conserving surgery and radiation
The trial sought to determine how effective anastrozole was compared to tamoxifen in preventing a breast cancer occurrence
With a median follow-up of 9 years:
Investigators found significantly fewer breast cancer events in the anastrozole group (n = 90) than in the tamoxifen group (n = 122)
The 10-year breast cancer event rate was lower among women randomized to anastrozole compared to tamoxifen:
6.9% [anastrozole] vs. 10.9% [tamoxifen], HR 0.73, p=0.02:
This recorded difference in breast cancer events was attributable almost entirely to younger postmenopausal women less than 60 years of age who received tamoxifen:
Women less than 60 receiving tamoxifen had nearly twice the events as those receiving anastrozole:
Events on tamoxifen: 63 vs events on anastrozole: 34, HR 0.53 (0.35-0.80), p=0.0026
Interestingly, the difference between treatments did not become apparent until after 5 years of follow-up, likely due to the low number of events in both groups
There was no difference in overall survival (OS) between the two treatment groups:
The 10-year estimates for overall survival were 92.1% for the tamoxifen group and 92.5% for the anastrozole group (p=0.38)
In B-35, anastrozole was found to further significantly reduce the rate of contralateral invasive cancer compared with tamoxifen
Based on this trial and others:
Aromatase inhibitors are the preferred adjuvant hormonal therapy for ER+ disease in post-menopausal women with either DCIS or invasive breast cancer, provided they have no contraindications to taking an aromatase inhibitor
References
Margolese RG, Cecchini RS, Julian TB, Ganz PA, Constantino JP, Vallow LA, et al. Anastrozole versus tamoxifen in postmenopausal women with ductal carcinoma in situ undergoing lumpectomy plus radiotherapy (NSABP B-35): a randomised, double-blind, phase 3 clinical trial. Lancet. 2016;387(10021):849-856
M Baum, AU Budzar, J Cuzick, et al., ATAC Trialists’ Group. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomized trial. Lancet. 2002;359(9324):2131-2139.
Eccrine carcinoma is an extremely rare neoplasm of the skin:
That accounts for approximately 0.005% of malignant epithelial neoplasia
It arises from the eccrine sweat glands:
There are least 10 described subtypes
Due to the rarity of these neoplasms:
Exact etiology and clinical recommendations are not clear
Most of these tumors are:
Slow-growing, solitary, dermal nodules:
That often arise from pre-existing benign skin lesions
Most common distribution is seen in:
The head, neck, and extremities
The diagnosis is often delayed:
Because of its relative rarity as well as difficulty in identification with traditional light microscopy
Recurrence is common
A wide local excision is the recommended treatment of choice:
With a 70% to 80% cure rate
Mohs microsurgery:
Can be used on cosmetically sensitive areas
Predictive factors for recurrence include:
Tumors thicker than 7 mm
Lymphovascular invasion
Greater than 14 mitoses per high power field
Dermal infiltration
Performing SLN biopsy on these patients is controversial:
Lymph node metastasis is relatively rare and sentinel lymph node biopsy:
Is not routinely performed for all cases
Distant metastases are rare and cross-sectional imaging for staging work-up should be performed only when clinically indicated
Recurrent tumors:
Are high risk for locoregional failure:
Should be considered for a sentinel lymph node biopsy
Distant metastasis is rare and any additional staging scans are not recommended
Radiation and chemotherapy have not demonstrated any significant benefit in the adjuvant setting
References
Barnes M, Hestley A, Murray DR, Carlson GW, Parker D, Delman KA. The risk of lymph node involvement in malignant cutaneous adnexal tumors. Am Surg. 2014;80:270-274.
The hallux and thumb are the most commonly affected sites
Antecedent trauma:
Has been reported in 25% to 55% of patients
Diagnosis is often delayed because of:
Inadequate biopsies
Lesion neglect
Confusion with benign melanonychia, hematoma, chronic trauma, or fungal nail infection (onychomycosis)
The classic features suggestive of melanoma include:
Melanotic lesions arising from the nail matrix and longitudinal melanonychia:
Defined as a band of pigmentation extending from the proximal nail fold / lunula throughout the nail to the free edge
Any band greater than 3 mm in width or associated with discoloration of the lateral or proximal nail folds (Hutchinson’s sign):
Mandates biopsy of the nail matrix and bed with either incisional or punch techniques:
Partial or total avulsion of the nail plate is usually needed to perform biopsy
Management of these lesions requires sound oncologic resection with consideration of functional deficits:
Margin principles in melanoma are maintained:
Which means amputation is often necessary
Special consideration is given to the hallux and thumb:
As the complete loss of either can cause substantial disability
For the hallux amputation of the digit preserves the metatarsal head, and for the thumb, efforts are made to preserve bone proximal to the interphalangeal joint, if appropriate margins allow:
Excision of the nail bed, matrix, and proximal nail fold will not provide adequate margins
Mohs micrographic surgery has been used in several small series for selected cases of melanoma-in-situ only, and this technique would not provide adequate resection of this melanoma deeper melanomas
Amputation of the thumb just proximal to the interphalangeal joint is the best approach:
As it provides for adequate margins while preserving a stump for some functional use. Radical amputation would also provide adequate margins, but the functional deficit created is unnecessary
References:
Ross MI. Excision of primary melanoma. In: Balch CM, Houghton AN, Sober AJ, Soong S-J, eds. Cutaneous Melanoma. 5th ed. St. Louis: Quality Medical Publishing; 2009:251-274.
Sureda N, Phan A, Poulalhon N, Balme B, Dalle S, Thomas L. Conservative surgical management of subungal (matrix derived) melanoma: report of seven cases and literature review. Br J Dermatol. 2011;165:852-858.
Tan KB, Moncrieff M, Thompson JF, et al. Subungual melanoma: a study of 124 cases highlighting features of early lesions, potential pitfalls in diagnosis, and guidelines for histologic reporting. Am J Surg Pathol. 2007;31:1902-1912.