- Although many patients with hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)-negative early breast cancer:
- Can be successfully treated with endocrine therapy:
- A proportion are at risk of disease recurrence and death
- Can be successfully treated with endocrine therapy:
- Novel, effective treatments are needed to improve outcomes in this patient population:
- Particularly for those at high risk of recurrence
- Inhibitors of cyclin-dependent kinases (CDK) 4 and 6:
- Have become standard of care for the adjuvant treatment of high-risk hormone receptor–positive / HER2-negative breast cancer
- More than 90% of patients with breast cancer are diagnosed with early-stage disease:
- Approximately 70% of whom have hormone receptor–positive / HER2-negative tumors
- Standard therapy for hormone receptor–positive / HER2-negative early breast cancer:
- Consists of adjuvant endocrine therapy (ie, aromatase inhibitors and / or antiestrogens) with or without ovarian suppression:
- Meta-analyses have indicated that up to 20% of such patients experience disease recurrence within the first 10 years of endocrine therapy:
- Including some who present with distant metastases
- Risk of relapse is especially great for those with high-risk clinical or pathologic features:
- Clinicopathologic features predictive of relapse for hormone receptor–positive / HER2-negative early breast cancer include:
- Tumor size, grade
- Nodal status
- Increased Ki-67 expression level
- Residual cancer burden
- Genomic signature
- Clinicopathologic features predictive of relapse for hormone receptor–positive / HER2-negative early breast cancer include:
- Meta-analyses have indicated that up to 20% of such patients experience disease recurrence within the first 10 years of endocrine therapy:
- Consists of adjuvant endocrine therapy (ie, aromatase inhibitors and / or antiestrogens) with or without ovarian suppression:
- CDK4/6 as a Therapeutic Target:
- CDK4 and CDK6 are involved in regulating cell cycle progression and controlling proliferation
- CDK4/6 regulation is altered in many solid tumors
- CDK4/6 is often overexpressed in hormone receptor–positive breast cancers
- CDK4/6 inhibitors:
- Target the ATP binding site of CDK4 and CDK6:
- Blocking their phosphorylation of Rb and inducing cell cycle arrest and apoptosis
- These compounds differ in their structure and affinity for the ATP binding pocket of CDK4 and CDK6:
- CDK4/6 inhibitors act in concert with endocrine therapy to inhibit breast cancer growth:
- Providing the clinical rationale for combination therapy
- CDK4/6 inhibitors act in concert with endocrine therapy to inhibit breast cancer growth:
- Target the ATP binding site of CDK4 and CDK6:
- Three CDK4/6 inhibitors:
- Palbociclib, ribociclib, and abemaciclib:
- Have been approved by the U.S. Food and Drug Administration (FDA) for the treatment of hormone receptor–positive / HER2-negative advanced or metastatic breast cancer (Table)
- In phase III trials, treatment with these CDK4/6 inhibitors in combination with endocrine therapy:
- Demonstrated improved progression-free survival compared to endocrine therapy alone:
- Leading to their approval in this setting
- Demonstrated improved progression-free survival compared to endocrine therapy alone:
- Palbociclib, ribociclib, and abemaciclib:
- In light of their benefit in advanced breast cancer, CDK4/6 inhibitors combined with endocrine therapy:
- Were subsequently evaluated as adjuvant therapy for hormone receptor–positive / HER2-negative early breast cancer

- Adjuvant Clinical Trials of CDK4/6 Inhibitors for Hormone Receptor–Positive/HER2-Negative Early Breast Cancer:
- Three CDK4/6 inhibitors have been evaluated in combination with endocrine therapy as adjuvant therapy for hormone receptor–positive / HER2-negative early breast cancer:
- Palbociclib, ribociclib, and abemaciclib
- To date, only abemaciclib has demonstrated a benefit in invasive disease–free survival compared with endocrine therapy alone and is the only CDK4/6 inhibitor currently approved as adjuvant therapy:
- For patients with hormone receptor–positive / HER2–negative, node-positive early breast cancer who are at high risk of recurrence and have a Ki-67 level ≥ 20%
- Three CDK4/6 inhibitors have been evaluated in combination with endocrine therapy as adjuvant therapy for hormone receptor–positive / HER2-negative early breast cancer:
- Palbociclib:
- Palbociclib therapy for hormone receptor–positive / HER2-negative early breast cancer has been studied in two phase III trials:
- Although neither demonstrated a significant benefit from the addition of palbociclib to endocrine therapy
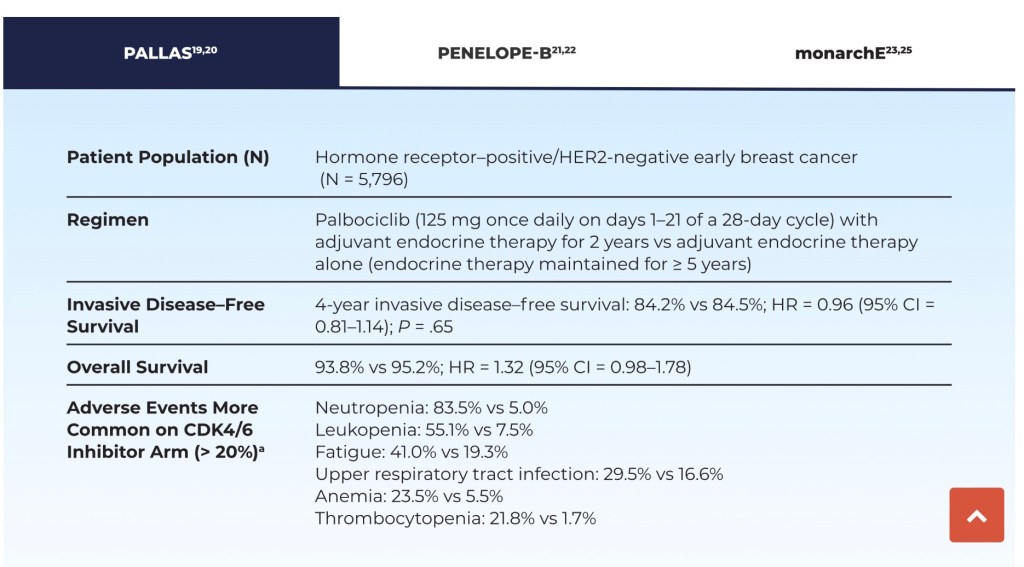
- In the PALLAS study:
- Patients received 2 years of palbociclib plus endocrine therapy or endocrine therapy alone as adjuvant therapy for hormone receptor–positive / HER2-negative high-risk breast cancer (with risk based on anatomic stage)
- No statistically significant benefit was seen with palbociclib for 4-year invasive disease–free survival or other survival endpoints (Table)
- The most common adverse events with palbociclib plus endocrine therapy were:
- Leukopenia, fatigue, thrombocytopenia, anemia, upper respiratory tract infection, and alopecia:
- With a significantly higher rate of grade 3/4 neutropenia with palbociclib/endocrine therapy compared with endocrine therapy alone:
- 61.3% vs 0.4%
- With a significantly higher rate of grade 3/4 neutropenia with palbociclib/endocrine therapy compared with endocrine therapy alone:
- Leukopenia, fatigue, thrombocytopenia, anemia, upper respiratory tract infection, and alopecia:
- Moreover, 42.2% of patients discontinued palbociclib prior to completion of the planned 2 years of therapy, mainly due to toxicity, based on protocol requirements
- Palbociclib therapy for hormone receptor–positive / HER2-negative early breast cancer has been studied in two phase III trials:
- Palbociclib in combination with endocrine therapy:
- Was also investigated in the PENELOPE-B trial in patients with hormone receptor–positive / HER2-negative breast cancer and residual invasive disease following resection and neoadjuvant chemotherapy who were at high risk of relapse (risk based on clinical pathologic staging–estrogen receptor grading)
- At a median follow-up of nearly 43 months:
- No significant increase was observed in estimated 3-year invasive disease–free survival or interim 3-year overall survival (Table 2)
- The most common adverse events with palbociclib plus endocrine therapy were neutropenia, leukopenia, thrombocytopenia, anemia, hypocalcemia, fatigue, stomatitis, constipation, cough, and infection:
- The incidence of grade 3/4 neutropenia (70% vs 1%) and leukopenia (56% vs 1%) was significantly increased on the palbociclib arm
- At a median follow-up of nearly 43 months:
- Was also investigated in the PENELOPE-B trial in patients with hormone receptor–positive / HER2-negative breast cancer and residual invasive disease following resection and neoadjuvant chemotherapy who were at high risk of relapse (risk based on clinical pathologic staging–estrogen receptor grading)

- Abemaciclib
- The monarchE phase III trial compared treatment with abemaciclib plus endocrine therapy to endocrine therapy alone in patients with hormone receptor–positive / HER2-negative early breast cancer who were at high risk of recurrence (based on positive lymph node status, tumor size, histologic grade, and Ki-67 score ≥ 20%):
- At the 27-month and 42-month follow-up analyses:
- Patients had a clinically meaningful improvement in invasive disease–free survival with abemaciclib-based therapy compared with the control treatment (Table)
- The abemaciclib regimen reduced the relative risk of recurrence by about 30%:
- These were mostly distant recurrences:
- With longer follow-up, we hope that it will also improve overall survival outcomes
- These were mostly distant recurrences:
- At the 27-month and 42-month follow-up analyses:
- The monarchE phase III trial compared treatment with abemaciclib plus endocrine therapy to endocrine therapy alone in patients with hormone receptor–positive / HER2-negative early breast cancer who were at high risk of recurrence (based on positive lymph node status, tumor size, histologic grade, and Ki-67 score ≥ 20%):
- The incidence of treatment-related adverse events was higher with abemaciclib (98.4% vs 88.8%):
- The most common of which were diarrhea, infections, neutropenia, fatigue, leukopenia, nausea, anemia, and headache:
- Grade 3/4 adverse events were also more frequent with abemaciclib (49.7% vs 16.3%), with a higher discontinuation rate during study treatment (18.5% vs 1.1%)
- The most common of which were diarrhea, infections, neutropenia, fatigue, leukopenia, nausea, anemia, and headache:
- Results of the monarchE trial led to FDA approval of abemaciclib in combination with endocrine therapy as adjuvant therapy for high-risk patients with hormone receptor–positive / HER2-negative, node-positive early breast cancer and a Ki-67 score ≥ 20%
- Both the American Society of Clinical Oncology (ASCO) and National Comprehensive Cancer Network® (NCCN) guidelines:
- Indicate that abemaciclib plus endocrine therapy can be considered for treatment of patients with hormone receptor–positive / HER2-negative, node-positive early breast cancer with high risk of recurrence:
- Since diarrhea (all grades) occurred in over 80% of patients on the abemaciclib arm in monarchE, patients should be educated on the risk of diarrhea and approaches for mitigation
- Venous thromboembolism can also occur with abemaciclib therapy (2.3% incidence, all grades, in monarchE24):
- Caution should be exerted when combining abemaciclib with tamoxifen because both agents can increase risk of thromboembolism:
- If possible, an aromatase inhibitor with or without ovarian suppression should be used as the preferred endocrine partner with abemaciclib
- Caution should be exerted when combining abemaciclib with tamoxifen because both agents can increase risk of thromboembolism:
- Indicate that abemaciclib plus endocrine therapy can be considered for treatment of patients with hormone receptor–positive / HER2-negative, node-positive early breast cancer with high risk of recurrence:
- Ribociclib
- While proven effective for hormone receptor–positive / HER2-negative advanced or metastatic breast cancer:
- Ribociclib has not yet conclusively demonstrated efficacy in hormone receptor–positive / HER2-negative early breast cancer, although several trials are ongoing
- The phase II LEADER trial (ClinicalTrials.gov identifier NCT03285412) evaluated 1 year of continuous or intermittent ribociclib in this setting:
- An interim safety analysis revealed that approximately one-third of patients discontinued ribociclib, largely within the first few months of treatment:
- The most common grade ≥ 3 adverse events resulting in study discontinuation were neutropenia, alanine aminotransferase increase, and aspartate aminotransferase increase
- Circulating tumor DNA (ctDNA) analysis:
- Revealed a strong association between detectable ctDNA and disease recurrence
- An interim safety analysis revealed that approximately one-third of patients discontinued ribociclib, largely within the first few months of treatment:
- ADAPTcycle (NCT04055493) is a phase III trial:
- Comparing ribociclib plus endocrine therapy to chemotherapy in patients with intermediate-risk hormone receptor–positive / HER2-negative early breast cancer (with risk determined by Oncotype DX score and response to 3 weeks of preoperative endocrine therapy)
- Another phase III trial, NATALEE (NCT03701334):
- Is evaluating adjuvant ribociclib and anastrozole in patients with hormone receptor–positive / HER2-negative early breast cancer
- While proven effective for hormone receptor–positive / HER2-negative advanced or metastatic breast cancer:
- It should be noted that approved dosing differs for these three CDK4 / 6 inhibitors:
- The shorter half-life of abemaciclib (18.3 hours vs 29.0–32.0 hours for palbociclib and ribociclib):
- Requires twice-daily dosing to maintain steady-state concentrations:
- Whereas palbociclib and ribociclib are administered daily for 3 weeks followed by 1-week rest
- Dosing for palbociclib and ribociclib is based on trials in advanced or metastatic breast cancer since they are not currently approved for early breast cancer
- Requires twice-daily dosing to maintain steady-state concentrations:
- The shorter half-life of abemaciclib (18.3 hours vs 29.0–32.0 hours for palbociclib and ribociclib):
- Ki-67 Expression
- Expression of the nuclear protein Ki-67 is strongly correlated with breast cancer cell proliferation
- In patients with hormone receptor–positive / HER2-negative early breast cancer:
- Ki-67 expression was prognostic for survival:
- With higher expression levels predicting lower 5-year disease-free survival rates
- Ki-67 expression was prognostic for survival:
- Two large meta-analyses reported Ki-67 cutoffs of 19% and 25% as prognostic for poor survival:
- Leading to consideration of a cutoff of ≥ 20% as prognostic for survival in patients with hormone receptor–positive breast cancer
- In monarchE:
- Patients with high (≥ 20%) Ki-67 expression had a clinically meaningful increased risk of developing invasive disease within 2 years compared with those with low Ki-67, with 2-year invasive disease–free survival rates of 86.1% (95% confidence interval [CI] = 83.1%–88.7%) and 92.0% (95% CI = 89.7%–93.9%), respectively
- Because approval of abemaciclib as adjuvant therapy for hormone receptor–positive / HER2-negative early breast cancer was based in part on a Ki-67 score ≥ 20%:
- Tumor Ki-67 expression level should be assessed when considering use of abemaciclib in this setting
- Ki-67 expression should be measured using an FDA-approved test based on either immunohistochemistry (MIB-1 pharmDx) or molecular profiling (Oncotype DX 21-gene recurrence score)
- Since benefit for abemaciclib was seen in patients with tumors having either low or high Ki-67:
- ASCO and NCCN guidelines (in contrast to the FDA indication) suggest that adjuvant abemaciclib may be considered for all patients with hormone receptor–positive / HER2-negative early breast cancer:
- Based on monarchE intent-to-treat results (which included patients with low and high Ki-67 expression)
- This is based in part, based on the fact that laboratory assessment of Ki-67 can be quite variable because of differences in immunohistochemistry procedures and interpretation of scoring relative to the 20% cutoff level, which could result in some otherwise eligible patients being denied treatment
- ASCO and NCCN guidelines (in contrast to the FDA indication) suggest that adjuvant abemaciclib may be considered for all patients with hormone receptor–positive / HER2-negative early breast cancer:

