My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
The use of an aromatase inhibitor (letrozole) with an inhibitor of the cyclin dependent kinases 4 and 6 (ribociclib):
Was compared with an aromatase inhibitor alone in postmenopausal women with hormone receptor positive HER2-negative metastatic breast cancer:
In the MONALEESA-2 study
MONALEESA-2 Trial:
Results showed an improvement with the addition of ribociclib to letrozole alone in:
Progression-free survival (PFS):
From 42.2% to 63%
Overall response rate:
From 37.1% to 52.7%
This regimen was also investigated in premenopausal women with advanced, hormone receptor-positive breast cancer, and improved PFS compared with placebo plus endocrine therapy
References
Hortobagi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, Paluch-Shimon S, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med.2016;375(18)1738-1748.
Tripathy D, Im SA2, Colleoni M3, Franke F4, Bardia A5, Harbeck Nm et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised phase 3 trial. Lancet Oncol. 2018;19(7):904-915.
A mandibulotomy can be performed in one of three locations:
Lateral:
Through the body or angle of the mandible
Midline
Paramedian
A lateral mandibulotomy has several disadvantages:
First, the muscular pull on the two segments of the mandible is unequal:
Putting the mandibulotomy site under significant stress and causing a delay in healing:
For this reason, intermaxillary fixation may be required
Second, the ability to gain access to the suture line to maintain cleanliness following surgery in the oral cavity is hampered as a result of intermaxillary fixationleading to poor oral hygiene and the potential risk for sepsis of the suture line
Third, a lateral mandibulotomy poses several anatomic disadvantages including:
Denervation of the teeth distal to the mandibulotomy site and the skin of the chin:
As a result of transection of the inferior alveolar nerve
A lateral mandibulotomy also causes devascularization of the distal teeth and the distal segment of the mandible:
From its endosteal blood supply
The exposure provided by a lateral mandibulotomy:
Is limited
If the patient needs postoperative radiation therapy:
Delayed healing can lead to complications at the site of the mandibulotomy
For these reasons, a lateral mandibulotomy:
Is not recommended
By placing the mandibulotomy in the anterior midline:
All the disadvantages of a lateral mandibulotolotomy:
Are avoided
However, splitting the mandible in the midline:
Requires extraction of one central incisor tooth:
To avoid exposure of the roots of both central incisor teeth:
Which are at risk of extrusion
Extraction of one central incisor tooth alters the aesthetic appearance of the lower dentition
In addition, a midline mandibulotomy requires:
Division of muscles arising from the genial tubercle, that is:
The geniohyoid and genioglossus:
Leading to a delayed recovery of the functions of mastication and swallowing
Therefore a median mandibulotomy:
Also is not preferred for these reasons
A paramedian mandibulotomy:
On the other hand, avoids all the disadvantages of a lateral mandibulotomy and the sequelae of a midline mandibulotomy
It offers significant advantages, such as:
Wide exposure
Preservation of the geniohyoid and genioglossus muscles:
Leading to preservation of the hyomandibular complex
The only muscle requiring division is the mylohyoid muscle:
Which leads to minimal swallowing difficulties
A paramedian mandibulotomy:
Does not cause denervation or devascularization of the skin of the chin or the teeth and mandible
Fixation at the mandibulotomy site is easy
The site of the mandibulotomy is able to withstand radiation therapy if the patient needs postoperative treatment
Thus at present a paramedian mandibulotomy:
Remains an optimal surgical approach for access to posteriorly located larger lesions of the oral cavity and tumors of the oropharynx and parapharyngeal space
Are available for resection of primary tumors of the oral cavity
The choice of a particularapproach will depend on factors such as:
The size and site (anterior versus posterior) of the primary tumor
As well as its depth of invasion
Proximity to the mandible or maxilla
Factorssuch as dentition, size of the oral aperture, trismus, and the size and mobility of the tongue:
Also influence selection of the surgical approach
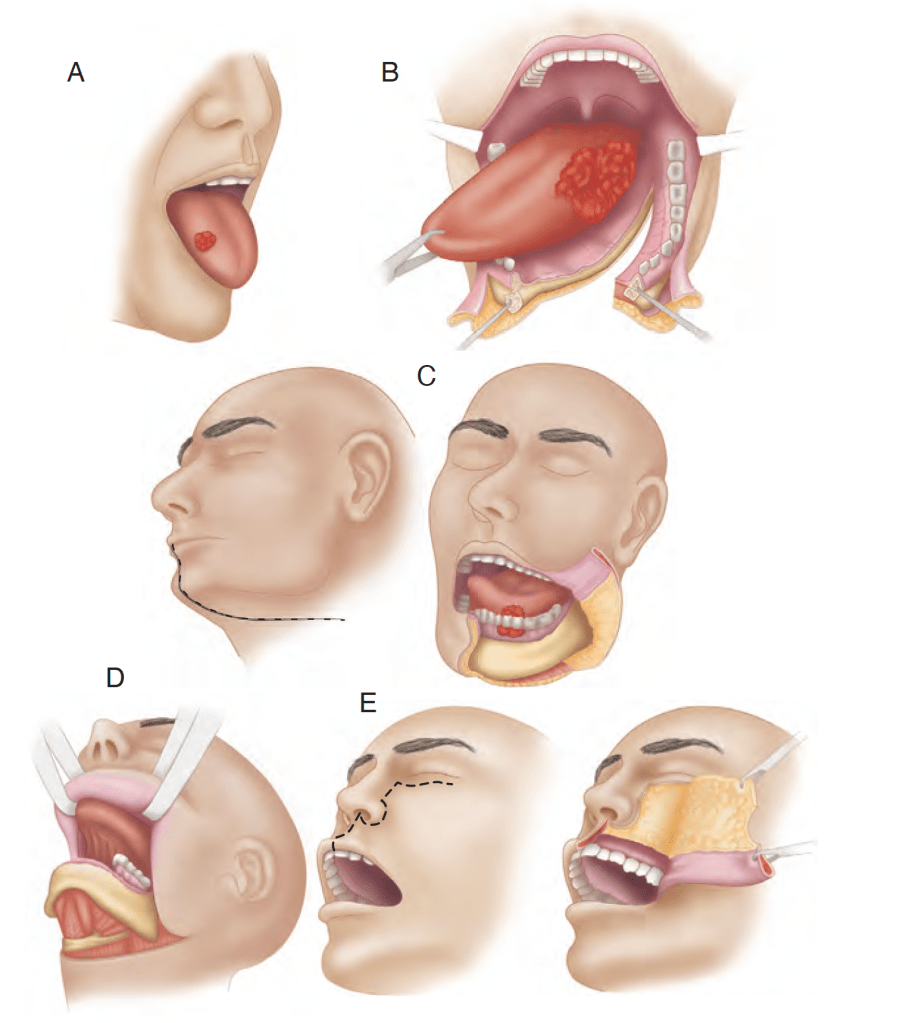
The various surgical approaches such as:
Peroral, mandibulotomy, lower cheek flap approach, visor flap approach, and upper cheek flap approach are shown in Figure
The transoral approach has wider applications with technologic advances using:
Lasers (transoral laser microsurgery [TLM]) and robotics (transoral robotic surgery [TORS])
Various surgical approaches. A, Peroral. B, Mandibulotomy. C, Lower cheek flap. D, Visor flap. E, Upper cheek flap.
When the peroral approach does not offer adequate exposure:
The visor flap or cheek flap approaches (upper or lower) become necessary
The visor flap approach:
Provides sufficient exposure for anteriorly located lesions:
But is not satisfactory for tumors located in the posterior oral cavity
The benefit of this approach is that it avoids a lower lip–splitting incision:
But produces permanent numbness of the chin:
Because the mental nerves need to be transected for adequate mobilization of the flap
It also may cause sagging of the lower lip and drooling:
Because of a loss of support and sensation:
Thus its utility is limited
The lower cheek flap approach:
Requires a midline lip–splitting incision that is continued laterally into the neck for exposureand neck dissection:
This approach provides excellent exposure for nearly all tumors of the oral cavity:
Except those of the upper gum and hard palate
Mandible resection (marginal or segmental) and reconstruction:
Require the lower cheek flap approach in most instances
The lower cheek flap approach:
Is required for marginal or segmental mandibulectomy of tumors adjacent to the body of the mandible
The upper cheek flap approach (the Weber-Ferguson incision and its modifications):
Is required for resection of larger tumors of the hard palate and upper alveolus:
Particularly if they are posteriorly located
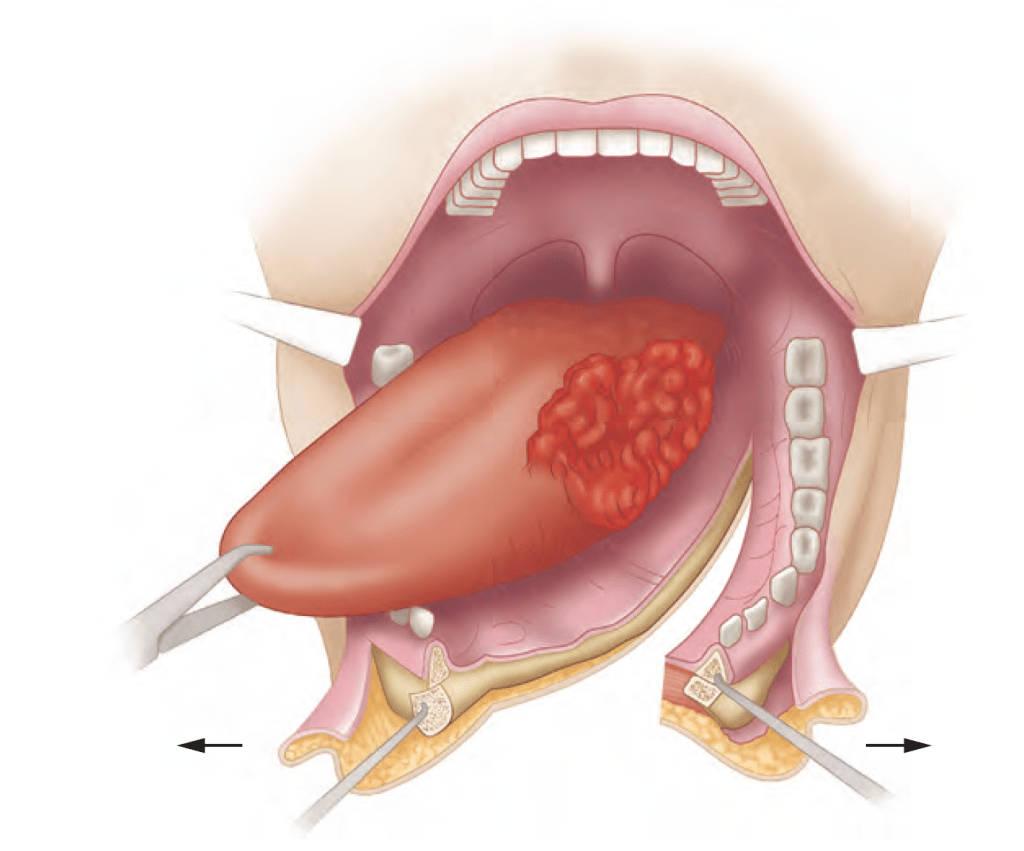
Access to larger tumors of the tongue, particularly those closer to the base of the tonguewhere the mandible is not involved:
Requires wider exposure for resection:
A mandibulotomy or mandibular osteotomy is an excellent mandible sparing surgical approach designed to gain access to the oral cavity or oropharynx for resection of primary tumors otherwise not accessible through the open mouth or by the lower cheek flap approach (Figure)
A mandibulotomy is an excellent mandible-sparing surgical approach to gain access to bulky tumors of the oral cavity or oropharynx.
The latest National Comprehensive Cancer Network (NCCN) clinical practice guidelines:
Have added fluoroestradiol F18 (FES) PET scan to its list of considerations for patients with recurrent or metastatic ER breast cancer
The NCCN guideline now recommends clinicians consider the use of FES PET for ER-positive disease during work-up of patients with recurrent or metastatic breast cancer
The guideline update follows the publication of the Society of Nuclear Medicine and Molecular Imaging’s appropriate use criteria statement on ER-targeted PET imaging in March of 2023:
Which noted that FES PET is appropriate when a clinician is considering endocrine therapy and assessing ER status at initial diagnosis of metastatic breast cancer, when the disease progresses after endocrine therapy, when lesions are challenging or dangerous to biopsy, and / or when other tests evaluating ER status are inconclusive
The addition to FES PET in the NCCN guidelines in addition to fluorodeoxyglucose gives clinicians an opportunity to assess ER function in all tumor sites in patients with ER-positive metastatic breast cancer
FES was approved by the FDA for use as an adjunct to biopsy in patients with recurrent or metastatic breast cancer in May 2020 and is currently the only imaging agent approved by the agency for that indication:
This is a helpful tool for diagnostic confirmation and may have the ability to aid in prognosis and prediction of clinical benefit from endocrine based therapies, including with CDK 4/6 inhibitors
We have many endocrine options now, and FES PET may identify patients who remain ER+ and thus potentially benefit from endocrine based therapy
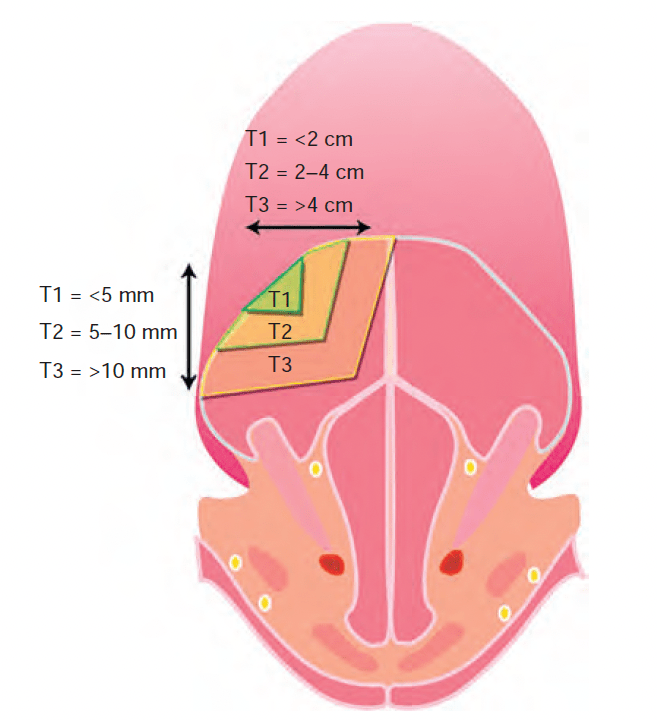
As published by the AJCC and UICC is widely accepted
In its most recent revision (eighth edition of the AJCC Staging Manual):
Depth of invasion (DOI):
Is added to the surface dimensions and local extent of the tumor:
As the required parameters for primary tumor staging in the oral cavity
Depth of invasion and surface dimensions are the parameters required for T staging of oral cancer
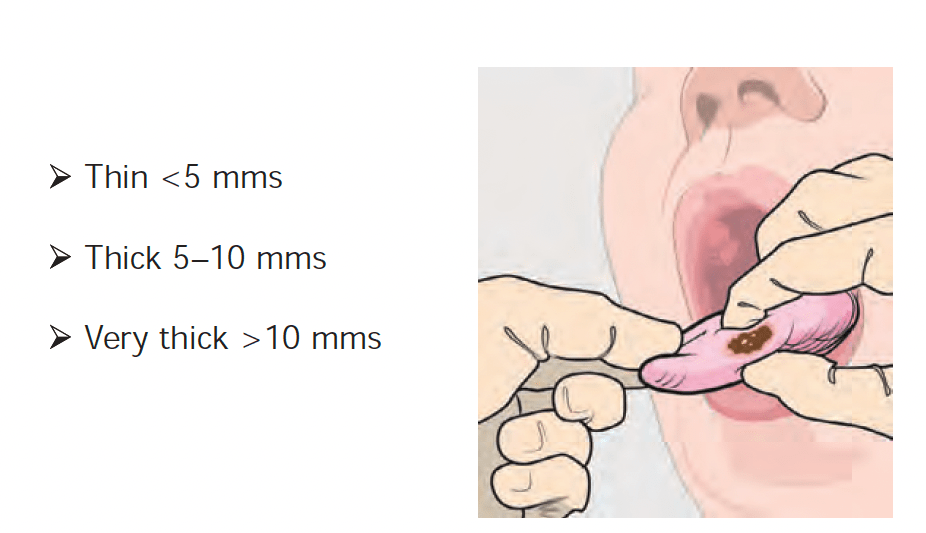
Accurate assessment of DOI by clinical examination is not possible:
However, the staging system stratifies DOI by 5 mm increments, and thus clinical estimates of DOI can be categorized into:
Thin (less than 5 mm)
Thick (5 to 10 mm)
Very thick (greater than 10 mm)
By palpation to assign clinical T stage
Primary tumors of the oral cavity are categorized as thin, thick, and very thick by palpation
The stage distribution of patients with squamous cell carcinoma of the oral cavity at the Memorial Sloan Kettering Cancer Center in New York is shown in the graph:
Stage distribution for squamous cell carcinoma of the oralcavity (MSKCC data 1985 to 2015)
With HER2 negative breast cancer and residual disease after undergoing neoadjuvant chemotherapy:
To standard postsurgical treatment and capecitabine or placebo
The primary end point:
Was disease-free survival (DFS)
Secondary end points included:
Overall survival (OS)
DFS was longer in the capecitabine group than in the control group (placebo):
74.1% vs. 67.6% of the patients were alive and free from recurrence or second cancer at 5 years
Among patients with triple-negative disease:
DFS was 69.8% in the capecitabine group versus 56.1% in the control group
OS rate was 78.8% versus 70.3%
There is no role for tamoxifen or anastrozole in triple negative breast cancer
Residual disease after completion of neoadjuvant chemotherapy:
Is associated with worse outcomes
References
1. Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Eng J Med. 2017;376(22):2147-2159.
2. Symmans WF, Wei C, Gould R, Yu X, Zhang Y, Liu M, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35(10):1049-1060.
The omission of adjuvant regional nodal irradiation did not appear to increase the risk for recurrence or death among patients with breast cancer whose disease converted from lymph node-positive to lymph node-negative after neoadjuvant chemotherapy, according to research presented at the 2023 San Antonio Breast Cancer Symposium
There is no standard of care in place for patients with breast cancer for whom neoadjuvant chemotherapy has eliminated lymph node involvement, the researchers explained
The researchers performed a phase 3 clinical trial of 1,641 patients with lymph-node positive, nonmetastatic breast cancer who were found to have no lymph node involvement after neoadjuvant chemotherapy and surgery
They randomly assigned patients to two different regimens:
One group was assigned to skip regional nodal irradiation after undergoing mastectomy or whole breast irradiation and breast-conserving surgery
The other group was assigned to continue with chest wall irradiation and regional nodal irradiation following mastectomy or whole-breast irradiation plus regional nodal irradiation and breast-conserving surgery
Median follow-up was 59.5 months, and patients were a median of 52 years old
Seventy-eight percent had experienced a complete breast pathological response
In the “no regional nodal irradiation group,” 91.8% of patients were invasive breast cancer-recurrence free at 5 years compared with 92.7% of those who did undergo regional nodal irradiation
In both groups, 93.4% of patients were reported to be distant-recurrence free at 5 years
Overall survival was 94% in patients who were assigned to skip regional nodal irradiation and 93.6% in those who did not skip the therapy, according to the researchers
The researchers are planning a longer-term follow-up to further examine their findings, and a 10-year analysis time point was reached this past year
There findings suggest that downstaging cancer-positive regional lymph nodes with neoadjuvant chemotherapy can allow some patients to skip adjuvant regional nodal irradiation without adversely affecting oncologic outcomes
Follow-up of patients for long-term outcomes continues
Reference:
Mamounas, E. Loco-regional irradiation in patients with biopsy-proven axillary node involvement at presentation who become pathologically node-negative after neoadjuvant chemotherapy: Primary outcomes of NRG Oncology/NSABP B-51/RTOG 1304. Abstract GS02-07. SABCS 2023
To determine the need and extent of mandible resection:
It is essential to understand the pathway by which oral cancers invade the mandible
Primary carcinomas of the lip, buccal mucosa, tongue, and floor of the mouth:
Extend along the surface mucosa and the submucosal soft tissues:
To approach the attached labial, buccal, or lingual gingiva
From this point:
The tumor does not extend directly through intact periosteum and cortical bone toward the cancellous part of the mandible:
Because the periosteum acts as a significant protective barrier
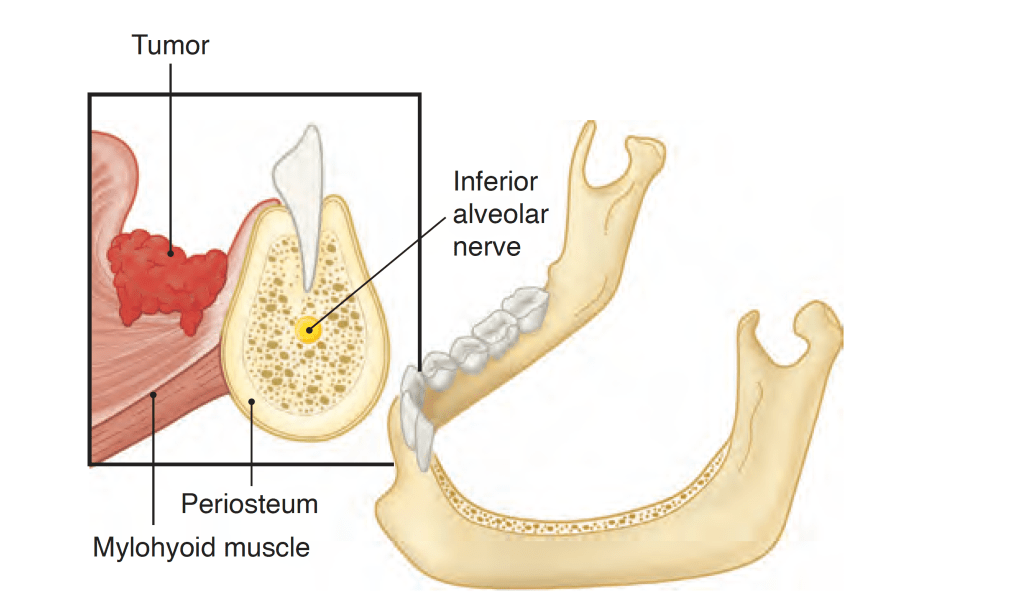
Instead:
The tumor advances from the attached gingiva toward the alveolus:
In patients with teeth, the tumor extends through the dental socket into the cancellous part of the bone and invades the mandible in that fashion (Figure)
Tumor invasion of the dentate mandible occurs through the dental socket to the cancellous bone and then to the alveolar canal
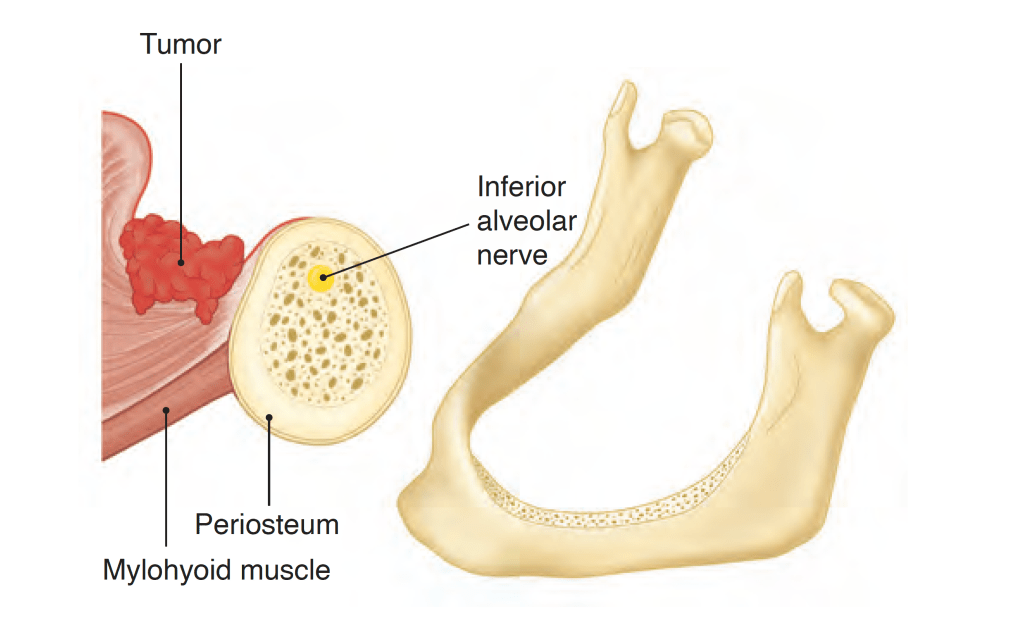
In edentulous patients:
The tumor extends up to the alveolar process and then infiltrates the dental pores in the alveolar ridge and extends to the cancellous part of the mandible (Figure)
Tumor invasion of the edentulous mandible occurs through the dental pores on the alveolar process to the cancellous bone and then to the alveolar canal.
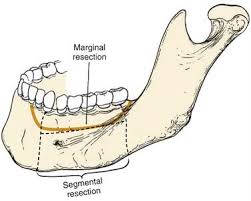
Thus even in patients with early invasion of the mandible:
A marginal mandibulectomy is feasible because the cortical part of the mandible inferior to the roots of the teeth:
Remains uninvolved and can be safely spared
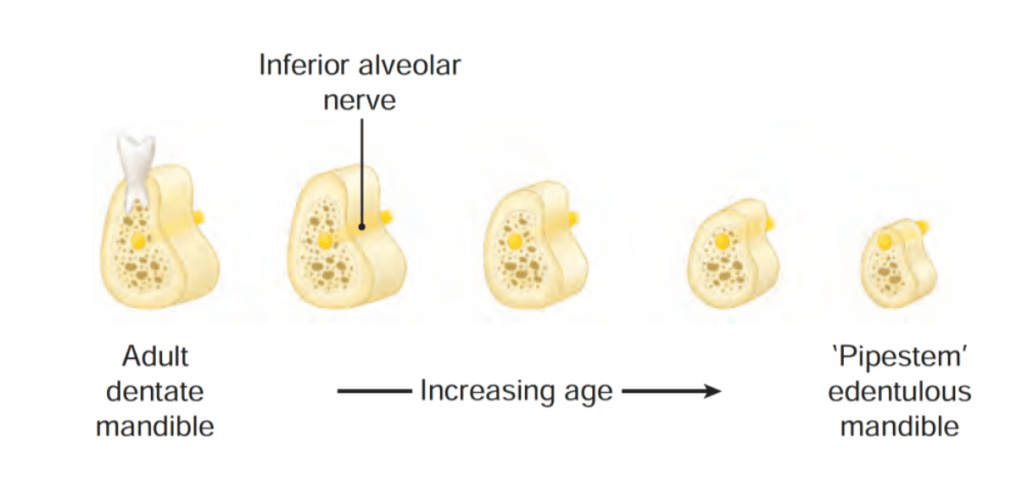
In edentulous patients, however, the feasibility of marginal mandibulectomy depends on the vertical height of the body of the mandible:
With aging, the alveolar process recedes and the mandibular canal comes closer to the surface of the alveolar process:
As shown in the Figure, the resorption of the alveolar process eventually leads to a “pipestem” mandible in elderly patients
Vertical height and location of the alveolar canal in dentate and edentulous mandibles.
The ability to perform a satisfactory marginal mandibulectomy in such patients is almost impossible:
Because the probability of iatrogenic fracture or postsurgical spontaneous fracture of the remaining portion of the mandible is very high:
Similarly, in patients who have received previous radiotherapy, a marginal mandibulectomy should be performed with extreme caution:
The probability of pathological fracture at the site of the marginal mandibulectomy in such patients is very high
When the tumor extends to involve the cancellous part of the mandible:
A segmental mandibulectomy must be performed
A segmental mandibulectomy also may be required in patients with massive primary tumors with significant soft tissue disease in the proximity of the mandible
Rodrigo Arrangoiz MS, MD, FACS, FSSO is an Assistant Professor at the Columbia University Division of Surgical Oncology at Mount Sinai Medical Center
He is first author on some publications on oral cavity cancer:
Oral Tongue Cancer: Literature Review and Current Management