My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Provide both structural and functional information and can be very useful in determining the etiology of biochemical hyperthyroidism:
In contrast, thyroidal nuclear imaging is not recommended in the evaluation of a patient with hypothyroidism
For nuclear imaging, scans using radioactive iodine isotopes are most preferred:
Because these directly reflect the active accumulation (trapping) of iodine by the thyroid follicular cell and covalent attachment (organification) of iodine to thyroglobulin
The preferred radionuclide for diagnostic nonthyroid cancer imaging:
Is 123I, because this isotope emits only gamma rays that pass through tissue without significant cellular damage:
In contrast, 131I emits both gamma rays for imaging, as well as damaging beta particles:
So it can be used for the treatment of hyperthyroidism and thyroid cancer:
To destroy iodine-avid thyroid tissue
For diagnostic imaging:
123I is administered orally:
With the measurement of iodine uptake and gamma scintigraphy images:
Obtained 4 hours and / or 24 hours later
Measured thyroidal uptake depends on the activity of NIS and overall iodine status as determined by the amount of circulating nonradioactive iodine:
When there is an excess of nonradioactive iodine:
The measured radioactive iodine uptake is reduced due to the competition between radioactive and nonradioactive iodine uptake by the thyroid follicular cells:
Sources of excess nonradioactive iodine include kelp, seaweed, seafood, iodine-rich medications and agents (amiodarone, saturated solution of potassium iodide [SSKI], Lugol’s solution, povidone iodine, tincture of iodine, iodoform gauze), and radiographic contrast media used commonly in computed tomography (CT) scans and gallbladder studies
An alternate radionuclide is technetium99m pertechnetate (99mTc):
Which is administered intravenously
Images are obtained much more rapidly than 123I:
Usually on the order of 30 to 60 minutes after the administration of the radionuclide tracer
Although 99mTc will be trapped by the thyroid follicular cells:
There is no iodine moiety for attachment to thyroglobulin, and therefore does not as accurately mimic the thyroidal uptake of iodine as radioiodine nuclides:
Thus 123I thyroid scans have 5% to 8% fewer false negative results than 99mTc scans:
However, because 99mTc scans are easier, faster, more readily available and less expensive to perform, they have largely replaced 123I scans at some institutions
Studies of direct comparison of radioiodine and 99mTc thyroid scans have been highly concordant in patients without nodules and in those with cold nodules:
One study reported that of 273 patients with thyroid nodules, only two had increased uptake with pertechnetate and no uptake with radioiodine:
However, if the results of the 99mTc scan are not in agreement with the clinical picture, an 123I scan should be performed
Although nuclear scans are useful in the differential diagnosis of biochemical hyperthyroidism:
Other radiologic modalities (e.g., ultrasonography, CT, and magnetic resonance imaging [MRI]) provide information regarding structural anatomy of the thyroid and provide no functional data
The primary role of thyroid ultrasound is in the initial evaluation of thyroid nodules:
As recommended by the American Thyroid Association and the American Association of Clinical Endocrinologists
Although thyroid ultrasound does not have a role in the initial evaluation of biochemical thyroid dysfunction:
It may demonstrate changes that are consistent but are not necessarily diagnostic of chronic lymphocytic thyroiditis, subacute granulomatous thyroiditis, and postpartum thyroiditis
Some individuals with subclinical hypothyroidism and sonographic features suggestive of chronic thyroiditis:
Are at significant risk for developing overt hypothyroidism requiring thyroid hormone replacement therapy
Before the implementation of routine screening mammography:
Most patients with DCIS presented with a:
Palpable mass
Nipple thickening
Nipple discharge
Paget disease of the nipple
Occasionally, DCIS was an incidental finding:
In an otherwise benign breast biopsy specimen
In patients with palpable lesions:
Up to 25% demonstrated foci of invasive disease
Now that screening mammography is more prevalent:
The incidence of DCIS has increased dramatically and currently comprises:
Approximately 20% of all breast cancers
Most cases of DCIS are diagnosed:
When the tumor is still clinically occult
Patients with abnormalities detected by screening mammography:
Should always undergo diagnostic imaging of the contralateral breast:
Because 0.5% to 3.0% of patients have:
Synchronous occult abnormalities or cancers in the contralateral breast
Mammographic images should be compared with previous images, if available, to establish interval changes
Mammographic features:
On a mammogram, DCIS can present as:
Microcalcifications:
80% to 90% of mammographic manifestations
A soft-tissue density
Both
Microcalcifications:
Are the most common (80% to 90%) mammographic manifestation of DCIS:
Which, in turn, accounts for 80% of all breast carcinomas:
Presenting with calcifications
Any interval change from a previous mammogram:
Is associated with malignancy in 15% to 20% of cases:
Most often indicates in situ disease
Holland et al. (1990):
Described two different classes of microcalcifications:
Linear branching-type microcalcifications:
Which are more often associated with:
High–nuclear-grade lesions
Comedo-type lesions
Fine, granular calcifications:
Which are primarily associated with:
Micropapillary or cribriform lesions:
Of lower nuclear grade and that do not show necrosis
Although the morphology of microcalcifications:
Suggests the architectural type of DCIS:
It is not always reliable
Holland et al:
Also demonstrated that the mammographic findings:
Significantly underestimated the pathologic extent of disease:
Particularly in cases of:
Micropapillary DCIS:
Lesions were more than 2 cm larger by histologic examination than by mammographic estimation:
In 44% of cases of micropapillary lesions, compared with only 12% of cases of the pure comedo subtype
However, when magnification views were used in diagnostic mammographic examination:
The extent of disease was underestimated in only 14% of cases of micropapillary tumors
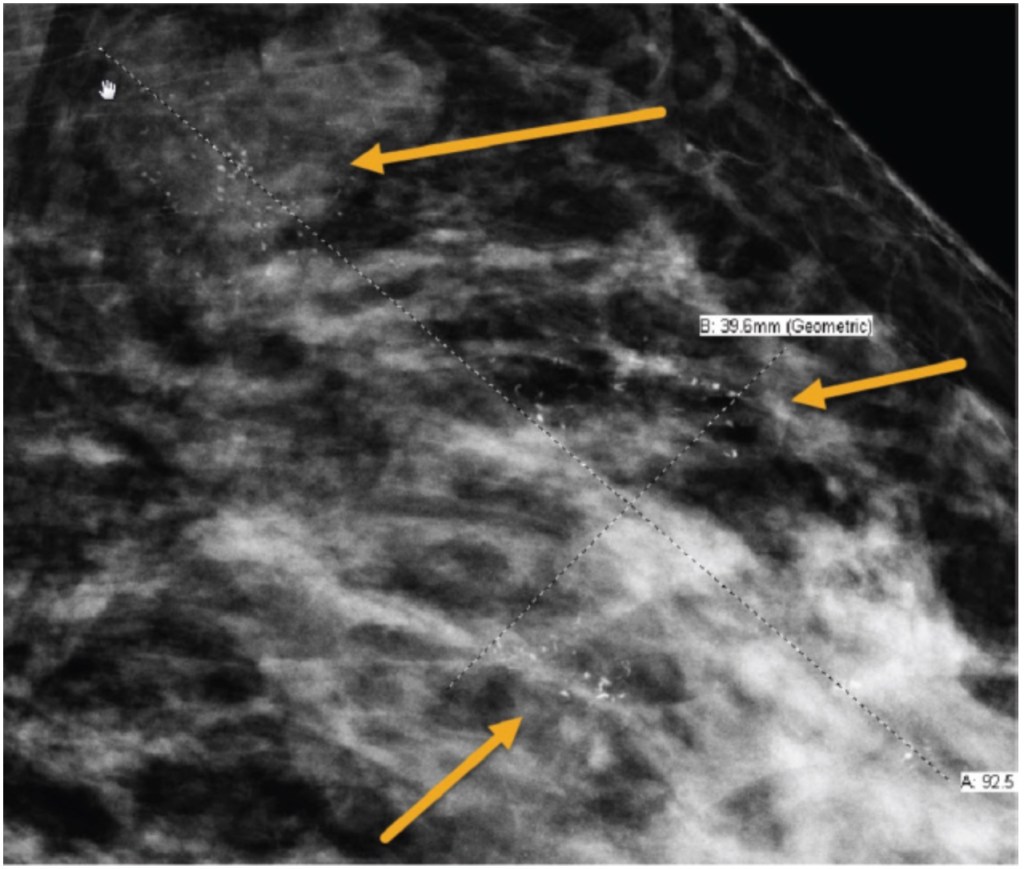
Hence, magnification views increase the image resolution and are better able to delineate the shape, number, and extent of microcalcifications when compared with mammography alone:
And should be used routinely in the evaluation of suspicious mammographic findings
Calcifications seen on diagnostic mammography associated with ductal carcinoma in situ (DCIS). Magnification view is shown to demonstrate calcifications spanning approximately 9 cm.
Maintaining genomic stability and regulating cell cycle checkpoints
Carriers of a TP53 pathogenic variant:
Would be expected to be unable to repair tissue damage from DNA-damaging radiotherapy and be at risk for significant radiotherapy-associated sequelae
Outcomes reported in published case reports:
Support this recommendation against radiotherapy in women with breast cancer who are carriers of a TP53 pathogenic variants:
Due to increased risk of radiation-induced secondary malignancies
Mutations in TP53 are considered:
An absolute contraindication of radiotherapy:
Except in those with a significantly high risk of locoregional recurrence
Mastectomy is the recommended therapeutic surgical option
The radiotherapy-induced toxicity spectrum in patients with breast cancer carrying ATM pathogenic variants is controversial:
Seven studies identified in a systematic review addressed radiotherapy after breast-conserving surgery among women with breast cancer who harbor ATM pathogenic variants:
Meyer et al found no significant differences in local relapse-free survival in a cohort of 138 patients with early stage breast cancer treated with breast-conserving surgery, followed by radiotherapy, of whom 20 were found to carry either an ATM truncating or missense variant:
They concluded that the results do not support the hypothesis that patients with breast cancer carrying a sequence variant in the ATM gene differentially benefit from postoperative radiotherapy
According to the ASCO-ASTRO-SSO Consensus recommendations for carriers of BRCA 1/2 and other germline pathogenic variants,:
Women with breast cancer may safely be offered radiotherapy when clinically indicated
Data on toxicity rates comparing carriers of ATM pathogenic variants and noncarriers:
Do not favor avoiding radiotherapy:
Potential absolute risks do not appear to be significant:
However, more research is needed
A discussion with ATM carriers interested in breast-conserving therapy is encouraged
There is no evidence of increased toxicity or contralateral breast cancer events from radiation exposure in BRCA 1/2, CHEK2, CDH1 carriers
References:
Trombetta MG, Dragun A, Mayr NA, Pierce LJ. ASTRO Radiation Therapy Summary of the ASCO-ASTRO-SSO Guideline on Management of Hereditary Breast Cancer. PractRadiat Oncol. 2020;10:235-242.
Lazzari G, Buono G, Zannino B, Silvano G. Breast cancer adjuvant radiotherapy in BRCA1/2, TP53, ATM genes mutations: Are there solved issues? Breast Cancer (Dove Med Press). 2021;13:299-310.
Ferrarini A, Auteri-Kaczmarek A, Pica A, et al. Early occurrence of lung adenocarcinoma and breast cancer after radiotherapy of a chest wall sarcoma in a patient with a de novo germline mutation in TP53. Fam Cancer. 2011;10:187-192.
Heymann S, Delaloge S, Rahal A, et al. Radio-induced malignancies after breast cancer postoperative radiotherapy in patients with Li- Fraumeni syndrome. Radiat Oncol. 2010;5:104.
Meyer A, John E, Dörk T, Sohn C, Karstens JH, Bremer M. Breast cancer in female carriers of ATM gene alterations: outcome of adjuvant radiotherapy. Radiother Oncol. 2004;72: 319-323.
Is a large glycoprotein that is stored as colloid:
The primary storage form of thyroid hormone, in the lumen of thyroid follicles
It is continuously secreted into circulation from the thyroid gland:
Thereby reflecting the mass of normal and malignant thyroid tissue
Higher serum concentrations result from:
TSH stimulation and / or injury of thyroid tissue:
However, for the individual with an intact thyroid gland:
Its clinical value for evaluating thyroid dysfunction or goiter is limited in the era of modern serum thyroid function testing and imaging
However, the demonstration of a suppressed serum Tg level in such a patient can be useful in differentiating factitious thyrotoxicosis (from exogenous thyroid hormone ingestion) from excessive endogenous thyroid hormone release of any etiology:
In this situation, when thyrotoxicosis is due to ingestion of exogenous thyroid hormone:
Normal thyroid hormone production is suppressed and serum Tg levels are decreased
In contrast, if excess thyroid hormone is produced from the thyroid:
Serum Tg levels are elevated
In current clinical practice:
The primary use of serum Tg concentrations is as a tumor marker in patients with differentiated thyroid cancer:
That is obtained to detect persistent and / or recurrent disease after a total thyroidectomy and radioactive iodine (131I) ablation
Most Tg assays have only first-generation functional sensitivity between 0.5 and 1 ng/mL:
But the second generation Tg assays are rapidly becoming the standard and have an improved functional sensitivity of 0.05 to 0.1 ng/mL
The Tg assay can be made more sensitive to detect persistent or recurrent tumor:
After stimulation by TSH:
Either endogenously by withholding thyroxine treatment in an athyreotic patient or with administration of recombinant human TSH (rhTSH):
The latter of which results in an approximate tenfold increase in basal serum Tg concentrations
Detection of persistent and / or recurrent disease in thyroid cancer depends on the performance of Tg immunometric assays:
Which currently have suboptimal sensitivity and high interassay variability
Virtually all immunometric methods:
Will report an undetectable Tg level in euthyroid Tg Ab positive controls:
Approximately 25% of patients with differentiated thyroid cancer have a positive serum TgAb titer:
Thus when a suspicious lymph node or neck mass is detected in an individual who has undergone a total thyroidectomy:
An unmeasurable basal or rhTSH-stimulated Tg in the setting of a positive serum TgAb level:
Does not necessarily exclude thyroid cancer recurrence
It is reasonable in this relatively uncommon situation to measure Tg instead by Tg Ab-resistant radioimmunoassay (RIA) or liquid chromatography tandem mass spectrometry:
Which are available at some specialty endocrine laboratories.
When the serum Tg Ab titer is positive:
It may also be used as a surrogate marker of tumor persistence / recurrence
In one study, a > 50% decrease of Tg Ab levels within the first year after a total thyroidectomy:
Was associated with the absence of tumor recurrence / persistence in all patients studied
Tumor recurrence / persistence was present in 37% of patients who had any rise of serum Tg Ab within the same period
Thus thyroid cancer patients with rising Tg antibody levels:
Are at high risk for disease persistence / recurrence and should be evaluated promptly
In addition, the sensitivities and absolute values reported by different methods of measuring Tg and TgAb are highly variable:
It is essential to always use the same Tg and TgAb method when following an individual over time for tumor persistence/recurrence
Finally, the presence of interfering heterophile antibodies (antibodies against the animal-derived antibodies used in the immunometric assay):
May rarely result in abnormally high or low serum Tg levels
The most common interfering antibodies are HAMAs:
Clinically, this should be suspected when an elevated serum Tg level is inappropriate for the clinical situation and does not increase with rhTSH stimulation
When heterophile antibody is suspected, the clinician should repeat the test using a commercially available heterophile-blocking tube (HBT) or measure Tg with an RIA assay
Can be estimated using a variety of indirect (analog, immunometric, and two-step labeled hormone assays) or direct methods (equilibrium dialysis, ultrafiltration), and are the most commonly used measurements of circulating thyroid hormone levels
Generally, most laboratories estimate free T4 by either the analog immunoassay or a calculated FT4I corrected to thyroid hormone binding capacity:
The former is readily available and provides quick results; it does not directly measure the free T4 concentration but is a reliable estimate of FT4 levels in most patients, based on one-step, two-step, or labeled antibody approaches
This type of free T4 estimate is especially sensitive to abnormal serum albumin levels and should not be used with conditions such as:
Familial dysalbuminemic hyperthyroxinemia, pregnancy, or severe nonthyroidal illness:
For example, it is common to have a free T4 lower than the reference range in a euthyroid pregnant woman:
Due to the high estrogen state of pregnancy greatly increasing serum TBG concentrations, thus resulting in inaccurate FT4 measurements
The serum FT4I measurement is a calculated value that is the product of the total T4 concentrations and a correction factor related to the number of available thyroid hormone binding sites:
This correction factor may be called:
A thyroid hormone binding ratio (THBR), T3 resin uptake (T3RU), or T3 uptake (T3U)
The T3RU is inversely related to the free thyroid hormone binding sites but is now used in only a few laboratories
Free T4 by equilibrium dialysis:
Is the gold standard and measures the 0.03% of T4 that is biologically active and unbound to protein
This assay is available only at reference laboratories and is useful to directly determine free T4 levels when other testing does not provide a clear result
Although a TSH-first testing algorithm is suffcient for general screening:
Both FT4 and TSH assays are needed for:
Diagnosing subclinical thyroid dysfunction, central hypothyroidism, and in the assessment of elderly and hospitalized patients, as well as for accurate assessment of treatment effects
Guidelines from multiple thyroid and endocrine societies:
Have also endorsed a TSH-first strategy in most clinical scenarios with FT4 testing when clinically indicated or TSH is found to be abnormal
Work by Henze et al. goes even further suggesting that a TSH-first strategy can be further perfected by:
Widening the TSH reference range from 0.4 to 4.0 mIU/L to 0.2–6.0 mIU/L with minimal impact on case detection
They found that only 4.2% of TSH values between 0.2 mIU/L and 0.4 mIU/L would not have led to detection of a high FT4 and equally, only 2.5% of TSH values between 4.0 mIU/L and 6.0 mIU/L were associated with low FT4 level
It is likely that this small additional group of patients outside the wider range with abnormal FT4 is clinically unimportant in most cases
Serum total T4 (TT4) and total T3 (TT3) concentrations:
Are a measure of both the bound and free hormone levels of these two hormones
TT4 or TT3 levels should be interpreted in the context of the clinical situation:
Because many clinical conditions and medications alter the concentrations of thyroid hormone binding proteins and / or compete with the binding of thyroid hormones to the binding proteins:
As such, measured TT4 and TT3 levels may be affected, even though the bioactive free levels and thus, the thyroidal status, remain unchanged
T3 is the active thyroid hormone:
It is primarily useful in the diagnosis and management of patients with hyperthyroidism
It occasionally can be used to differentiate stimulation induced thyrotoxicosis / Graves’ disease (TT3 / TT4 ratio > 20) from destruction induced thyrotoxicosis / subacute thyroiditis (TT3 / TT4 ratio < 12):
This assessment can be further augmented when TSH is considered as serum levels of TSH are generally suppressed in most untreated Graves’ patients, whereas they usually were not completely suppressed in patients with painless thyroiditis or subacute thyroiditis
Measurement of serum TT3 is not usually helpful if hypothyroidism is suspected:
Because the activity of 5’deiodinas type 2 enzyme (Dio2):
Which converts T4 to the biologically active T3:
Increases while serum T4 falls:
Thus maintaining normal T3 levels until the overall thyroid hormone levels are very low
rT3, which may be elevated during nonthyroidal illness:
Is not biologically active:
As such, the utility of measuring it and other forms of inactive iodothyronine are limited during the evaluation of thyroid status
Finally, the human anti-mouse antibodies (HAMAs) that interfere with TSH testing:
Can also interfere with the thyroid hormone assays
HAMA positivity:
May result in artificially elevated or reduced TT4, TT3, FT4, and FT3 levels
Patients who have received therapeutic monoclonal antibody treatment may be at increased risk of develop interfering positive HAMA titers
After stimulation by thyrotropin-releasing hormone (TRH)
Thyrotropin-releasing hormone (TRH):
Is a modified three-amino acid peptide:
Produced by neurons of the paraventricular nucleus:
In the hypothalamus
TRH signaling from the hypothalamus:
Is achieved through a portal venous system:
Located in the infundibulum of the pituitary stalk:
Which allows communication to the pituitary gland
Both TRH and TSH gene expression:
Are decreased by excess thyroid hormone levels:
Via negative feedback mechanisms (Figure)
Both the hypothalamus and pituitary:
Have high levels of 5′deiodinases Type 2 enzyme (Dio2):
Catalyzes the removal of the 5′ iodine from the outer ring of thyroxine (T4):
To create the metabolically active triiodothyronine (T3)
So T4 levels are the primary feedback:
T4 is converted locally to T3:
Which suppresses TRH and TSH gene expression
Schematic Representation of Control of Thyroid-Stimulating Hormone (TSH) Secretion by the Thyrotroph Cells in the Anterior Pituitary Gland. High concentrations of T3 suppress TSH release, and low concentrations enhance the expression of TSH. Thyrotropin-releasing hormone (TRH) also stimulates TSH release, and its absence results in failure of the thyrotroph to release TSH, resulting in hypothyroidism. TRH is secreted by neurons in the paraventricular nuclei in the hypothalamus and reaches the anterior pituitary via the hypothalamic hypophyseal portal venous system. TSH travels through the circulatory system to stimulate the thyroid and to produce thyroid hormones T4 and T3. By negative feedback inhibition, the circulating thyroid hormones suppress the production and excretion of TRH and TSH to bring the system back into equilibrium to maintain tight control over circulating thyroid hormone levels.
Pituitary TSH is secreted in a pulsatile manner:
Higher levels at night and lower levels during the day:
The inverse of the cortisol cycle
Although pulse frequency is increased nocturnally to result in a diurnal variation of TSH concentrations:
Levels remain within the reference range
Generally, laboratory testing of serum TSH concentrations during daylight hours:
Is not substantially affected by the diurnal variation of TSH secretion:
But results outside the reference range may occur in euthyroid individuals when drawn outside of these times
TSH stimulates the synthesis and release of thyroid hormone from the thyroid gland:
TSH production from the anterior pituitary gland is inverse log-linearly regulated by serum thyroid hormone concentrations:
When there are small decreases in thyroid hormone levels in circulation:
Large increases in serum TSH stimulate thyroid hormone production by the thyroid gland
This negative feedback loop between serum TSH and the serum-free thyroid hormones:
Is able to maintain circulating thyroid levels within a tight range
Serum TSH is the preferred screening test:
In the evaluation of thyroid function in the ambulatory patient:
Regardless of whether the patient is taking thyroid hormone replacement medication
For the healthy patient in an ambulatory setting:
The diagnosis of hypothyroidism or hyperthyroidism:
May be determined with approximately 98% sensitivity and 92% specificity using serum TSH
In addition, TSH has a narrow intraindividual variability of ± 0.5 mIU/L:
Such that thyroid dysfunction may be present if there are significant changes in TSH values over time in an individual, even if they remain within the reference range
In certain situations, however, such as known or suspected pituitary or hypothalamic dysfunction, recent hyperthyroidism, critical illness, starvation, use of certain medications (dopamine or high-dose glucocorticoids), interference with serum thyroid autoantibodies, and thyroid hormone resistance syndromes:
The TSH level is inaccurate for the thyroidal status and should not be used in isolation to determine thyroid function
In addition, the presence of interfering heterophile antibodies (antibodies against the animal-derived antibodies used in the immunometric assay):
May rarely cause abnormally high or low TSH levels:
These conditions should be suspected when the pattern of the TSH levels does not correlate to the clinical presentation or when the peripheral serum hormone levels do not change as expected with elevated or suppressed serum TSH concentrations
Serum TSH assays:
Have evolved considerably since measurements were first described in the 1960s:
When the functional sensitivity was between 1 and 2 mIU/L
The commonly used second-generation TSH assays have an improved functional lower limit of 0.10 to 0.20 mIU/L:
Which is able to differentiate between euthyroid and hyperthyroid states but does not indicate the degree of hyperthyroidism
In contrast, a third-generation TSH assay can detect levels as low as 0.01 to 0.02 mIU/L:
This is helpful when there is a challenging pattern of serum thyroid function tests that include an extremely suppressed TSH
In the rare instance they are needed, fourth-generation immunochemiluminometric assays are capable of detecting TSH levels in the range of 0.01 to 0.001 mIU/L
A serum TSH level measured in an ambulatory population that lies within the reference range:
Is generally considered evidence of normal thyroid function and requires no additional testing
Reference ranges for serum TSH can vary slightly from one commercial laboratory to another:
It should be noted that normal ranges, which are based on the epidemiologic distribution of serum TSH concentrations in healthy populations:
From which serum thyroid autoantibody positivity and iodine status (both of which can affect TSH), may be variable
If an abnormal screening TSH result is encountered:
The circulating thyroid hormone levels should be assessed
The specific pattern of tests will allow further insight into whether clinical thyroid dysfunction should be suspected
Evaluation and Management of Hypothyroidism in Individuals With Corresponding Signs and Symptoms.Evaluation and Management of Hyperthyroidism in Individuals with Corresponding Signs and Symptoms.
Such as thyroid peroxidase (TPO Ab, previously known as antimicrosomal antibodies), thyroglobulin (Tg Ab), and the TSH receptor (TSHR Ab):
Are formed against thyroid proteins
The presence of TPOab is commonly associated with patients with hypothyroidism:
But can be present in normal individuals who do not display any obvious symptoms of clinical thyroid disease
TPOabs are present in approximately 10% of normal individuals:
While it was detected in almost 100% of samples of patients with autoimmune hypothyroidism
More than 90% of patients with autoimmune thyroid disease (Hashimoto’s thyroiditis and Graves’ disease):
Will have elevated titers of second-generation assays for TPO Ab and Tg Ab
When biochemical hypothyroidism is found:
Measuring TPO Ab can be helpful:
Because its result can provide additional information regarding the etiology of the thyroid dysfunction
Median serum TSH concentrations are increased within the reference range:
Among those with serum TPO Ab and Tg Ab positivity:
Compared with those without TPO Ab titers, and are a predictor for the development of biochemical thyroid dysfunction in euthyroid individuals
In individuals with subclinical hypothyroidism:
Bothserum TPO Ab positivity and sonographic characteristicssuggestive of chronic thyroiditis:
Are associated with an increased likelihood of progression to overt hypothyroidism
The TSHR Abs are a group of immunoglobulins:
That produce Graves’ hyperthyroidism
Measured as:
TSH receptor binding, TRAB (TSH-receptor antibody) or in a functional bioassay, thyroid stimulating immunoglobulin (TSI)
TSH receptor antibodies:
Are being increasingly recommended for monitoring activity of disease to assess response to therapy in Graves’ patients
Less commonly, TSH receptor binding antibodies:
Can block the TSH receptor and produce hypothyroidism
In the setting of normal serum thyroid function:
Thyroid antibodies should generally not be measured except in special circumstances:
Such as a history of hyperthyroidism during pregnancy or recurrent miscarriages:
In these situations, both the stimulating and inhibiting TSHR Abs can cross the placenta to affect fetal thyroid function and potentially induce fetal goiter
Although serum thyroid antibody positivity during pregnancy:
Is associated with a higher risk of postpartum subacute thyroiditis:
Antibody screening in pregnant women is not currently recommended
The evaluation of a chronically ill or hospitalized patient with abnormal serum thyroid function tests:
Can often be challenging
Nonthyroidal illness is not considered a primary thyroid disorder:
Its pathophysiology is not completely understood:
Although it is known that the elevation of cytokines and hypoxia plays a significant role
It is generally recommended to avoid measuring serum thyroid function tests during acute illness:
Unless thyroid dysfunction is thought to be a significant contributor to the illness
Severe nonthyroidal illness:
Is accompanied by significant alterations in thyroid physiology
Due to the decreased availability in all of the thyroid binding proteins (thyroxine bindings globulin, transthyretin, albumin):
Serum total T4 and total T3 levels are reduced:
Whereas free levels are usually normal or slightly low (Figure)
Total T3 levels are further decreased:
Due to reduced Dio1 activity:
Which converts T4 to T3
A relatively greater amount of T4 is metabolized to the inactive metabolite:
Reverse T3 (rT3):
By Dio3
Although measurement of rT3 does not reliably distinguish nonthyroidal illness from primary hypothyroidism
The degree of serum rT3 elevation, depressed T3 / rT3 ratio, and decreased FT3 and FT4 concentrations:
Have been associated with higher mortality among patients in the intensive care unit (ICU):
Treatment with T4 or T3, however, does not consistently improve outcome
Whether other T4 metabolites, including 3,3′-diiodothyronine (3,3′-T2); 3,5-diiodothyronine (3,5-T2); and 3-iodothyronamine (3-T1AM):
Have functional roles in nonthyroidal illness remains unclear
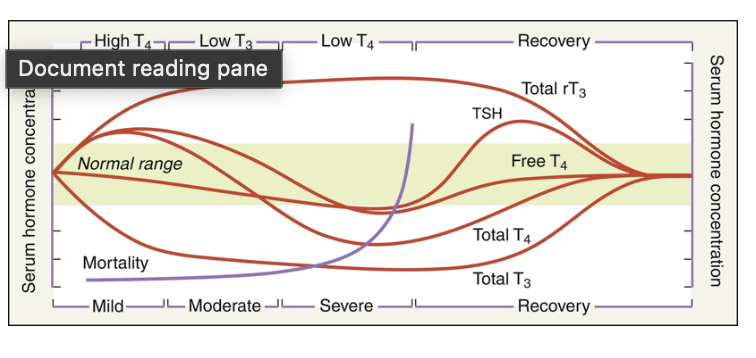
Alternations in Serum Thyroid Hormone Concentrations During Acute Nonthyroidal Illness and Recovery. The degree of change in hormone concentrations relates to the severity and duration of the illness. Thyroid-stimulating hormone (TSH) may also be suppressed during severe illness and transiently rise moderately above the reference range before returning to normal with recovery. Mortality correlates inversely with the degree of reduction in total T4 concentration. (From Farwell AF. Sick euthyroid syndrome in the intensive care unit. In: Irwin RS, Rippe JM, eds. Intensive Care Medicine. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2003.)
It is important that the diagnosis of primary thyroid dysfunction:
Is not established during severe illness based solely on an abnormal serum TSH
In nonthyroidal illness:
Serum TSH concentrations may be low, normal, or high:
Due to the TSH-lowering effects of commonly used medications (glucocorticoids, ipodate, amiodarone, dopamine) in patients managed for a nonthyroidal illness or from a reversible form of acquired central hypothyroidism in severe nonthyroidal illness
During the recovery phase of nonthyroidal illness:
The TSH may briefly rise above the upper reference range, as suppression of TSH lessens, before it normalizes
When possible, thyroid evaluation after recovery from an acute illness is recommended in patients suspected of having intrinsic thyroid disease
Mammography relies on the presence of calcifications for the detection of DCIS:
Thus, lesions without calcifications are generally occult on mammography
Extensive DCIS:
Can present as a palpable mass
Nipple discharge:
Can also be a sign of either DCIS or invasive breast cancer
Paget disease:
Is a rare presentation:
Occurring in only 1% to 4% of women with breast cancer
It is characterized histologically by:
Intraepithelial tumor cells
It presents as a chronic ulceration or eczema of the nipple:
That can involve the surrounding areolar skin
It may be associated with invasion but, in the absence of invasion:
Is treated as DCIS
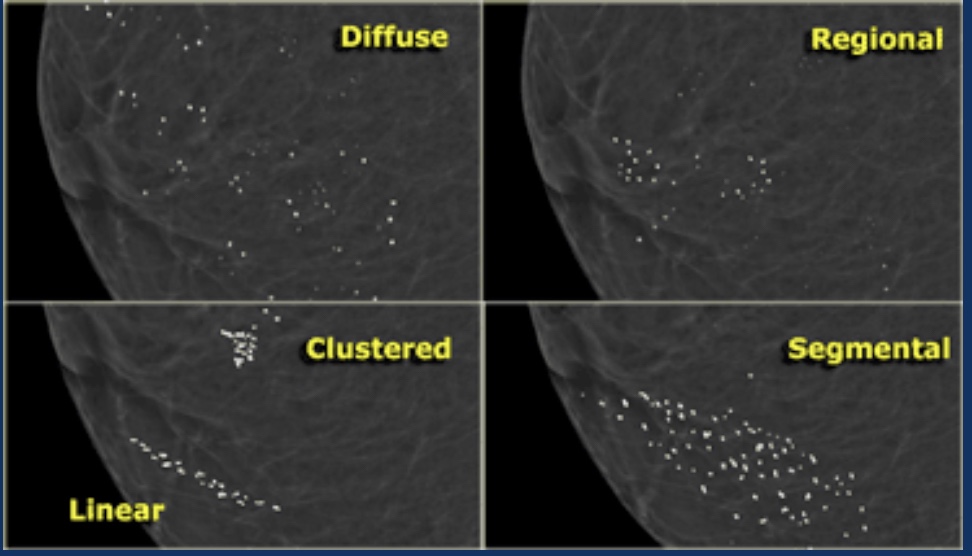
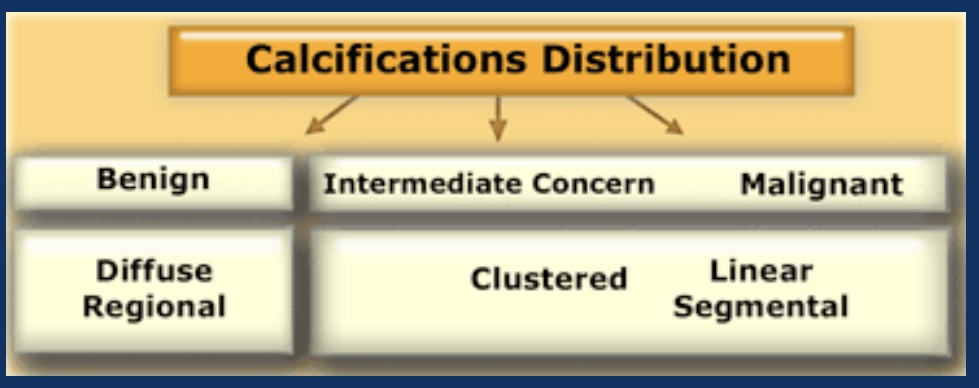
Morphology The form of the calcifications is the most important factor in the differentiation between benign and malignant. If calcifications cannot be readily identified as typically benign or as ‘high probability of malignancy’, they are termed of ‘intermediate concern or suspicious’. If a specific etiology cannot be given, a description of the calcifications should include their morphology and distribution using the descriptions given in the BI-RADS atlas.Distribution In the BI-RADS atlas the following descriptions are given for the distribution of calcifications: Diffuse or Scattered: diffuse calcifications may be scattered calcifications or multiple similar appearing clusters of calcifications throughout the whole breast. Regional: scattered in a larger volume (> 2 cc) of breast tissue and not in the expected ductal distribution. Clustered : at least 5 calcifications occupy a small volume of tissue. Linear: calcifications arrayed in a line, which suggests deposits in a duct. Segmental: calcium deposits in ducts and branches of a segment or lobe.Diffuse or scattered distribution is typically seen in benign entities. Even when clusters of calcifications are scattered throughout the breast, this favors a benign entity. Regional distribution according to the BI-RADS atlas would favor a non-ductal distribution (i.e. benignity)
Segmental distribution would favor a ductal distribution (i.e. malignancy). Sometimes this differentiation can be made, but in many cases the differentiation between ‘regional’ and ‘segmental’ is problematic, because it is not clear on a mammogram or MRI where the bounderies of a segment (or a lobe) exactly are.
Clustered calcifications are both seen in benign and malignant disease and are of intermediate concern. When clusters are scattered througout the breast, this favors a benign entity. A single cluster of calcification favors a malignant entity. Linear distribution is typically seen when DCIS fills the entire duct and its branches with calcifications