My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Anita K. Lam et al., Hong Kong cohort published in Cancer, 2005
Design:
Retrospective cohort of patients with thyroid carcinoma managed postoperatively:
From 2000 to 2003
Population:
Patients who underwent total thyroidectomy, categorized by RAI administration (yes / no) and lymph node metastasis characteristics
Primary Outcome:
Lymph node (regional) recurrence-free survival
Key Findings
RAI vs No‑RAI:
RAI-treated patients with lymph node metastases (N1) had significantly lower rates of regional lymph node recurrence compared to those managed without RAI
Influencing Factors:
Higher node burden (N1b vs N1a) and presence of microscopic extrathyroidal extension increased recurrence risk
Multivariate Analysis:
RAI independently predicted improved lymph node recurrence-free survival, even after adjusting for patient age, number of involved nodes, and ETE
Clinical Implications for Expert Surgeons:
Strengthens rationale for recommending RAI in patients with clinical / pathologic nodal metastases, particularly those with multiple nodes or N1b disease:
Supports adjuvant RAI as an effective tool to reduce surgical re-treatment for nodal recurrence
Highlights the importance of comprehensive nodal assessment in postoperative planning to determine RAI need
Encourages a risk-adapted approach:
For example, reserving RAI for patients with ≥ 1 cm nodal involvement or aggressive features
Summary:
Lam AK and colleagues provide more evidence supporting the benefit of RAI in reducing regional lymph node recurrence in node-positive thyroid cancer patients, particularly those with more extensive nodal disease
This data reinforces a targeted use of RAI in intermediate-risk cohorts to optimize outcomes
Reference:
Lam AK, et al. RAI impact on lymph node recurrence: Hong Kong cohort study. Cancer. 2005;103(5):920–9. Summary for expert thyroid surgeons
Trabajo realizado por Rodrigo Arrangoiz MS, MD, FACS y el equipo de Sociedad Quirúrgica S.C. que se presento en Septiembre del 2018 en el 6th World Congress of the International Federation of Head and Neck Oncology Societies llevado acabo en Buenos Aires, Argentina.
Rodrigo Arrangoiz is a board-certified surgical oncologist who subspecializes in breast cancer and head and neck cancer. Dr. Arrangoiz earned his medical degree at the Anahuac University Medical School in Mexico City, Mexico and graduated Suma Cum Laude. He completed his internship and residency in general surgery at Michigan State University, where he was named chief resident during his fifth year of residency. Dr. Arrangoiz also completed a complex surgical oncology, head and neck fellowship at the Fox Chase Cancer Center in Philadelphia and at the same time he undertook a master’s in science (Clinical Research for Health Care Professionals) at Drexel University in Philadelphia. Dr. Arrangoiz also participated in a two-year global online fellowship in head and neck surgery and oncology through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center.
Dr. Arrangoiz has participated in multiple courses and academic congresses as a lecturer and guest professor and has also participated in several publications on topics related to his specialty that include oral cavity cancer, hyperparathyroidism, thyroid cancer, breast cancer, endocrine tumors, squamous cell carcinoma of the head and neck, and more. He is board certified by the American Board of Surgery, the Mexican Board of General Surgery and the Mexican Board of Oncology.
He is a member of various medical associations such as the American College of Surgeons, American Thyroid Association, American Head and Neck Society, American Medical Association, American Society of Clinical Oncology, Association of Academic Surgeons, Society of Surgical Oncology, The Society of Surgery of the Alimentary Tract, Society of American Gastrointestinal Endoscopic Surgeons, and the American Society of Breast Surgeons, among others.
Specialty:
Head and Neck Surgery Thyroid and Parathyroid Surgery Breast Surgery Complex Surgical Oncology
Areas of Clinical Interest:
Malignant thyroid disease (papillary, follicular, medullary, anaplastic thyroid cancer, thyroid lymphoma, and metastatic disease to the thyroid gland) benign thyroid diseases (goiter, multinodular goiter, substernal goiter, hyperthyroidism), hyperparathyroidism / hypercalcemia, benign and malignant breast diseases, head and neck surgery and head and neck cancer.
👉Without surgery, primary hyperparathyroidism results in decreased bone density in the majority of patients, raising questions regarding how long patients should be followed without intervention.
Haymart MR, Banerjee M, Stewart AK, Koenig RJ, Birkmeyer JD, Griggs JJ. Use of radioactive iodine for thyroid cancer. JAMA. 2011;306(7):721–728.
Type:
Observational cohort using the National Cancer Database (NCDB) and SEER registries from 2004 to 2008
Population:
189,219 adult patients with well-differentiated thyroid cancer (papillary or follicular) who underwent total thyroidectomy at 981 U.S. cancer centers
Objectives:
Analyze trends in RAI usage from 1990 to 2008
Identify patient-, tumor-, and hospital-level predictors of RAI administration
Assess variation in use across centers, adjusted for disease severity
Key Findings:
Rising Use Over Time
RAI utilization increased significantly across all tumor sizes between 1990 and 2008
Variation Driven by Non-Clinical Factors
Patient / tumor characteristics explained ~21% of variation in RAI use
Hospital traits (type, volume) accounted for ~17%, and 29% remained unexplained, suggesting practice pattern influence
Disease Stage and Use:
Compared to Stage IV:
Patients with Stage I disease were much less likely to receive RAI (OR 0.34), but Stage II / III use was similar to Stage IV (OR ~1)
Regional Disparities:
Rate of RAI use for low-, medium-, and high-risk disease varied by region (49% to 66%):
Indicating inconsistency in treatment approaches
Clinical Implications:
Overuse concern:
Increasing RAI use even in low-risk settings raises questions about overtreatment
Practice patterns matter:
Institutional priorities and physician preferences strongly influenced whether patients received RAI, beyond tumor biology
Guideline alignment needed:
The lack of deficit-stage conformity highlights a need to standardize RAI delivery based on risk stratification, not provider bias
Takeaway for Expert Surgeons:
Recognize that RAI is often employed inconsistently, even for Stage II to III disease, despite limited evidence of benefit in these groups
Encourage benchmarking and quality initiatives within institutions to ensure RAI administration aligns with ATA risk-based guidelines
Educate multidisciplinary teams that evidence-based risk stratification should dictate RAI use, minimizing unnecessary exposure for patients with lower-stage disease
If multi-gland disease (MGD) in primary HPT is known preoperatively:
Genetic testing should be considered prior to operation:
As this may further change the operative approach
There are two distinct operative approaches in MGD:
Total parathyroidectomy with auto-transplantation (TP)
Sub-total parathyroidectomy (STP):
In a sub-total parathyroidectomy, the most normal appearing gland is chosen to be the remnant (ideally an inferior gland):
Which is then cut back to approximately the size of a normal gland
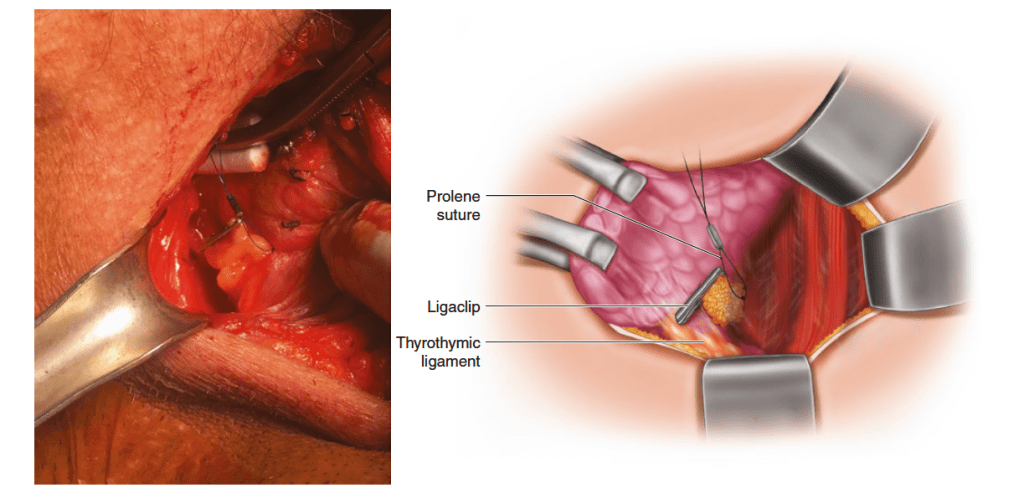
The gland is subsequently tagged with a Prolene suture:
Cut 1 to 2 cm long with a Hemoclip on the ends:
Which will aid in identification should re-exploration be required
Care should be taken not to compromise the vascular supply of the gland with this suture
Tagging of the remnant gland in sub-total parathyroidectomy. The gland chosen to be the remnant has been cut back to approximately the size of a normal gland. The gland is subsequently tagged with a Prolene suture, cut 1 to 2 cm long with a Hemaclip on the ends, which will aid in identification should re-exploration be required. Care should be taken not to compromise the vascular supply of the gland with this suture
Each approach carries different risks, benefits, and indications, as shown in the Table:
Which should always be considered with regard to the patient and his or her underlying pathology (e.g., genetic syndrome, tertiaryHPT)
Risks, benefits, and indications for sub-total and total parathyroidectomy
Other important considerations when dealing with MGD include:
Cervical thymectomy:
Due to the increased risk of ectopic supernumerary glands in MGD
Cryo-preservation of resected tissue:
Should be performed to protect against the rare, though devastating, complication of permanent hypoparathyroidism due to graft or remnant failure
If available, iPTH can be used to help guide the extent of resection in sub-total:
Aiming for a greater than 90% reduction at the completion of the operation
Close observation postoperatively for hypoparathyroidism and hungry bone syndrome regardless of approach
While all patients with symptomatic primary hyperparathyroidism (PHPT) should consider surgery (95% of patients are usually symptomatic when appropriate history is taken):
It is also indicated in some asymptomatic patients (5% of the cases of PHPT):
The normal feedback on parathyroid hormone production by extracellular calcium seems to be lost:
Resulting in a change in the set point
In primary hyperparathyroidism from parathyroid hyperplasia:
An increase in the cell numbers is probably the cause of the change in the set point
The chronic excessive resorption of calcium from bone caused by excessive parathyroid hormone can result in:
Osteopenia
In severe cases, this may result in osteitis fibrosa cystica:
Which is characterized by subperiosteal resorption of the distal phalanges, tapering of the distal clavicles, salt-and-pepper appearance of the skull, and brown tumors of the long bones
This is not commonly seen now
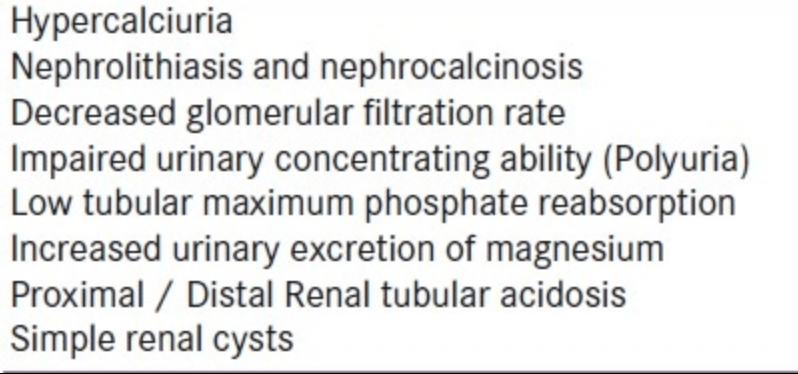
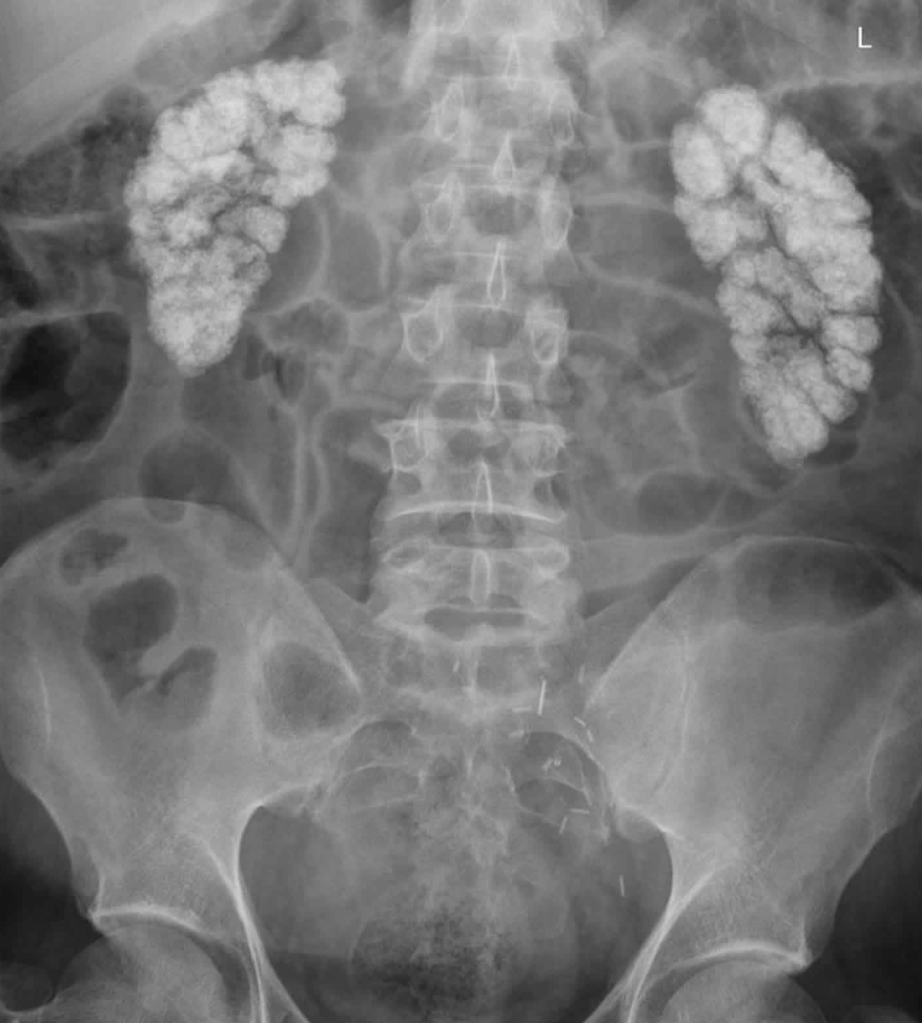
In addition, the chronically increased excretion of calcium in the urine:
Can predispose to the formation of renal stones
The other symptoms of hyperparathyroidism:
Are due to the hypercalcemia itself:
And are not specific to hyperparathyroidism
These can include:
Muscle weakness
Fatigue
Volume depletion
Nausea and vomiting
In severe cases, coma and death
Neuropsychiatric manifestations are particularly common and may include:
Depression
Confusion
Subtle deficits that are often characterized poorly and may not be noted by the patient (or may be attributed to aging)
Increased calcium can increase gastric acid secretion, and persons with hyperparathyroidism:
May have a higher prevalence of peptic ulcer disease
Rare cases of pancreatitis have also been attributed to hypercalcemia
A prospective cohort study by Ejlsmark-Svensson et al:
Reported that in patients with primary hyperparathyroidism, quality-of-life questionnaire scores were significantly lower:
In association with moderate-severe hypercalcemia:
Than in relation to mild hypercalcemia:
However, quality of life did not seem to be related to the presence of organ-related manifestations of primary hyperparathyroidism, such as osteoporosis, renal calcifications, and renal function impairment
This suggests that hypercalcemia is the primary driver of an impaired quality of life