- Bone disease, including:
- Osteopenia, osteoporosis, and osteitis fibrosa cystica:
- Is found in approximately 15% of patients with primary hyperparathyroidism at the time of diagnosis
- Increased bone turnover:
- As found in patients with osteitis fibrosa cystica:
- Can be determined by documenting:
- Elevated alkaline phosphatase concentration
- Can be determined by documenting:
- As found in patients with osteitis fibrosa cystica:
- Advanced PHPT with osteitis fibrosa cystica:
- Now occurs in less than 5% of patients
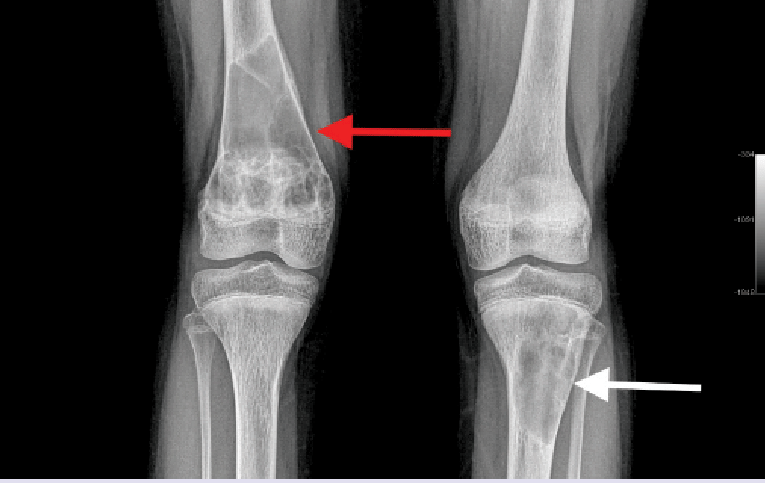
- The classic manifestation of PHPT bone disease is:
- Osteitis fibrosa cystica:
- Which is characterized clinically by bone pain and radiographically by subperiosteal bone resorption
- It has pathognomonic radiological findings:
- Which are best seen on radiographs of the hands:
- And are characterized by subperiosteal resorption:
- Most evident in the radial aspect of the middle phalanx of the second and third fingers
- Bone cysts
- Tuft formation of the upper part of the distal phalanges
- And are characterized by subperiosteal resorption:
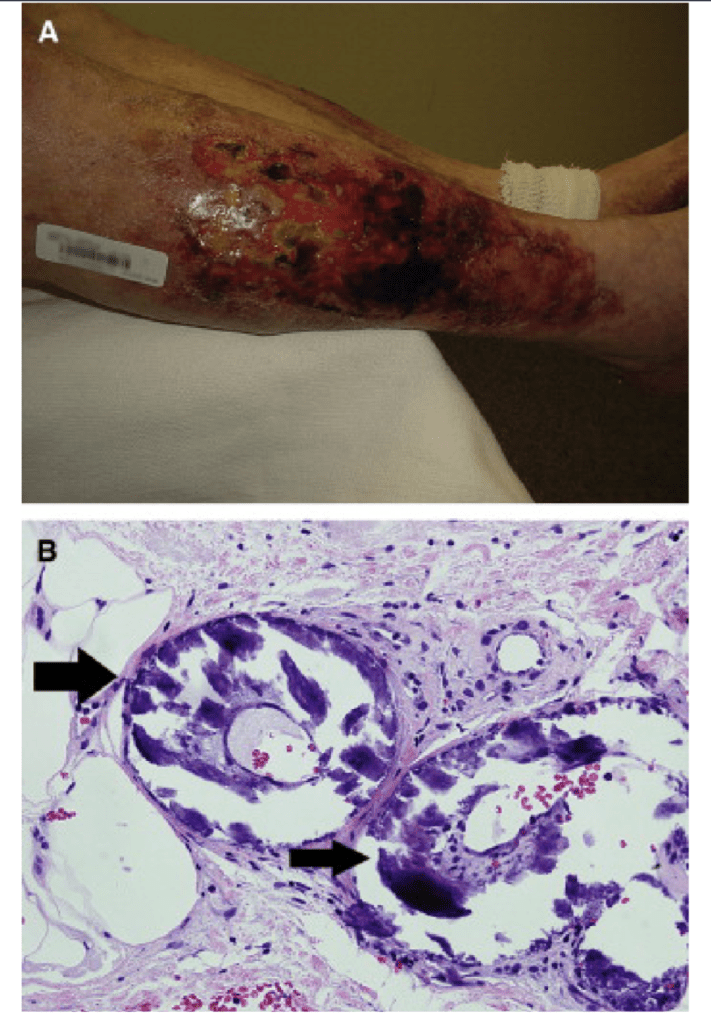
- Brown or osteoclastic tumors of the long bones:
- Result from excess osteoclast activity:
- And consist of collections of osteoclasts intermixed with fibrous tissue and poorly mineralized woven bone
- The brown coloration is due to:
- Hemosiderin deposition
- Result from excess osteoclast activity:
- Tapering of the distal clavicle
- Which are best seen on radiographs of the hands:
- Patients with normal serum alkaline phosphatase levels:
- Rarely have clinically apparent osteitis fibrosa cystica
- Osteitis fibrosa cystica:
- Osteopenia, osteoporosis, and osteitis fibrosa cystica:
- PHPT typically results in a loss of bone volume:
- At the cortical bone sites such as:
- The radius
- Relative preservation of cancellous bone:
- As found in vertebral bodies
- Patients with primary hyperparathyroidism, however:
- May also have osteoporosis in the lumbar spine that dramatically improves after parathyroidectomy
- At the cortical bone sites such as:
- Fractures are also more common in patients with primary hyperparathyroidism, and the incidence of fractures:
- Also decreases after parathyroidectomy:
- Bone disease is correlated with serum PTH and vitamin D levels
- Also decreases after parathyroidectomy:




#Arrangoiz #ParathyroidSurgeon #ParahthyroidExpert #Hyperparathyroidism #HeadandNeckSurgeon #EndocrineSurgery #MountSinaiMedicalCenter #MSMC #Miami #Mexico