-
In 1952, Schwartz coined the term atrophica idiopathica mucosa oris to describe an oral fibrosing disease he discovered in 5 Indian women from Kenya.
-
Joshi subsequently coined the termed oral submucous fibrosis (OSF) for the condition in 1953.
-
-
Oral submucous fibrosis is a chronic debilitating disease of the oral cavity characterized by inflammation and progressive fibrosis of the submucosal tissues (lamina propria and deeper connective tissues):
-
Oral submucous fibrosis results in marked rigidity and an eventual inability to open the mouth.
-
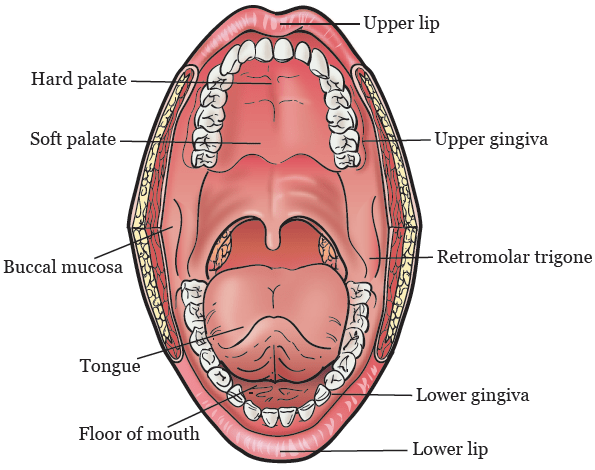
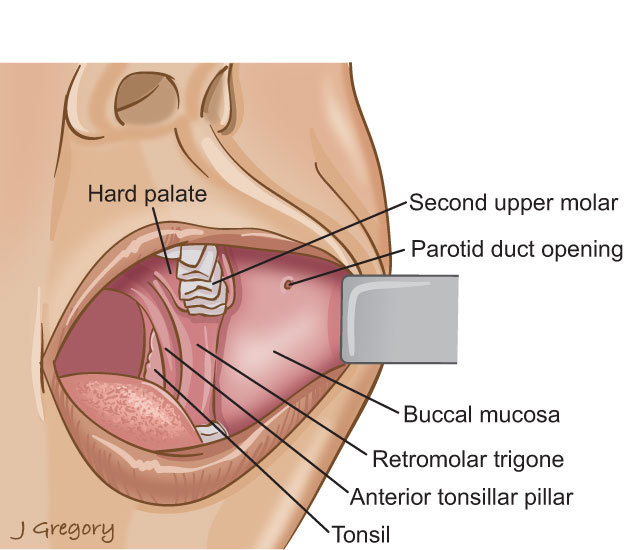
The buccal mucosa is the most commonly involved site, but any part of the oral cavity can be involved, even the pharynx
-
-
Oral submucous fibrosis (OSF) is a premalignant condition caused by betel chewing:
-
It is very common in Southeast Asia but has started to spread to Europe and North America.
-
The condition is well recognized for its malignant potential and is particularly associated with areca nut chewing, the main component of betel quid.
-
Betel quid chewing is a habit practiced predominately in Southeast Asia and India that dates back for thousands of years.
-
It is similar to tobacco chewing in westernized societies.
-
-
The mixture of this quid, or chew, is a combination of the areca nut (fruit of the Areca catechu palm tree, erroneously termed betel nut) and betel leaf (from the Piper betel, a pepper shrub), tobacco, slaked lime (calcium hydroxide), and catechu (extract of the Acacia catechu tree).
-
Lime acts to keep the active ingredient in its freebase or alkaline form, enabling it to enter the bloodstream via sublingual absorption.
-
Arecoline, an alkaloid found in the areca nut, promotes salivation, stains saliva red, and is a stimulant:
-
Major constituents of betel quid are arecoline from betel nuts and copper, which are responsible for fibroblast dysfunction and fibrosis.
-
-
-



-
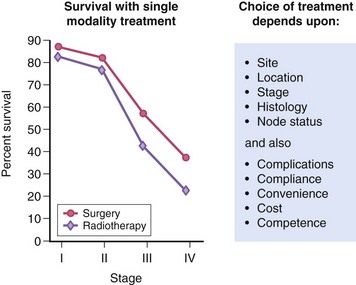
OSF can lead to squamous cell carcinoma, a risk that is further increased by concomitant tobacco consumption.
-
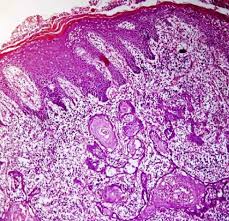
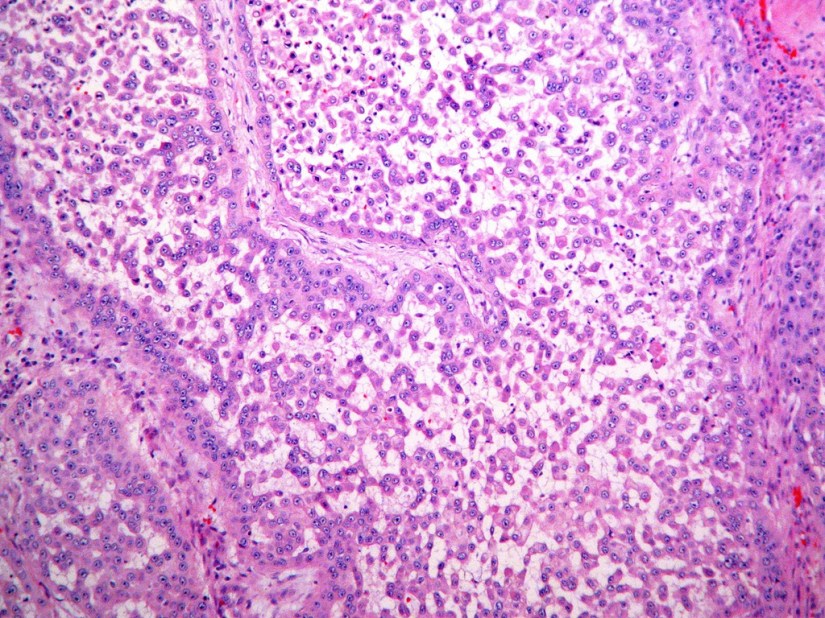
OSF is a diagnosis based on clinical symptoms and confirmation by histopathology.
-
Hypovascularity leading to blanching of the oral mucosa, staining of teeth and gingiva, and trismus are major symptoms:
-
Symptoms of oral submucous fibrosis (OSF) include the following:
-
Progressive inability to open the mouth (trismus) due to oral fibrosis and scarring
-
Oral pain and a burning sensation upon consumption of spicy foodstuffs
-
Increased salivation
-
Change of gustatory sensation
-
Hearing loss due to stenosis of the eustachian tubes
-
Dryness of the mouth
-
Nasal tonality to the voice
-
Dysphagia to solids (if the esophagus is involved)
-
Impaired mouth movements (eg, eating, whistling, blowing, sucking)
-
-
-
-
-
- Oral submucous fibrosis is clinically divided into three stages, and the physical findings vary according:
- Stage 1:
- Stomatitis includes erythematous mucosa, vesicles, mucosal ulcers, melanotic mucosal pigmentation, and mucosal petechia.
- Stage 1:
- Stage 2:
- Fibrosis occurs in ruptured vesicles and ulcers when they heal, which is the hallmark of this stage.
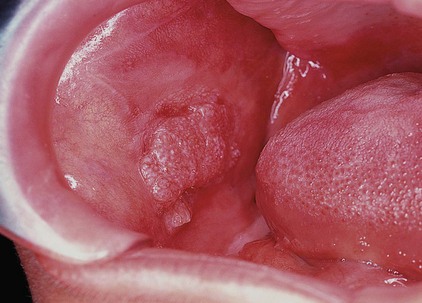
- Early lesions demonstrate blanching of the oral mucosa.
- Older lesions include vertical and circular palpable fibrous bands in the buccal mucosa and around the mouth opening or lips, resulting in a mottled, marblelike appearance of the mucosa because of the vertical, thick, fibrous bands running in a blanching mucosa.
- Specific findings include the following:
- Reduction of the mouth opening (trismus)
- Stiff and small tongue
- Blanched and leathery floor of the mouth
- Fibrotic and depigmented gingiva
- Rubbery soft palate with decreased mobility
- Blanched and atrophic tonsils
- Shrunken budlike uvula
- Sinking of the cheeks, not commensurate with age or nutritional status
- Fibrosis occurs in ruptured vesicles and ulcers when they heal, which is the hallmark of this stage.
- Stage 3:
- Leukoplakia is precancerous and is found in more than 25% of individuals with oral submucous fibrosis.
- Speech and hearing deficits may occur because of involvement of the tongue and the eustachian tubes.
Rodrigo Arrangoiz MS, MD, FACS a head and neck surgeon and is amember of Sociedad Quirúrgica S.C at the America British Cowdray Medical Center.He is first author on some publications on oral cavity cancer:
-
Oral Tongue Cancer: Literature Review and Current Management
-
Understand Cancer: Research and Treatment Oral Cavity Cancer: Literature Review and Current Management.
 • Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery: • Masters in Science (Clinical research for health professionals):
• Masters in Science (Clinical research for health professionals):








 • Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina:
• Cirugia oncológica / tumores de cabeza y cuello / cirugia endocrina: • Maestria en ciencias (Clinical research for healthprofessionals):
• Maestria en ciencias (Clinical research for healthprofessionals): • Cirugia de tumores de cabeza y cuello / cirugiaendocrina
• Cirugia de tumores de cabeza y cuello / cirugiaendocrina