👉After a rapid rise in thyroid cancer rates in the United States over nearly 30 years, the steady climb tapered from 2009 to 2014 and has appeared to be stable ever since, new research shows.
👉Between 2009 and 2016, after three decades of rapid increase, the incidence of thyroid cancer incidence in the United States reached a plateau and possibly started to decline.
👉Although a true decline in the occurrence of thyroid cancer is a possible explanation for these changing trends, less intensive workup of thyroid nodules is more likely.
👉From 1974 to 2013, the incidence of thyroid cancer in the United States tripled, from 4.5 to 14.4 cases per 100,000 in the population.
👉Although other factors have not been ruled out, the unprecedented rise in incidence is widely believed to have resulted from the advent of newer imaging technologies capable of detecting smaller, subclinical thyroid cancers that are of low risk.
👉The new finding that incidence rates have leveled off reflects a trend that has been happening for some time in which there has been an evolving understanding of overdiagnosis and the indolent nature of many small thyroid cancers.
👉Studies of autopsies have shown that clinically occult thyroid cancers are detected in 4% to 11% of people who have no known thyroid disease, underscoring the fact that small thyroid cancers are commonly inconsequential, they note.
👉The appreciation of the indolent nature of many thyroid cancers was reflected in changing clinical practice guidelines, including recommendations against screening for thyroid cancer by the US Preventive Services Task Force in 2017.
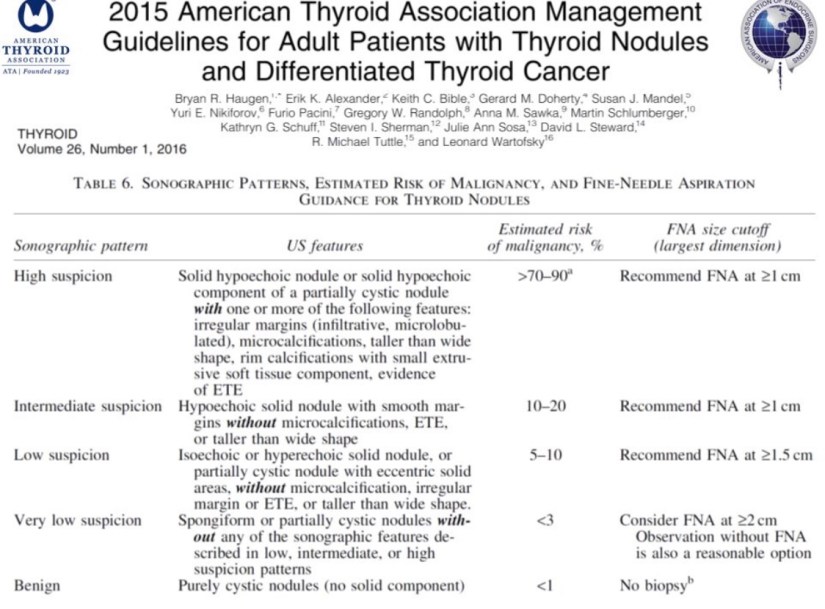
👉Other changes in guidelines include radiographic classification systems for thyroid nodules that have been implemented by several US professional societies and recommendations that the routine use of biopsy of nodules be more closely stratified according to risk.
👉In 2009 and 2015, for example, American Thyroid Association guidelines introduced size- and appearance-based criteria and recommended observation rather than immediate biopsy for many smaller, lower-risk nodules, the authors note.
👉Trends in other countries offer more extreme examples of the effects of thyroid screening, the authors state. In South Korea, the widespread practice of screening healthy individuals with thyroid ultrasound corresponded with a surge in thyroid cancer incidence to a level 15 times greater in 2011 than in 1993.
👉Subsequently, upon awareness of the likely role of thyroid screening processes in the trend and a significant revision of screening practices, thyroid cancer incidence rates in South Korea reversed.
👉For the study, Marti and colleagues analyzed data from the population-based Surveillance, Epidemiology, and End Results (SEER) 13 registry, representing 14% of the US population in 13 geographic regions.
👉They found an age-adjusted increase in thyroid cancer incidence from 5.7 to 13.8 per 100,000 individuals from 1992 to 2009. The highest annual percentage change, 6.6% (95% confidence interval [CI], 6.2% – 7.0%), occurred from 1998 to 2009.
👉Subsequently, a significant slowing, from 13.8 to just 14.7 per 100,000, occurred from 2009 to 2014 (annual percentage change, 2.0%; 95% CI, 0.3% – 3.7%; P = .001).
👉Since 2014, the incidence has remained stable, and there has even been a slight decline, from 14.7 to 14.1 cases per 100,000 (annual percentage change, –2.4%; 95% CI, –7.5% to 3.1%; P = .06).
👉With regard to subcentimeter thyroid cancers, which are believed to have largely driven the higher overall incidence rates, the authors found an expectedly larger increase in rate. From 1992 to 2009, the rate of subcentimeter cancers increased from 1.2 to 4.7 per 100,000; the highest annual percentage change occurred from 1996 to 2009 (9.1%; 95% CI, 8.4% – 9.8%).
👉That increase in subcentimeter cancers stabilized from 2009 to 2013, with an incidence of 4.7 to 5.3 per 100,000, for an annual percentage change of just 2.9% (95% CI, −2.5% to 8.6%; P = .02).
👉Further decline in subcentimeter thyroid cancers was observed from 2013 to 2016, from 5.3 to 4.7 per 100,000 (annual percentage change −3.7%; 95% CI, −8.7% to 1.7%; P = .04).
👉The patterns reflect not only the increasing ability to detect smaller cancers but also the subsequent awareness of the implications, the authors note.
#Arrangoiz
#ThyroidExpert
#ThyroidCancer
#ThyroidSurgeon
#CancerSurgeon
#SurgicalOncologist
#ThyroidNodules
#HeadandNeckSurgeon