👉Rodrigo Arrangoiz MS, MD, FACS is the first thyroid surgeon in Mexico to utilize this test in the management of a thyroid nodule.
👉He is now a member of Center for Advanced Surgical Oncology in Miami
👉ThyroSeq Genomic Classifier (GC) is a test for the pre-operative assessment of thyroid nodules with indeterminate cytology:
👉Which offers accurate assessment of cancer probability in a given nodule and additionally provides information on cancer prognostication, helping to select the most optimal patient management.
👉ThyroSeq incorporates all major scientific advances in thyroid cancer genetics and has more than 10-years’ experience serving physicians and their patients with thyroid nodules and cancer.
👉The first version of ThyroSeq was launched for clinical use at the University of Pittsburgh Medical Center as a seven-gene panel (ThyroSeq v0) in April of 2007.
👉Until recently, the test was offered as ThyroSeq v2. Today, ThyroSeq v3 is available for clinical use.

👉ThyroSeq v3 is also based on next-generation sequencing of DNA and RNA. However, it is expanded to analyze 112 genes, providing information on greater than 12,000 mutation hotspots and greater than 150 gene fusion types (Nikiforova MN et al. 2018).
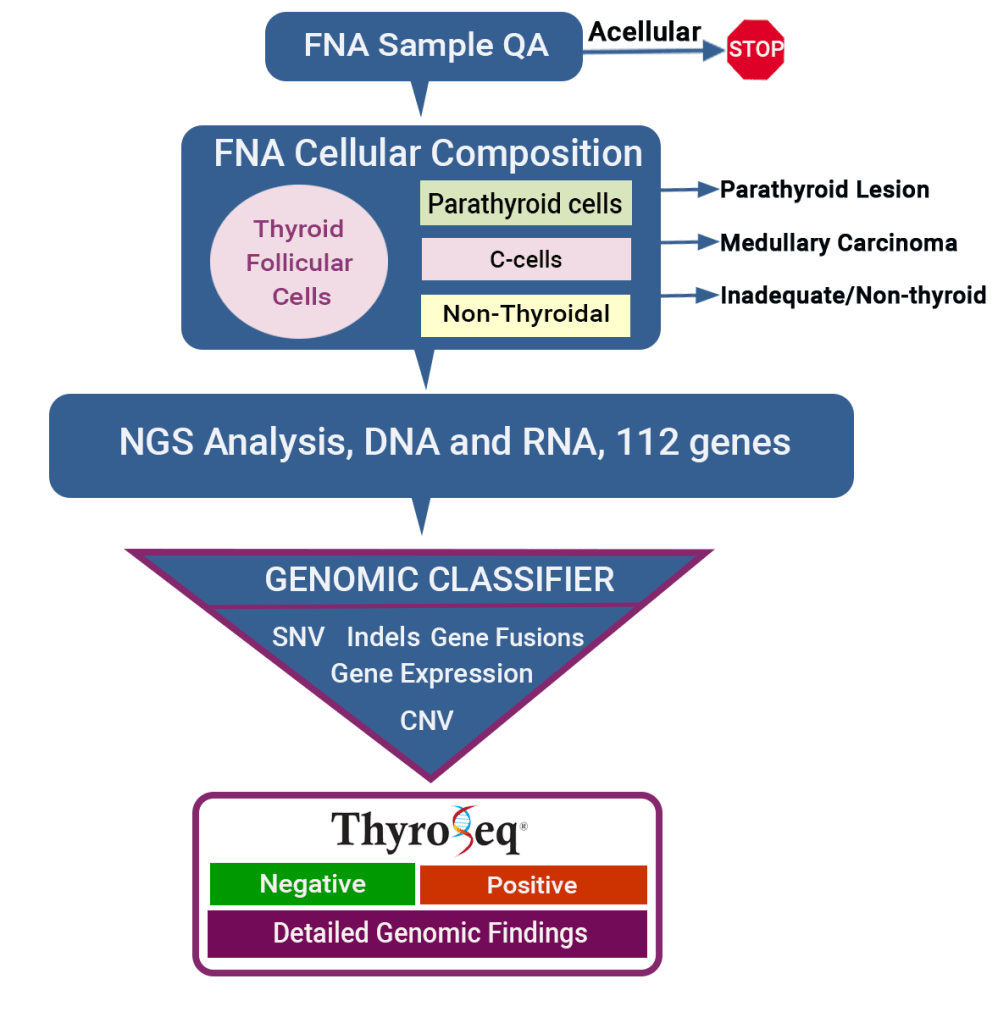
👉The test detects four classes of genetic alterations: (i) mutations (SNVs, indels); (ii) gene fusions; (iii) gene expression alterations; and (iv) copy number variations (CNVs).
👉The test utilizes a proprietary Genomic Classifier (GC) based on the algorithmic analysis of all detected genetic alterations to report the test result as Positive or Negative.
👉ThyroSeq test consists of several steps:
- It starts with the assessment of the FNA sample cellularity:
- This is a quality assurance (QA) step that determines if the provided sample has sufficient number of cells to proceed with the analysis.
- If the number of cells is below the required limit, the test is cancelled and no charges are posted.
- Next, cellular composition of the sample is evaluated:
- This step assures that the provided sample has an adequate proportion of thyroid follicular cells.
- It also allows accurate detection of c-cells (MTC), parathyroid cells, and other non-thyroidal cells.
- Then, the generated next generation sequencing data on 112 genes are processed using an in-house bioinformatic pipeline that applies a complex algorithm to estimate cancer probability in the tested nodule:
- The algorithm was built based on cancer probability associated with each genetic alteration and their combination and validated in a prospective, multicenter, double-blind study.
- Next, the test results and findings are reviewed by a board-certified pathologist who verifies all findings and releases the test report.
- ThyroSeq test report is provided in a user-friendly format that states the probability of cancer in the patient’s nodule, suggests potential patient management, and also lists specific genomic alterations that are relevant to the individual patient.
- You can expect results within 2 weeks from the time your specimen is received.
#Arrangoiz #ThyroidSurgeon #ThyroidExpert #ThyroidCancer #HeandandNeckSurgeon #CancerSurgeon #ThyroidNodules #Thyroseq