My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
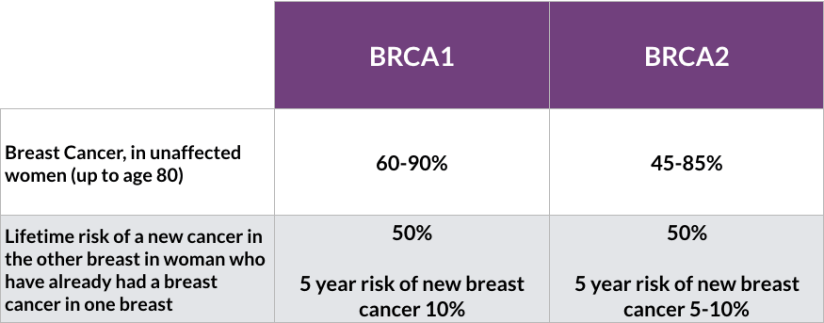
The risk of contralateral breast cancer at 20 years post initial breast cancer diagnosis is:
41% in BRCA1 mutation carriers:
Age at diagnosis does affect risk of contralateral breast cancer:
Women under 40 are at highest risk
Tamoxifen has been shown to decrease the risk of contralateral breast cancer overall
Phillips et al:
Report that estrogen receptor status of the initial breast cancer diagnosis did not affect contralateral breast cancer risk:
However the status was missing in over 50% of the cohort
In addition, women found to be at the highest risk:
Were those diagnosed with initial breast cancer under age 50
With two or more family members with history of breast cancer
Intact ovaries
The 15-year risk of contralateral breast cancer was 68% in these women
These women should be counseled about risk reducing contralateral mastectomy and salpingo-oopherectomy
The strongest predictor of contralateral risk was oophorectomy
Contralateral prophylactic mastectomy is a controversial area in breast surgical oncology, and patient decision-making around this process continues to be studied
References
Metcalfe K, Gershman S, Lynch HT, et al. Predictors of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. Br J Cancer. 2011;104(9):1384–1392.
Phillips KA, Milne RL, Rookus MA, et al. Tamoxifen and risk of contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2013;31(25):3091-3099.
Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317(23):2402-2416.
However, local recurrence and distant recurrence remains quite high:
Close monitoring is recommended
The role of chemotherapy:
Is unclear
Therefore, surgery should remain the primary treatment of choice
Preoperative radiation:
With hyperfractionated and accelerated radiation therapy:
Has also been identified as a potential alternative to surgery alone, with improved survival and should be considered:
More trials are needed to improve outcomes for this aggressive but rare complication of radiation
References
Torres, K.E., Ravi, V., Kin, K. et al. Long-term outcomes in patients with radiation-associated angiosarcomas of the breast following surgery and radiotherapy for breast cancer. Ann Surg Oncol. 2013;20(4):1267-1274.
Palta M , Morris CG, Grobmyer SR, Copeland EM, Mendenhall NP. (2010), Angiosarcoma after breast‐conserving therapy. Cancer. 116(8):1872-1878.
Smith TL, Morris CG, Mendenhall NP. Angiosarcoma after breast-conserving therapy: long-term disease control and late effects with hyperfractionated accelerated re-irradiation (HART). Acta Oncol. 2014;53(2):235-241.
Penel N, Bui BN, Bay JO, et al. Phase II trial of weekly paclitaxel for unresectable angiosarcoma: the ANGIOTAX Study. J Clin Oncol. 2008;26(32):5269-5274.
Palta M, Morris CG, Grobmyer SR, Copeland EM 3rd, Mendenhall NP. Angiosarcoma after breast-conserving therapy: long-term outcomes with hyperfractionated radiotherapy. Cancer. 2010;116(8):1872-1878.
Three important conclusions are agreed upon regarding this clinical entity:
Prognosis of occult primary breast cancer is the same or slightly better than women with classic stage IIA disease (T0, N1, M0)
An exhaustive workup for the non-breast primary is usually not fruitful
Treatment of the breast in some manner decreases the risk of local failure over time
Modified radical mastectomy has been the traditional surgical treatment for many years
Previously, the primary breast cancer was found in the mastectomy specimen:
40% to 80% of the time, but with the advent of much better mammography and ultrasound along with breast MRI, this rate is much lower now
However, what was true then and still holds today:
Is that no treatment to the breast itself results in an unacceptably high local recurrence rate
An alternative to a modified radical mastectomy:
Is complete ALND followed by whole-breast irradiation
Axillary dissection:
Provides local control while also fine tuning staging
Theoretically the whole-breast radiation:
Should control any subclinical disease in the breast not detected on imaging
Primary radiation to the breast, axilla, and supraclavicular area without any surgery of the breast or axilla:
Results in higher local and regional recurrence compared to surgery and radiation combined
Axillary node dissection and whole-breast irradiation:
Has been found to have equivalent survival as a modified radical mastectomy
A recent meta-analysis of 7 studies and more than 240 patients with occult primary breast cancers (0.3% to 0.8% of all breast cancers):
Found 39% were treated with ALND and radiation while 47% had modified radical mastectomy and 15% had ALND alone
With a mean follow-up of 5 years:
The study found no difference in local regional recurrence (12.7% vs 9.8%), distant metastasis (7.2% vs 12.7%), or mortality (9.5% vs 17.9%) between ALND and radiation vs modified radical mastectomy (all p>0.16)
ALND with radiation was superior to ALND alone in terms of local regional recurrence (12.7% vs 34.3%, p < 0.01) and trended towards improved survival but this was not statistically significant (P=0.09)
References:
Barton SR, Smith IE, Kirby AM, Ashley S, Walsh G, Parton M. The role of ipsilateral breast radiotherapy in management of occult primary breast cancer presenting as axillary lymphadenopathy. Eur J Cancer. 2011;47(14):2099-2106.
Macedo FI, Eid JJ, Flynn J, Jacobs MJ, Mittal VK. Optimal surgical management for occult breast carcinoma: a meta-analysis. Ann Surg Oncol. 2016;23(6):1838-1844.
Rueth NM, Black DM, Limmer AR, et al. Breast conservation in the setting of contemporary multimodality treatment provides excellent outcomes for patients with occult primary breast cancer. Ann Surg Oncol. 2015;22(1):90-95.
Walker GV, Smith GL, Perkins GH, et al. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis. Cancer. 2010;116(17):4000-4006.
Hessler LK, Molitoris JK, Rosenblatt PY, et al. Factors Influencing management and outcome in patients with occult breast cancer with axillary lymph node involvement: analysis of the National Cancer Database. Ann Surg Oncol. 2017;24(10):2907-2914.
Macedo FI, Eid JJ, Flynn J, Jacobs MJ, Mittal VK. Optimal surgical management for occult breast carcinoma: a meta-analysis. Ann Surg Oncol. 2016;23:1838-1844. https://www.ncbi.nlm.nih.gov/pubmed/26832884
Walker GV, Smith GL, Perkins GH, et al. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis. Cancer. 2010;116:4000-4006. PMID: 20564117. http://www.ncbi.nlm.nih.gov/pubmed/20564117
Woo SM, Son BH, Lee JW, et al. Survival outcomes of different treatment methods for the ipsilateral breast of occult breast cancer patients with axillary lymph node metastasis: a single center experience. J Breast Cancer. 2013;16:410-416. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3893343/
Is frequently useful to assess for lymph node involvement in patients with breast cancer at initial disease presentation:
However, normal appearing lymph nodes on ultrasound, before and/or after chemotherapy:
Do not obviate the need for surgical axillary staging
Axillary ultrasound with percutaneous biopsy of any suspicious lymph nodes, if present:
Allows marking of the positive node:
To be sure it is removed following treatment with neoadjuvant chemotherapy
Plecha et al. recently published data:
That show wire localization of marked nodes increases the likelihood of removing the node that was positive prior to neoadjuvant chemotherapy
Boughey et al.:
Had previously shown that clipping the positive node decreases the false-negative rate of sentinel node biopsy following neoadjuvant chemotherapy
Supraclavicular disease:
Is classified as N3, stage IIIC disease, not as distant metastatic disease:
Supraclavicular involvement can be documented by percutaneous biopsy:
Excision is not required prior to chemotherapy
Removal of sentinel lymph nodes prior to neoadjuvant chemotherapy:
Interferes with assessment of nodal response to chemotherapy
PET/CT scan is not needed to plan nodal staging after neoadjuvant chemotherapy:
Small volume disease is poorly detected with this modality:
So axillary ultrasound is preferred:
Regardless of imaging results, surgical staging of the axilla is required
References
Boughey JC, Ballman KV, Symmans WF, et al. Methods impacting the false-negative rate of sentinel lymph node surgery in patients presenting with node-positive breast cancer (T0–T4, N1–2) who receive neoadjuvant chemotherapy: results from a prospective trial—ACOSOG Z1071 (Alliance). Poster presented at: San Antonio Breast Cancer Symposium; December 9-13, 2014; San Antonio, TX.
Plecha D, Bai S, Patterson H, Thompson C, Shenk R. Improving the accuracy of axillary lymph node surgery in breast cancer with ultrasound-guided wire localization of biopsy proven metastatic lymph nodes. Ann Surg Oncol. 2015;22(13):4241-4246.
Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer-Verlag; 2010.
Kuerer HM, Sahin AA, Hunt KK, et al. Incidence and impact of documented eradication of breast cancer axillary lymph node metastases before surgery in patients treated with neoadjuvant chemotherapy. Ann Surg. 1999;230(1):72-78.
Hieken TJ, Trull BC, Boughey JC, et al. Preoperative axillary imaging with percutaneous lymph node biopsy is valuable in the contemporary management of patients with breast cancer. Surgery. 2013;154(4):831-838; discussion 838-840.
Diagnosis of a breast cancer during pregnancy requires:
A complex treatment plan with multiple multidisciplinary providers:
From both oncology and obstetrics:
Coordinating the timing of cancer treatment and the delivery of a high-risk pregnancy
Gestational or pregnancy-associated breast cancer:
Refers to any breast cancer diagnosed:
During pregnancy or within the first year after childbirth
This is a rare diagnosis:
Yet remains the most common cancer in pregnant women:
Affecting approximately 15 to 35 per 100,000 deliveries:
Approximately 0.05%
The majority of pregnancy-associated breast cancers are:
Ductal in origin
More likely to be poorly-differentiated
ER negative or PR negative and HER2-positive compared to non-pregnant women
Present at advanced stages
Evaluation of a dominant breast mass should include:
Ultrasound and mammogram with fetal shielding, and core biopsy:
Interpretation of mammography can be difficult in the highly dense tissue of pregnant women
Use of MRI during pregnancy is both contraindicated and unhelpful:
Gadolinium contrast may cause fetal harm during the first trimester and is typically avoided
Although the majority (approximately 80%) of breast biopsies in pregnant women will be benign:
It is critical that malignancy be ruled out
Fine needle aspiration during pregnancy is associated with a higher rate of false positive and false negative results, without receipt of tumor markers:
Therefore core biopsy is recommended
Routine staging is not recommended:
In an asymptomatic patient with early-stage breast cancer
Routine staging if indicated:
Should be performed per National Comprehensive Cancer Network guidelines:
With consideration given to safety of both the patient and fetus
CT scans are not recommended due to excessive fetal radiation exposure
Early termination of pregnancy, is not thought to improve outcome in these patients
Staging should be performed in women with advanced disease, and in those with symptoms concerning for metastases:
This should include:
Chest radiograph with fetal shielding
Liver ultrasound or MRI without contrast
“Low-dose” radionuclide bone scans
When possible, treatment of pregnancy-associated breast cancers:
Should follow similar guidelines to non-pregnant patients, and if at all possible, the pregnancy should be carried to term
Systemic treatment of breast cancer during pregnancy:
Involves special consideration of both the mother and baby
Surgery is safe at all stages
Chemotherapy can be delivered:
From 14 weeks of gestation following completion of organogenesis through 35 weeks,:
When it should be stopped to avoid leukopenia in preparation for delivery
Data from a single-institution prospective study indicates that:
FAC chemotherapy (5-FU, doxorubicin, and cyclophosphamide) is safe during the second and third trimesters:
With fetal malformations approximating 1%
Experience with taxanes remained limited:
There are insufficient safety data regarding the use of taxanes during pregnancy and as such they are not recommended for general use during pregnancy
But the National Comprehensive Cancer Network (NCCN) guidelines:
Recommend weekly paclitaxel if warranted
Methotrexates are contraindicated due to teratogenic side effects
Although 20% of pregnancy-associated breast cancers are HER2-positive:
Anti-HER2 therapy including trastuzumabhas not been proven safe during pregnancy and is best delivered in the adjuvant setting
Anhydramnios has been reported with use of trastuzumab during pregnancy
MotHER, a prospective U.S. registry:
Is evaluating women exposed to trastuzumab +/- pertuzumab during pregnancy or within 6 months of conception and following pregnancy outcomes and infants for the first month of life:
Current recommendations suggest that targeted anti-HER2 therapy be delayed until after delivery
Breast conservation is not recommended:
If radiation would be timed during pregnancy because this is contraindicated:
However, it can be performed if radiation falls after delivery
Axillary lymph node dissection was previously recommended:
But sentinel lymph node biopsy is feasible and should be offered
Hormone therapy should be postponed until after childbirth
Chemotherapy during pregnancy can cause concerns for the fetus which depend on the timing of drug administration:
In the first trimester:
Congenital malformations can occur
In the second and third trimester the greatest concerns are :
Prematurity
Low birth weight
Myelosuppression
Among approved chemotherapy agents:
Long-term outcomes of children with in-utero exposure demonstrate normal development, cognition, and school performance when prematurity is controlled for
Brent RL. The effect of embryonic and fetal exposure to x-ray, microwaves, and ultrasound: counseling the pregnant and nonpregnant patient about these risks. Sem Oncol. 1989;16(5):347-368.
Meisel JL, Economy KE, Calvillo KZ, et al. Contemporary multidisciplinary treatment of pregnancy-associated breast cancer. Springerplus. 2013;2(1):297.
Pant S, Landon MB, Blumenfeld M, Farrar W, Shapiro CL. Treatment of breast cancer with trastuzumab during pregnancy. J Clin Oncol. 2008;26(9):1567-1569.
Yang WT, Dryden MJ, Gwyn K, Whitman GJ, Theriault R. Imaging of breast cancer diagnosed and treated with chemotherapy during pregnancy. Radiology. 2006;239(1):52-60.
Berry DL, Theriault RL, Holmes FA, et al. Management of breast cancer during pregnancy using a standardized protocol. J Clin Oncol. 1999;17(3):855-861.
Macdonald HR Pregnancy associated breast cancer. Breast J. 2020 Jan 14. doi: 10.1111/tbj.13714. [Epub ahead of print]
Goidescu I, Nemeti G, Caracostea G, Eniu DT, Chiorean A, Pintican R, Cruciat G, Muresan D. The role of imaging techniques in the diagnosis, staging and choice of therapeutic conduct in pregnancy associated breast cancer. Med Ultrason. 2019 Aug 31;21(3):336-343. doi: 10.11152/mu-1958. Review.
Alfasi A, et al. Breast Cancer during Pregnancy-Current Paradigms, Paths to Explore. Cancers. 2019; 11: 1669
Gooch JC1,2, Chun J1, Kaplowitz E1, Guth A1, Axelrod D1, Shapiro R1, Roses D1, Schnabel F1. Pregnancy-associated breast cancer in a contemporary cohort of newly diagnosed women Breast J. 2019 Aug 25. doi: 10.1111/tbj.13510. [Epub ahead of print]
The role of locoregional treatment in the setting of de novo metastatic breast cancer:
Is controversial
Typically, surgery has been reserved for:
Palliation
A 2012 meta-analysis of 15 retrospective studies:
Showed resection of the primary tumor was associated with:
Increased overall survival:
OS; HR 0.69, 95% CI 0.63 to 0.77, P<0.00001
Unfortunately, recent prospective studies have shown conflicting results:
A Turkish study showed improved survival at a median of 40 months follow-up:
Especially in more indolent forms of breast cancer
In contrast, a U.S. study did not show improvement in survival associated with surgery
Determinants of improved survival:
Were related to response to therapy
An Italian study showed:
Improvement in survival:
In patients with HER2 positive disease after first-line trastuzumab-based therapy
In addition, an Indian study by Badwe et al:
Did not show a survival advantage with resection of the primary cancer:
At a median follow-up of 23 months:
The overall survival was 41.9% in the locoregional surgical arm vs. 43.0% in the non-locoregional treatment arm
Each of these studies has potential bias flaws:
But show potential benefit of resection:
In select patients with:
High functional status and good response to optimal systemic therapy
While awaiting the results of ECOG E2108 clinical trial:
Surgery in stage IV breast cancer:
Patients should be discussed in a multidisciplinary setting, taking into account:
Comorbidities, response to therapy, and tumor burden
References
Poggio F, Lambertini M, de Azambuja E. Controversies in oncology: Surgery of the primary tumour in patients presenting with de novo metastatic breast cancer: to do or not to do? ESMO Open 2018;3:e000324.
Wu SG, Zhang WW, Sun JY, et al. The survival benefits of local surgery in stage IV breast cancer are not affected by breast cancer subtypes: a population-based analysis. Oncotarget. 2017;8(40):67851-67860. Published 2017 Jun 29.
Soran A, Ozmen V, Ozbas S, et al. randomized trial comparing resection of primary tumor with no surgery in Stage IV breast cancer at presentation: Protocol MF07-01. Ann Surg Oncol. 2018;25(11): 3141-3149.
R Badwe, R Hawaldar, N Nair, et al.: Locoregional treatment versus no treatment of the primary tumour in metastatic breast cancer: an open-label randomised controlled trial. Lancet Oncol. 2015;16(13):1380-1388.
Rebbeck TR, Kauff ND, Domchek SM. Meta-analysis of risk reduction estimates associated with risk-reducing salpingo-oophorectomy in BRCA1 or BRCA2 mutation carriers. J Natl Cancer Inst. 2009;101(2):80-87.
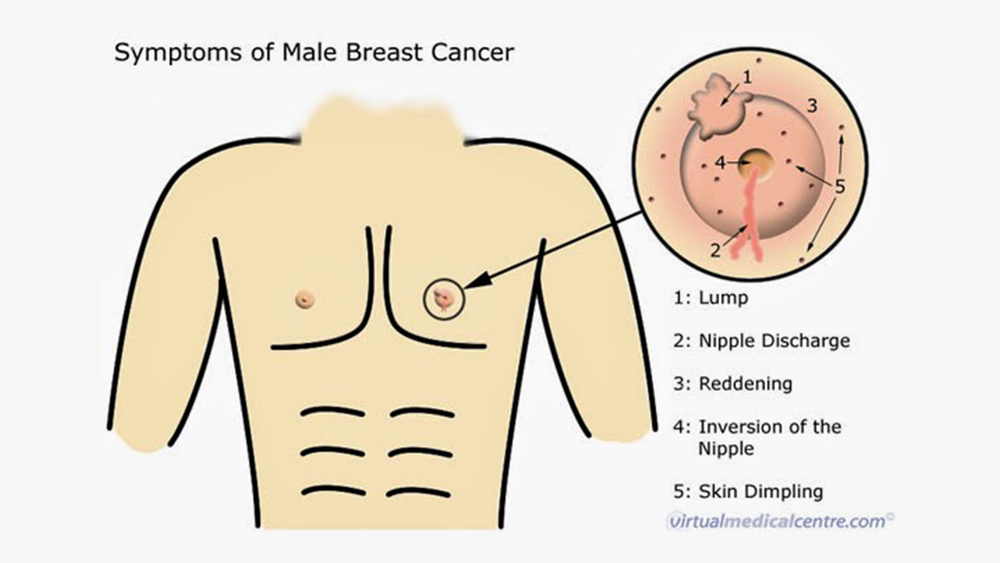
Male breast cancer accounts for less than 1% of all breast cancers:
There have been no randomized control trials for surgical management of breast cancer in men
Although breast conservation is increasing:
The current surgical management remains simple mastectomy with sentinel lymph node biopsy
Sentinel lymph node biopsy has been demonstrated to be accurate in men
There are no data to support staging studies:
Such as positron emission tomography (PET) or computed tomography (CT):
In early-stage breast cancer in either men or women
The role of the 21-gene signature assay is an emerging field in male breast cancer
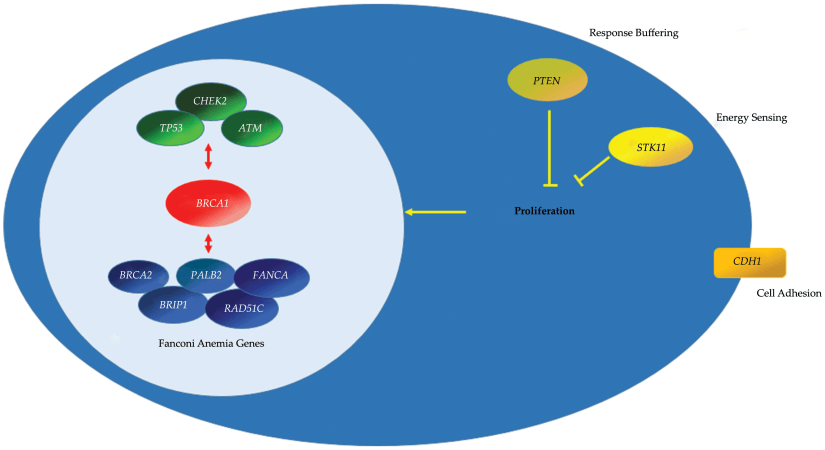
Approximately 10% of male breast cancers are associated with genetic mutations:
BRCA2 is the most common among the mutations:
With a lifetime risk of 5% to 10% among BRCA2 carriers
Klinefelter’s is also associated with an increased risk of male breast cancer:
With an incidence between 3% and 7%
All male breast cancer patients should be referred for genetic counseling and testing
Endocrine therapy is indicated for ER+ breast cancer:
Aromatase inhibitors can be used but have not been well-studied in men
Tamoxifen is the best-studied drug for male breast cancer
The role of hormonal therapy in male breast cancer has not been evaluated by a prospective, randomized trial
Nevertheless, the rationale for estrogen blockade in male breast cancer is the same as that for female breast cancer:
With numerous prospective, randomized trials supporting the role of endocrine therapy:
To reduce risk of breast cancer recurrence and death
Anti-hormone therapy may also provide chemoprevention for the contralateral breast in men treated by ipsilateral mastectomy
The majority of male breast cancer is ER+ and thus eligible for targeted antiestrogen therapy
Men who have breast cancer:
Should not take testosterone therapy:
Because it may stimulate breast cancer growth by modulating increased estrogenic activity
The balance between estrogen and testosterone in men may have physiologic effects on breast tissue
References
Fentiman IS. Surgical options for male breast cancer. Breast Cancer Res Treat. 2018;172(3):539-544.
Gentilini O, Chagas E, Zurrida S, Intra M, De Cicco C, Gatti G, et al. Sentinel lymph node biopsy in male patients with early breast cancer. Oncologist. 2007;12(5):512-515.
Massarweh SA, Sledge GW, Miller DP, McCullough D, Petkov VI, Shak S. Molecular characterization and mortality from breast cancer in men. J Clin Oncol 2018;36:1396-1404.
Giordano SH. Breast cancer in men. N Engl J Med. 2018;378(24):2311–2320.
Korde LA, Zujewski JA, Kamin L, et al. Multidisciplinary meeting on male breast cancer: summary and research recommendations. J Clin Oncol. 2010;28(12):2114-2122.
Greif JM, Pezzi CM, Klimberg VS, Bailey L, Zuraek M. Gender differences in breast cancer: analysis of 13,000 breast cancers in men from the National Cancer Data Base. Ann Surg Oncol. 2012;19:3199-3204.
Kiluk JV, Lee MC, Park CK, Meade T, et al. Male breast cancer: management and follow-up recommendations. Breast J. 2011;17:503-509.
Mendez, JE, ter Meulen D, Padussis J, et al. Tissue compression is not necessary for needle-localized lesion identification. Amer J Surg. 2005;190(4):580-582.
Graham RA, Homer MJ, Katz J, Rothschild J, Safaii H, Supran S. The pancake phenomenon contributes to the inaccuracy of margin assessment in patients with breast cancer. Am J Surg. 2002;184(2):89-93.
Graham RA, Homer MJ, Sigler CJ et al. The efficacy of specimen radiography in evaluating the surgical margins of impalpable breast carcinoma. AJR Am J Roentgenol. 1994;162(1):33-36.
As the primary method of axillary staging for patients with early stage breast cancer
Changes in patient presentation and advancements in systemic therapy:
Have led clinicians to question the utility of ALND even in the presence of involved nodes
The American College of Surgeons Oncology Group (ACOSOG) Z0011 trial:
Randomized women with T1 / T2 tumors undergoing breast conservation with one or two positive sentinel nodes to undergo ALND vs. no additional axillary surgery
Results showed no difference in local recurrence, disease-free survival (DFS), or overall survival (OS) between the groups
The authors concluded that ALND was not indicated in this setting
One of the major advantages of SLNB compared to ALND:
Is the ability to stage the axilla with reduced rates of lymphedema
A recent meta-analysis of five randomized controlled trials (including the Z0011 trial):
Reported a 70% reduction in risk of lymphedema with SLNB compared to ALND
Multi-gene assays such as the 21-gene recurrence score (RS):
Have provided prognostic information regarding risk of distant recurrence:
For patients with node-negative, ER+ breast cancers
Although evidence suggests that adding chemotherapy to endocrine therapy does result in improved DFS and OS for node-positive patients:
Exploratory data suggest that this may not be true for all patients
A retrospective analysis of the RS performed on 367 specimens from the SWOG 8814 trial:
Showed that RS was prognostic for DFS and OS in node-positive patients
The National Comprehensive Cancer Network:
Allows patients with 1 to 3 positive nodes to consider the 21-gene recurrence score to determine benefit from chemotherapy
References
Giuliano AE, Ballman K, McCall L, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: long-term follow-up from the American College of Surgeons Oncology Group (Alliance) ACOSOG Z0011 randomized trial. Ann Surg. 2016; 264(3):413-420.
Glechner A, Wockel A, Gartlehner G, et al. Sentinel lymph node dissection only versus complete axillary lymph node dissection in early invasive breast cancer: a systematic review and meta-analysis. Eur J Cancer. 2013;49(4):812-825.
Albain KS, Barlow WE, Shak S, et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, estrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11(1):55-65.