- The ACOSOG Z1071 trial:
- Was designed to determine the false negative rate (FNR) of sentinel lymph node biopsy (SLNB) after neoadjuvant chemotherapy (NAC) in women initially presenting with cN1 disease
- The trial enrolled women from 136 institutions who had:
- Clinical T0 through T4, N1 through N2, M0 breast cancer who received neoadjuvant chemotherapy
- Patients enrolled had pre-chemotherapy axillary nodal disease confirmed by fine-needle aspiration or core needle biopsy
- Following NAC:
- Patients underwent both SLNB, followed by a back-up axillary lymph node dissection
- SLNB with dual tracer using both blue dye (isosulfan blue or methylene blue) and a radiolabeled colloid mapping agent was encouraged
- Rates of detection of at least one SLN were 92.9% in patients with cN1 disease and 89.5% in patients with cN2 disease
- Overall, the FNR of SLNB after NAC was 12.6%
- Bivariable analyses found that the likelihood of a false-negative SLN finding was significantly decreased when:
- The mapping was performed with the combination of blue dye and radiolabeled colloid:
- P=.05; FNR, 10.8% combination vs 20.3% single agent
- By removal of at least 3 SLNs:
- P=.007; FNR, 9.1% for ≥ 3 SLNs vs 21.1% for two
- The mapping was performed with the combination of blue dye and radiolabeled colloid:
- A clip was placed at initial node biopsy prior to NAC in 203 patients:
- In the 170 (83.7%) patients with cN1 disease and at least two SLNs resected, clip location was confirmed in 141 cases
- In 107 (75.9%) patients where the clipped node was within the SLN specimen, the FNR was 6.8% (confidence interval [CI]: 1.9%-16.5%)
- If the clipped node was found in the ALND specimen, the FNR was 19.0% (CI: 5.4%-41.9%)
- In cases where a clip was not placed (n = 355) and in those where the clipped node location was not confirmed at surgery (n = 29):
- The FNR was 13.4% and 14.3%, respectively
- While the FNR overall exceeded the 10% threshold considered to be clinically acceptable:
- The authors concluded that with modifications to the SLN technique (i.e., dual tracer mapping and retrieval of at least 3 negative SLNs), to the FNR was < 10% and supported the use of SLN surgery as an alternative to axillary lymph node dissection in this patient population
- Subsequently, Caudle et al have reported a separate registry of 191 patients and showed that removing the clipped positive node in addition to SLN:
- Had an FNR as low as 2.0%
- References
- Boughey JC, Suman VJ, Mittendorf EA, Ahrendt GM, Wilke LG, Taback B, et al.; Alliance for Clinical Trials in Oncology. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (Alliance) clinical trial. JAMA. 2013;310(14):1455-1461.
- Boughey JC, Ballman KV, Le-Petross HT, McCall LM, Mittendorf EA, Ahrendt GM, et al. Identification and resection of clipped node decreases the false-negative rate of sentinel lymph node surgery in patients presenting with node-positive breast cancer (T0-T4, N1-N2) who receive neoadjuvant chemotherapy: results from ACOSOG Z1071 (Alliance). Ann Surg. 2016;263(4):802-807.
- Caudle AS, Yang WT, Krishnamurthy S, Mittendorf EA, Black DM, Gilcrease MZ, et al. Improved axillary evaluation following neoadjuvant therapy for patients with node-positive breast cancer using selective evaluation of clipped nodes: implementation of targeted axillary dissection. J Clin Oncol. 2016;34(10):1072-1078.
Author: Rodrigo Arrangoiz MS, MD, FACS, FSSO
My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
- The presence of goiter was originally determined from autopsy studies that weighed the thyroid gland, but this was superseded by the use of ultrasound by which a goiter is diagnosed if:
- The size of the thyroid gland is greater than three standard deviations of the median:
- Volume 18 ml for women and 25 ml for men
- The size of the thyroid gland is greater than three standard deviations of the median:
- Goiter is more common in iodine-deficient regions of the world:
- Where endemic goitre affects 10% of the population
- In Framingham:
- Clinically apparent nodules (palpation) were present in:
- 6.4% of women and 1.5% of men:
- The presence of single thyroid nodules was 3%, and multinodular goiter was 1%
- 6.4% of women and 1.5% of men:
- Clinically apparent nodules (palpation) were present in:
- In an autopsy study in 1955:
- 50% of people had thyroid nodules and the majority were multiple
- Like autopsy, imaging frequently reveals subclinical thyroid nodules and, when ultrasound is used in epidemiological studies:
- The estimate of goiter prevalence is 19% to 67%
- Incidental thyroid nodules are seen in up to:
- 25% of contrast-enhanced chest CT scans
- 16% to 18% of CT and MR scans of the neck
- 1% to 2% PET scans
- In patients under 40 years:
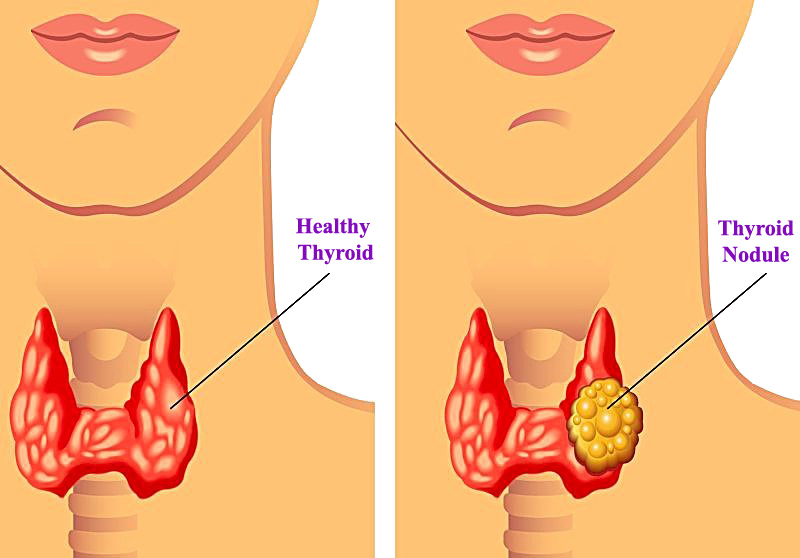
- The goiter is typically a solitary nodule,
- Whereas diffuse goitrer is more common over the age of 65 years
- The female to male ratio is:
- 4:1

Clinical Presentation of Euthyroid Goiter
- Patients present with a painless lump and are often unsure as to its duration:
- The increased size of the goiter can lead to symptoms related to pressure effects on adjacent structures such as:
- Dysphagia (from pharyngeal and/or esophageal compression)
- Globus sensation
- Hoarseness (from laryngeal or recurrent laryngeal nerve compression)
- Shortness of breath (from tracheal deviation and compression)
- The increased size of the goiter can lead to symptoms related to pressure effects on adjacent structures such as:
- An incidental thyroid nodule (ITN) is one of the most common incidental findings on imaging studies that include the neck:
- Guidelines have been developed to assist the medical provider in deciding when and how to investigate ITN
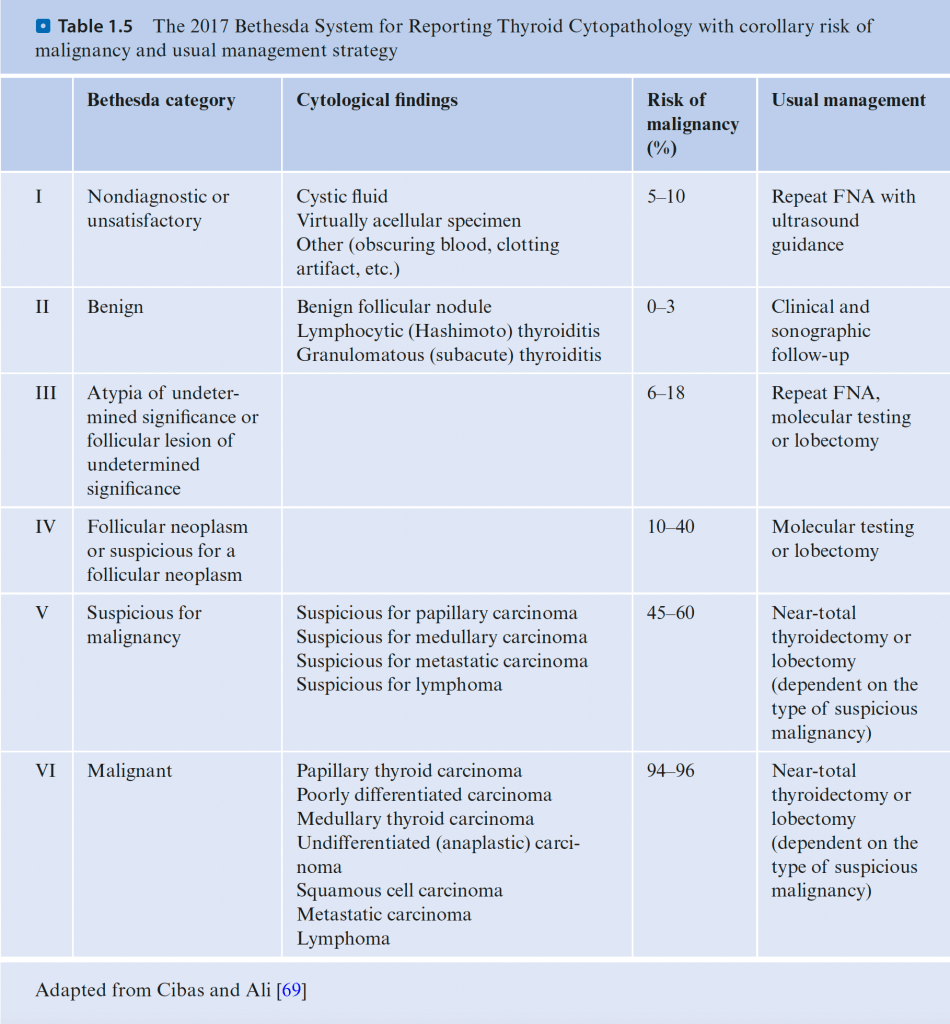
Bethesda System for Reporting Thyroid Cytopathology
What is the most common surgical side effect of sentinel lymph node dissection as reported by the American College of Surgeons Oncology Group (ACOSOG) Z0010 t
- The overall significant complication rate from sentinel lymph node dissection reported from the ACOSOG Z0010 trial:
- Was low, with 32% of patients reporting at least one surgical side effect and less than 1% of patients requiring hospitalization
- The most common surgical side effect was axillary paresthesia:
- Affecting 307 (8.6%) of 3,573 patients
- Allergic reaction was reported in less than 1% related to the administration of lymphazurin blue dye
- Lymphedema in 7%
- Brachial plexus injury in less than 1% of patients
- Only one anaphylactic reaction to blue dye was reported
- References
- Hunt KK, Ballman KV, McCall LM, Boughey JC, Mittendorf EA, Cox CE, et al. Factors associated with local-regional recurrence after a negative sentinel node dissection: results of the ACOSOG Z0010 trial. Ann Surg. 2012;256(3):428-436.
- Boughey JC, Hunt KK. The ACOSOG experience. In: Kuerer HM, ed. Kuerer’s Breast Surgical Oncology. New York, NY: McGraw-Hill Companies; 2010:517-530.
#Arrangoiz #BreastSurgeon #BreastCancer #SurgicalOncologist #CancerSurgeon #SLNB #SentinelLymphNodeBiopsy
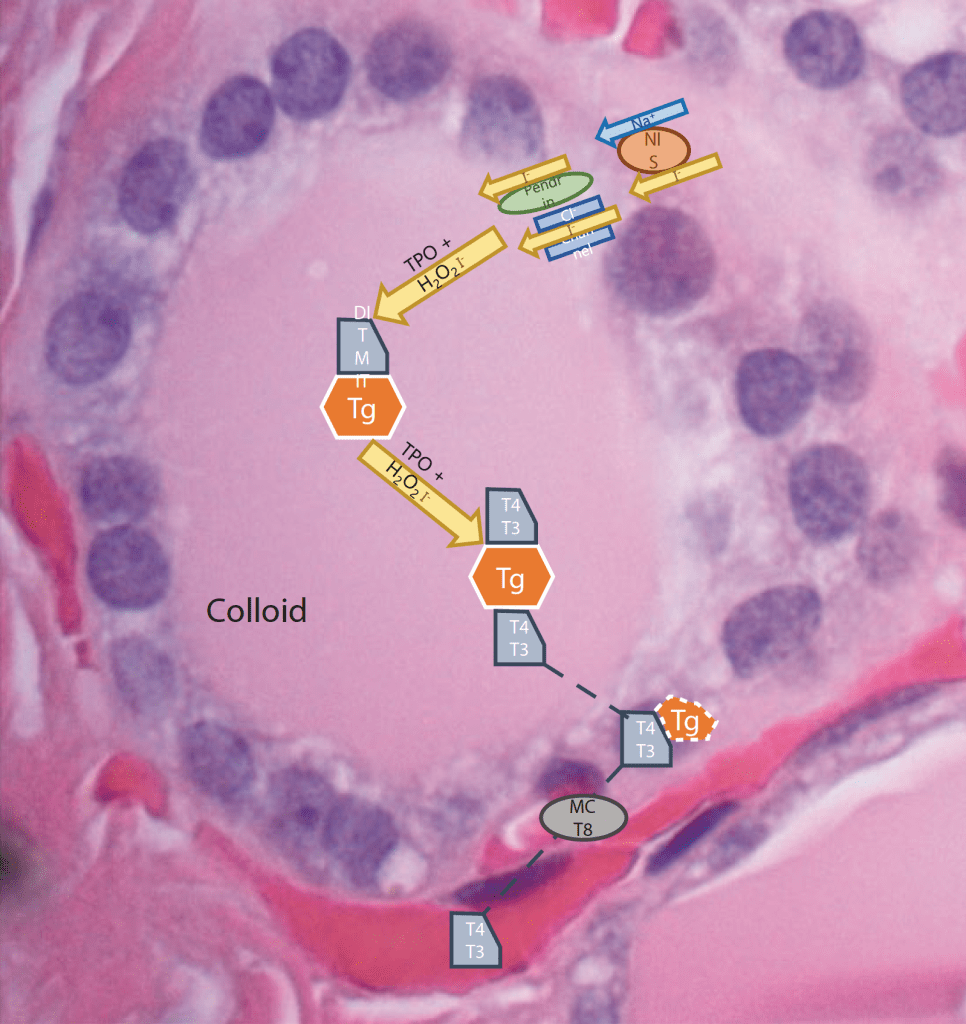
Thyroid Hormone Synthesis
- Active transport of iodine (I-) into the thyroid follicular cells:
- Is mediated by the Na/I symporter (NIS)
- Intracellular accumulated iodide ion is then passively translocated across the apical membrane into the colloid:
- Via pendrin proteins and Cl channels
- The effluxed iodide ion becomes covalently attached to thyroglobulin:
- Mediated by thyroperoxidase (TPO)
- Further iodinization of tyrosine molecules on the thyroglobulin glycoprotein then occurs via TPO forming:
- Monoiodotyrosines (MIT) and diiodotyrosines (DIT):
- Which are then coupled to create the bioactive thyroid hormones T4 and T3:
- Again catalyzed via TPO
- Which are then coupled to create the bioactive thyroid hormones T4 and T3:
- Monoiodotyrosines (MIT) and diiodotyrosines (DIT):
- Colloid is taken up into the follicular cell by:
- Micropinocytosis
- Through digestion of this thyroglobulin by:
- Lysosomal extracts and a resulting proteolytic breakdown of the thyroglobulin:
- T4 and T3 are released into the cytoplasm
- Lysosomal extracts and a resulting proteolytic breakdown of the thyroglobulin:
- Finally T4 and T3 are transported into the circulation by a hormone transporter:
- Monocarboxylate transporter 8 (MCT8)
#Arrangoiz #ThyroidSurgeon #CancerSurgeon #HeadandNeckSurgeon #EndocrineSurgeon #ThyroidHormone
Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer
- The 21-gene recurrence-score assay (e.g., Oncotype DX, Genomic Health):
- Is one of several commercially available gene-expression assays:
- That provide prognostic information in hormone-receptor-positive breast cancer
- Is one of several commercially available gene-expression assays:
- The assay originally set cut points for:
- Low risk at a recurrence score < 18
- Intermediate risk at 18 to 30
- High risk at > 31
- It is predictive of chemotherapy benefit when:
- The recurrence score (RS) is high (> 26), and prognostic for very low rates of distant recurrence (2% at 10 years) when the RS is low (< 10)
- The TAILORx prospective randomized clinical trial:
- Was completed to determine whether chemotherapy is beneficial for women:
- With an intermediate RS of 11 to 25
- The cutoffs for this trial were adjusted to ensure all patients in the intermediate range who may benefit were included
- At 9 years of follow-up:
- The endocrine therapy only and the chemo-endocrine therapy group:
- Had similar rates of invasive disease-free survival:
- 83.3% vs. 84.3% respectively
- Had similar rates of invasive disease-free survival:
- The endocrine therapy alone was noninferior to chemoendocrine therapy for all patients in the intermediate RS study group
- The two groups also had similar outcomes in freedom from disease recurrence at a distant or locoregional sites
- However, the chemotherapy benefit for invasive disease-free survival varied with the combination of recurrence score and age (P=0.004):
- With some benefit of chemotherapy found in women 50 years old or younger with an RS of 16 to 25
- In women less than 50 receiving chemotherapy demonstrated a lower rate of distant recurrence than endocrine therapy if RS was 16 to 20 (percentage-point difference, 0.8 at 5 years and 1.6 at 9 years) or 21 to 25 (percentage-point difference, 3.2 at 5 years and 6.5 at 9 years)
- Overall survival however remained similar
- The endocrine therapy only and the chemo-endocrine therapy group:
- For this reason, researchers conclude that the 21-gene assay can identify women with ER postive early-stage breast cancer:
- Who may be spared chemotherapy if they are over 50 years old with an RS of 25 or lower, as well as women 50 years or younger with RS of 15 or lower
- Was completed to determine whether chemotherapy is beneficial for women:
- References
- Sparano JA, Gray RJ, Makower DF, Pritchard K, Albain KS, Hayes DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med. 2018;379(2):111-121.
#Arrangoiz #BreastCancer #BreastSurgeon #OncotypeDx #SurgicalOncologist #21GeneRecurrenceScoreAssay #CancerSurgeon
Canadian Trial – Long-Term Results of Hypofractionated Radiation Therapy for Breast Cancer
- A multi-institution, prospective randomized trial:
- From participating Cancer Care Ontario centers was performed from 1993 to 1996
- The study sought to determine whether:
- Accelerated hypofractionated whole-breast irradiation (WBI) was as effective as conventional 5-week fractionation
- Included in the study were women who received:
- Breast-conserving surgery (BCS) for invasive breast cancer with clear surgical margins and negative axillary nodes
- Participants were randomly assigned to receive:
- WBI either at the standard dose of 50.0 Gy in 25 fractions over 35 days (control group), or at a dose of 42.5 Gy in 16 fractions over 22 days (hypofractionated-radiation group)
- The control group included 612 patients and the hypofractionation group had 622 patients
- Results from this study indicated:
- That the Canadian regimen was not inferior to the standard 5-week treatment regimen for women who received BCS for invasive breast cancer with clear surgical margins and negative axillary nodes
- The risk of local recurrence at 10 years was:
- 6.7% in the control group and 6.2% in the hypofractionated group
- Cosmesis at 10 years was found to be comparable between the 2 groups:
- With good or excellent outcomes for 71.3% of women in the control group and 69.8% in the hypofractionated-radiation group
- There was also no difference between the 2 groups in overall survival and no increase in cardiac-related deaths was seen in the hypofractionated group
- References
- Whelan TJ, Pignol J-P, Levine MN, Julian JA, MacKenzie R, Parpia S, et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med. 2010;362(6):513-520
#Arrangoiz #BreastSurgeon #BreastCancer #SurgicalOncologist #Miami #Mexico #RadiationTherapy #Hypofractionation
National Cancer Institute of Canada Clinical Trials Group (NCIC-CTG) MA.20 Trial
- The NCIC-CTG MA.20 trial:
- Randomized 1,832 high-risk women who were treated with breast-conserving surgery and sentinel node biopsy (SLNB) or axillary lymph node dissection (ALND) to:
- Either WBI alone or WBI plus regional nodal irradiation (RNI)
- Axillary lymph node dissection was required for any patients with a positive SLN
- RNI included the:
- Internal mammary nodes
- Supraclavicular nodes
- High axillary nodes
- The trial enrolled patients with node-positive or high-risk node-negative disease
- Eighty-five percent of patients had 1 to 3 positive nodes, 5% had more than 4 positive nodes, and 10% were node negative
- Node-negative patients:
- With tumors greater than or equal to 2 cm who had fewer than 10 axillary nodes removedwere considered high risk if they had at least one of the following:
- ER negative
- Lymphovascular invasion
- Nuclear grade 3
- With tumors greater than or equal to 2 cm who had fewer than 10 axillary nodes removedwere considered high risk if they had at least one of the following:
- All patients had systemic therapy.
- With a median follow-up of 10 years:
- The addition of RNI improved:
- Locoregional DFS from 92.2% to 95.2% (P=0.009)
- Distant DFS from 82.4% to 86.3% (P=0.03)
- There was no difference in OS from 81.8% to 82.8% (P=0.38)
- The addition of RNI to WBI was associated with:
- An increase in grade 2 or greater pneumonitis from 0.2% to 1.2% (P=0.01) and lymphedema from 4.5% to 8.4% (P=0.001)
- The addition of RNI improved:
- Randomized 1,832 high-risk women who were treated with breast-conserving surgery and sentinel node biopsy (SLNB) or axillary lymph node dissection (ALND) to:
- Similarly, European Organisation for Research and Treatment of Cancer (EORTC) 22922:
- Randomized 4004 women undergoing breast-conserving surgery or mastectomy and ALND for histological stage I, II, or III breast cancer to:
- RNI (supraclavicular and internal mammary nodal irradiation) or no regional nodal irradiation
- At a median follow-up of 10.9 years:
- The addition of regional nodal irradiation improved DFS from 69.1% to 72.1% (P=0.04)
- Again, there was a non-significant trend toward improvement in OS from 80.7% to 82.3% (P=0.06 among the RNI group.
- Randomized 4004 women undergoing breast-conserving surgery or mastectomy and ALND for histological stage I, II, or III breast cancer to:
- The results of NCIC-CTG MA.20:
- Have led many to conclude that all patients with axillary nodal metastases, regardless of tumor size or extent of nodal involvement:
- Should receive comprehensive nodal radiation therapy (RT)
- Have led many to conclude that all patients with axillary nodal metastases, regardless of tumor size or extent of nodal involvement:
- A major conundrum in current practice is resolving the apparently contradictory findings of American College of Surgeons Oncology Group (ACOSOG) Z0011 and After Mapping of the Axilla, Radiation or Surgery? (AMAROS) with those of MA.20
- The modest benefit in DFS with nodal RT in MA.20 may reflect differences in patient populations between the studies:
- Patients with clinically positive nodes were excluded from ACOSOG Z0011 and AMAROS (and not MA.20)
- In addition, fewer than 10 nodes were removed in one-third of patients in the MA.20 study and the median node count was 12, compared to a median of 17 in the ALND arms of Z0011 and AMAROS
- The modest benefit in DFS with nodal RT in MA.20 may reflect differences in patient populations between the studies:
- The benefit of nodal RT:
- Therefore may be limited to higher risk patients with more extensive nodal disease and perhaps more limited axillary surgery
- References
- Poortmans PM, Collette S, Kirkove C, Limbergen EV, Budach V, Struikmans H, et al. Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med. 2015;37(4)3:317-327.
- Pepels MJ, de Boer M, Bult P, van Dijck A, van Deurzen CH, Menke-Pluymers MB, et al. Regional recurrence in breast cancer patients with sentinel node micrometastases and isolated tumor cells. Ann Surg. 2012;255(1):116-121.
- Whelan TJ, Olivotto IA, Parulekar WR, Ackerman I, Chua BH, Nabid A, et al; MA.20 Study Investigators. Regional nodal irradiation in early-stage breast cancer. N Engl J Med.2015;373(4):307-316.
The Arimidex, Tamoxifen, Alone or in Combination (ATAC) Trial
- The Arimidex, Tamoxifen, Alone or in Combination (ATAC) trial:
- Was the first study to compare:
- A 3rd-generation aromatase inhibitor (AI), anastrozole, with tamoxifen for the adjuvant treatment of early breast cancer
- Was the first study to compare:
- The ATAC trial:
- As designed to compare the efficacy and safety of:
- Anastrozole (1 mg) with tamoxifen (20 mg) as adjuvant treatment for postmenopausal women with early-stage breast cancer
- Patients were treated every day for 5 years
- The study was a double-blind, prospective, randomized trial:
- With 9,366 postmenopausal women
- A proportional hazards model was used to assess:
- The primary endpoints of:
- DFS
- Secondary endpoints of:
- Time to recurrence
- Time to distant recurrence
- Overall survival
- Death with or without recurrence
- The primary endpoints of:
- The combination arm of anastrozole and tamoxifen:
- Was discontinued after the initial analysis:
- As it was found to have no efficacy or tolerability benefits over tamoxifen alone.
- Was discontinued after the initial analysis:
- Long-term follow-up of 120 months showed:
- Significant improvements in the anastrozole group versus the tamoxifen group for:
- DFS, time to recurrence, and time to distant recurrence
- In hormone receptor-positive patients:
- These benefits were seen to increase over time
- Recurrence rates were found to:
- Remain lower on anastrozole after treatment was completed
- There was little difference in overall survival:
- Between anastrazole and tamoxifen (hazard ratio, 0.95; 95% confidence interval, 0.84–1.06; P=0.4)
- Fractures were more frequent during the active treatment in patients receiving anastrozole:
- But were similar between the two groups in post-treatment follow-up
- Treatment-related serious adverse events:
- Were less common in the anastrozole group:
- But were also found to be similar between the two groups after treatment completion
- Anastrozole showed a non-significant increased incidence of colorectal cancer and lung cancers, and a decreased incidence of endometrial, melanoma, and ovarian cancers:
- However, only the decrease in endometrial cancers remained statistically significant after Bonferroni correction (P<0.001)
- Were less common in the anastrozole group:
- Overall, anastrozole was found to have:
- Superior long-term efficacy and safety than tamoxifen as initial adjuvant therapy for postmenopausal women with hormone-sensitive early-stage breast cancer
- Outcomes from the ATAC trial made anastrozole the preferred treatment for postmenopausal women with localized hormone receptor-positive breast cancer
- Significant improvements in the anastrozole group versus the tamoxifen group for:
- As designed to compare the efficacy and safety of:
- References
- Howell A, Cuzick J, Baum M, Buzdar A, Dowsett M, Forbes JF, et al. Results of the ATAC (arimidex, tamoxifen, alone or in combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. Lancet. 2005;365(9453):60-62.
- Cuzick J, Sestak I, Baum M, Buzdar A, Howell A, Dowsett M, et al; ATAC/LATTE Investigators. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol. 2010;11(12):1135-1141.
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOncologist #ATAC #EndocrineTherapy #Mexico #Miami #Teacher #Surgeon
