Familial non-medullary thyroid cancer (FNMTC) constitutes 3–9% of all thyroid cancer (TC) cases and is divided into syndromic and non-syndromic FNMTC. In syndromic a FNMTC, patients are at risk of non-medullary thyroid cancer (minor component) and multiple other tumors with syndrome-specific clinical features (Familial adenomatous polyposis, Gardner syndrome, Cowden syndrome, Werner syndrome, Carney complex). The genes for syndromic FNMTC are known.
In non-syndromic FNMTC, thyroid cancer is the major feature of the disease, and the susceptibility gene has not yet been identified.
First, let’s define the diagnosis and management of FNMTC. Population studies have shown that the risk of TC increases nine-fold in patients who have a first-degree relative with TC. Traditionally, FNMTC is diagnosed when two or more first-degree relatives are affected [1]. The probability that a patient’s cancer is FNMTC is greater than 95% when ≥3 first-degree relatives are affected, compared to 31–38% when only two first-degree relatives are affected [2]. However, given the high incidence of TC in the general population, patients with only two first-degree relatives with non-medullary thyroid cancer (NMTC) could represent sporadic disease (a chance occurrence) and not an inherited predisposition [2].
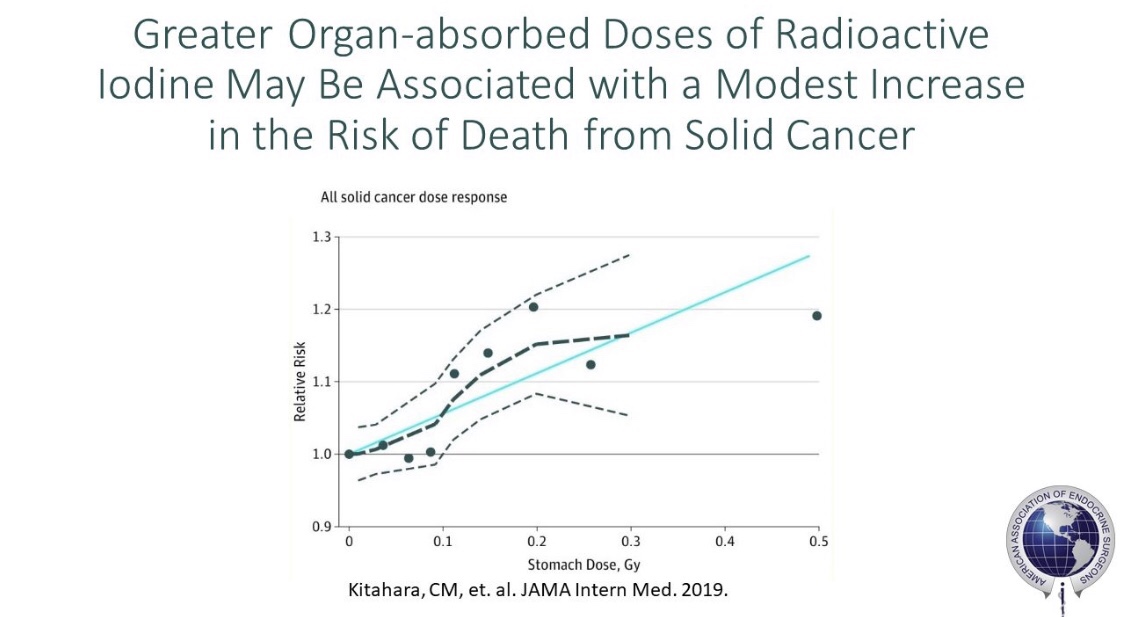
In a prospective screening study at the National Cancer Institute [3], Dr. Klubo-Gwiezdzinska used thyroid ultrasound and physical examination in family members who had at least two first-degree relatives affected with TC and evaluated thyroid nodules according to the ATA guidelines. They found that 4.6% of people in families with two affected first-degree relatives had TC diagnosed on screening, while 22.7% of those from families with ≥3 affected first-degree relatives had a TC diagnosis. All cases diagnosed by screening had smaller tumor size, lower rate of central neck lymph node metastases, needed less extensive initial surgical intervention, and had a lower rate of radioiodine therapycompared to patients who presented with clinical disease. The youngest age of TC detection was 18 years old. They suggested screening with thyroid ultrasound in patients with ≥3 family members affected by FNMTC [3, 4]. However, recent ATA guidelines do not recommend screening and surveillance in non-syndromic FNMTC, citing a lack of evidence. To date, it is unknown whether earlier detection of less-advanced disease via this proposed screening and surveillance approach would result in a lower rate of TC recurrence and TC-related death or in overdiagnosis and overtreatment.
Second, is FNMTC more aggressive than sporadic disease? This is still debated. A meta-analysis of 12 studies with a total of 12,741 participants compared the extent of disease and outcomes in non-syndromic FNMTC versus sporadic NMTC and found that FNMTC was associated with a younger age at diagnosis and higher rate of multifocal and bilateral tumors, extrathyroidal invasion, lymph node metastasis, and recurrence rate [5]. In a recent prospective cohort study comparing 78 patients with FNMTC to 53,571 NMTC patients [6], FNMTC cases presented at a younger age, with a greater rate of lymph node metastasis. On the other hand, a retrospective study in which 67 patients with FNMTC and 375 controls with sporadic disease were followed for 10 years showed similar long-term disease-free survival rates [7]. Some of these discrepancies are due to study design shortcomings, such as variable inclusion criteria/definitions for FNMTC, data based on retrospective studies, and small sample size.
Third, which are the genes believed to cause non-syndromic FNMTC? By performing linkage analyses and whole-genome/-exome sequencing studies, several candidate genes have been found, including the serine/arginine repetitive matrix 2 gene (SRRM2) [8]; HABP2 germline variant, G534E [9]; and genes involved in the MAPK/ERK and PI3K/AKT pathways [10]. However, all these variants appear to be present in only a few patients, are most often not present within all family members affected by FNMTC, and are subsequently not validated across different populations. Unstudied alternative mechanisms, such as epigenetic mechanisms, might be involved in FNMTC and warrant further investigations.
These findings highlight a real black box and the need for future large prospective studies. Ensuing results might help establish improved management guidelines for providers and patients with multiple family members harboring TC and raise their awareness about FNMTC.
References:
1. Malchoff, C.D. and D.M. Malchoff, Familial nonmedullary thyroid carcinoma. Cancer Control, 2006. 13(2): p. 106-10.
2. Charkes, N.D., On the prevalence of familial nonmedullary thyroid cancer in multiply affected kindreds. Thyroid, 2006. 16(2): p. 181-6.
3. Klubo-Gwiezdzinska, J., et al., Results of Screening in Familial Non-Medullary Thyroid Cancer. Thyroid, 2017. 27(8): p. 1017-1024.
4. Sadowski, S.M., et al., Prospective screening in familial nonmedullary thyroid cancer. Surgery, 2013. 154(6): p. 1194-8.
5. Wang, X., et al., Endocrine tumours: familial nonmedullary thyroid carcinoma is a more aggressive disease: a systematic review and meta-analysis. Eur J Endocrinol, 2015. 172(6): p. R253-62.
6. El Lakis, M., et al., Do patients with familial nonmedullary thyroid cancer present with more aggressive disease? Implications for initial surgical treatment. Surgery, 2019. 165(1): p. 50-57.
7. Robenshtok, E., et al., Clinical characteristics and outcome of familial nonmedullary thyroid cancer: a retrospective controlled study. Thyroid, 2011. 21(1): p. 43-8.
8. Tomsic, J., et al., A germline mutation in SRRM2, a splicing factor gene, is implicated in papillary thyroid carcinoma predisposition. Sci Rep, 2015. 5(10566).
9. Gara, S.K., et al., Germline HABP2 Mutation Causing Familial Nonmedullary Thyroid Cancer. N Engl J Med, 2015. 373(5):448-55.
10. Srivastava, A., et al., Whole Genome Sequencing of Familial Non-Medullary Thyroid Cancer Identifies Germline Alterations in MAPK/ERK and PI3K/AKT Signaling Pathways. LID – 10.3390/biom9100605 [doi] LID – 605. Biomolecules 2019. 9(10): p. 605.