- Immunohistochemical features suggestive of progression:
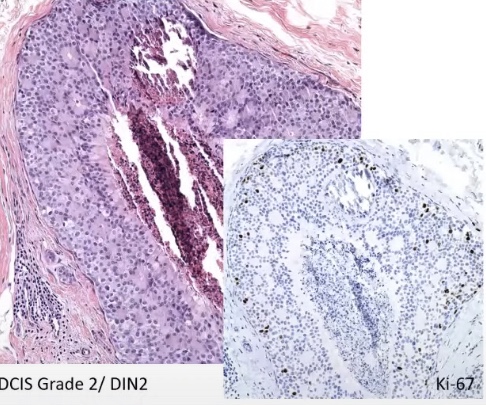
- Proliferation index (Ki-67):
- DCIS grade 2 / DIN 2 have a low proliferation index
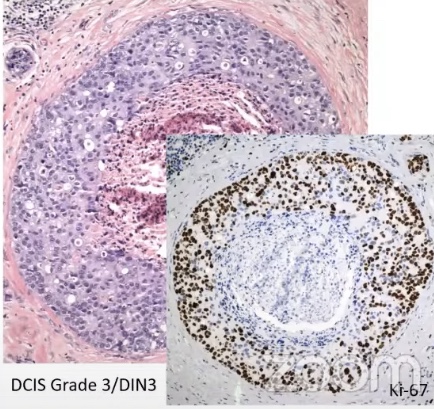
- DCIS grade 3 / DIN 3 have a high proliferation index
- Proliferation index (Ki-67):
- Immunohistochemical features suggestive of progression:
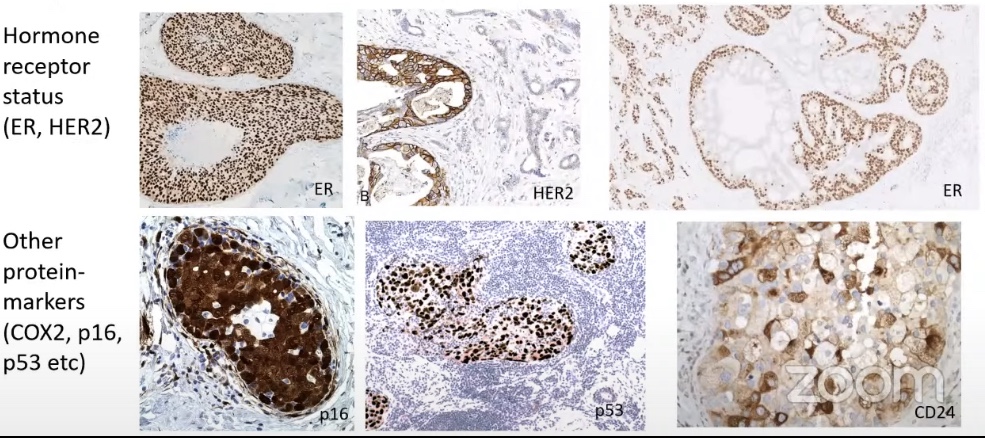
- Protein markers:
- Hormone receptor status:
- ER, PR, HER2
- Nearly all low- and intermediate-grade DCIS are ER-positive
- 50% of high-grade DCIS are ER-negative
- HER2 is amplified in ~34% of DCIS (vs. 13% in invasive cancer) – predominantly in high-grade lesions
- Other protein markers:
- COX2, p16, p53, etc
- The majority of the protein markers correlated with grade:
- But are associated with significant heterogeneity
- ER, PR, HER2
- Hormone receptor status:
- Protein markers:
- At this point in time we do not have a single robust biomarker:
- That can predict the risk of progression of DCIS to IBC
- Can combinations of biomarkers predict the risk of progression (clinico-pathological prediction models)?
- Unclear clinical validity of prediction models combining biomarkers (Schmitz, R. Cancers. 2022):
- They lack of external validation
- They do not include the option of active surveillance
- Unclear clinical validity of prediction models combining biomarkers (Schmitz, R. Cancers. 2022):
- Molecular features suggestive of progression:
- Gene expression analysis:
- Intrinsic subtypes of DCIS:
- Higher frequency of luminal B and HER2 subtypes
- They are NOT prognostic of recurrence in DCIS
- Gene expression differs extensively across tumors:
- No specific gene expression profile exists that can predict progression in DCIS
- Confounded by intrinsic subtypes?
- The intrinsic subtypes are related to different pathways:
- One of the pathways is tumor micro environment
- Intrinsic subtypes of DCIS:
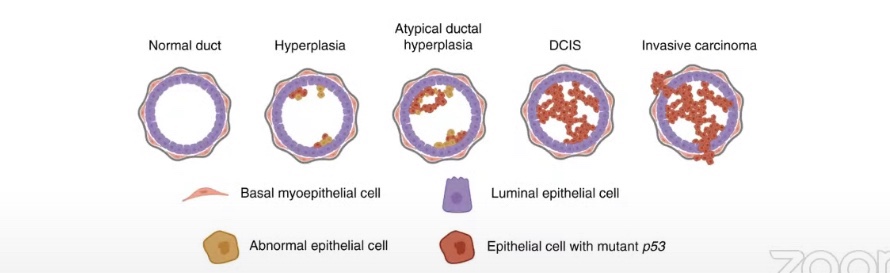
- Genetic alterations:
- There is an increase in genetic alterations in the progression from usual ductal hyperplasia to IBC:
- P53 mutation within the epithelial cell
- DCIS is a genetically advanced lesion with marked intratumoral heterogeneity:
- The higher the grade (grade 3 DCIS / DIN3) the more genetic alterations identified
- There is an increase in genetic alterations in the progression from usual ductal hyperplasia to IBC:
- Gene expression analysis:
- The majority of the studies on molecular analysis in DCIS are describing synchronous alterations:
- They are comparing tumor cells from the DCIS or IBC from the same lesion
- Not subsequent events from the same (untreated) lesion
- In these lesions DCIS and IBC share most genetic mutations and copy number alterations:
- Most common mutations:
- PIK3CA and TP53
- Most common mutations:
- No known genetic mutations can differentiate progressive from indolent DCIS:
- Progression of DCIS varies from patient to patient
- The lack of clear genetic alterations helping us identify progression points us towards:
- Tumor micro environment and stroma
- The lack of clear genetic alterations helping us identify progression points us towards:
- Progression of DCIS varies from patient to patient
- Summary:
- DCIS is a very heterogenous disease
- Biological question is what drives or inhibits progression of DCIS
- The majority of studies describes observations of varying events
- Synchronous DCIS and IBC share most genetic alterations:
- Though not universal, but case to case based
- No known genetic alterations / morphological features can estimate risk of progression:
- Leading interest towards micro environment
- Awaiting active surveillance studies

