- Perioperative Immunotherapy – KEYNOTE-689 Continues to Shape Practice:
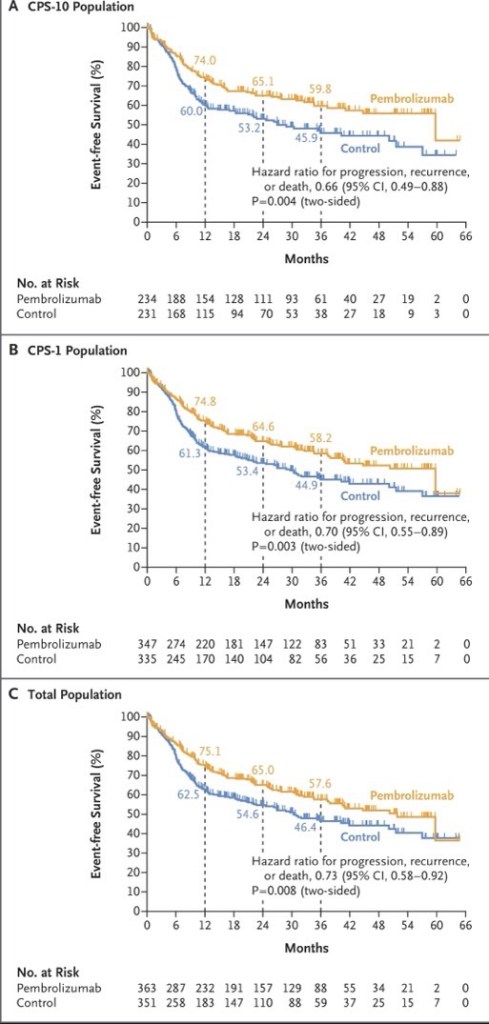
- The KEYNOTE-689 phase 3 trial:
- Which led to the FDA approval of perioperative pembrolizumab (June 2025):
- For resectable locally advanced HNSCC with PD-L1 CPS ≥ 1:
- Remains a central focus
- For resectable locally advanced HNSCC with PD-L1 CPS ≥ 1:
- New ASCO 2026 exploratory analyses demonstrate that the EFS benefit of neoadjuvant / adjuvant pembrolizumab:
- Persists across surgical outcome subgroups, including:
- Patients with and without extranodal extension or positive margins
- Notably, fewer patients in the pembrolizumab arm had ENE or positive margins post-surgery:
- Suggesting neoadjuvant pembrolizumab contributes to pathologic downstaging
- Persists across surgical outcome subgroups, including:
- Which led to the FDA approval of perioperative pembrolizumab (June 2025):
- A pooled meta-analysis of three phase 3 trials (KEYNOTE-689, NIVOPOSTOP, and IMvoke010; n=1,786) presented at ASCO 2026:
- Confirmed a significant improvement in event-free / disease-free survival with perioperative or adjuvant PD-1 / PD-L1 blockade (pooled HR 0.79, 95% CI 0.68–0.91):
- With no meaningful increase in treatment-related deaths
- Confirmed a significant improvement in event-free / disease-free survival with perioperative or adjuvant PD-1 / PD-L1 blockade (pooled HR 0.79, 95% CI 0.68–0.91):
- The KEYNOTE-689 phase 3 trial:
The following figure from the KEYNOTE-689 trial illustrates the event-free survival benefit across PD-L1 subgroups:
- Neoadjuvant Bispecific Antibody Combinations: Ivonescimab Leads the Way:
- Several ASCO 2026 abstracts highlight the emerging role of bispecific antibodies in the neoadjuvant setting:
- Ivonescimab (PD-1 / VEGF bispecific) + nab-paclitaxel / cisplatin:
- Achieved a remarkable 100% ORR:
- 50% CR, 50% PR
- Achieved a 50% pCR rate:
- In 30 surgical patients with resectable LA-HNSCC
- All patients with CPS >30 achieved pCR, and 100% laryngeal / pharyngeal preservation was achieved
- Achieved a remarkable 100% ORR:
- Ivonescimab (PD-1 / VEGF bispecific) + nab-paclitaxel / cisplatin:
- A randomized phase II trial comparing ivonescimab (PD-1 / VEGF), cadonilimab (PD-1 /CTLA-4), and penpulimab (PD-1 alone), each combined with chemotherapy:
- Showed the highest pCR rate with ivonescimab at 60%, compared to 42.1% with cadonilimab and 40% with single-agent PD-1
- Adebrelimab (PD-L1 inhibitor) + chemotherapy demonstrated:
- An 87.5% ORR and a 95.8% larynx preservation rate in resectable LA-HNSCC:
- With all p16-positive and CPS ≥ 20 patients responding
- An 87.5% ORR and a 95.8% larynx preservation rate in resectable LA-HNSCC:
- Several ASCO 2026 abstracts highlight the emerging role of bispecific antibodies in the neoadjuvant setting:
- Novel Agents in Recurrent / Metastatic HNSCC:
- Bispecific antibodies are generating significant excitement in the recurrent / metastatic setting:
- Ficerafusp alfa (EGFR × TGF-β) + pembrolizumab:
- Two-year follow-up data showed a confirmed ORR of 54% in HPV-negative R/M HNSCC (21% CR), with a median DOR of 21.7 months and median OS of 21.3 months
- The phase 2 / 3 FORTIFI-HN01 trial is now actively enrolling
- Two-year follow-up data showed a confirmed ORR of 54% in HPV-negative R/M HNSCC (21% CR), with a median DOR of 21.7 months and median OS of 21.3 months
- Petosemtamab (EGFR × LGR5) + pembrolizumab:
- Updated phase 2 data showed a 60% ORR (including 5 CRs) in first-line PD-L1+ R/M HNSCC, with median DOR of 11 months
- Two phase 3 trials (LiGeR-HN1 and LiGeR-HN2) are recruiting
- Updated phase 2 data showed a 60% ORR (including 5 CRs) in first-line PD-L1+ R/M HNSCC, with median DOR of 11 months
- CRB-701 (Nectin-4 ADC):
- A phase 1 / 2 study in heavily pretreated R/M HNSCC (85% refractory to immunotherapy and platinum):
- Showed a confirmed ORR of 33.3% at both 2.7 and 3.6 mg/kg doses, regardless of HPV status
- A phase 1 / 2 study in heavily pretreated R/M HNSCC (85% refractory to immunotherapy and platinum):
- Becotatug vedotin (EGFR ADC):
- A new randomized phase II trial is evaluating neoadjuvant becotatug vedotin alone or combined with immune checkpoint inhibitors in resectable LA-HNSCC
- Ficerafusp alfa (EGFR × TGF-β) + pembrolizumab:
- Bispecific antibodies are generating significant excitement in the recurrent / metastatic setting:
- HPV-Directed Immunotherapy and De-escalation:
- The TARGET-HPV trial presented at ASCO 2026:
- Evaluated neoadjuvant HB200 (HPV16-specific viral immunotherapy) + carboplatin / paclitaxel in HPV16+ oropharyngeal SCC:
- The deep response rate was 87.9%, with 86% of patients receiving de-escalated definitive therapy
- At 23 months median follow-up, 2-year PFS was 86% and OS was 100%
- Circulating tumor HPV-DNA was significantly associated with recurrence
- Evaluated neoadjuvant HB200 (HPV16-specific viral immunotherapy) + carboplatin / paclitaxel in HPV16+ oropharyngeal SCC:
- The TARGET-HPV trial presented at ASCO 2026:
- Evolving First-Line R / M HNSCC Pipeline:
- A landscape analysis presented at ASCO 2026 identified 145 active regimens (111 unique assets) in the first-line R / M HNSCC pipeline
- Key trends include a shift toward chemotherapy-free combinations alongside PD-1 blockade:
- With bispecific antibodies (10.8%), ADCs (10.8%), and cancer vaccines (9.0%) representing the most common novel modalities
- Eight key phase 3 trials are underway:
- All incorporating PD-1 as a target, with pembrolizumab as the backbone in 7 of 8
- Overall, ASCO 2026 highlights a transformative period in head and neck oncology:
- With perioperative immunotherapy now established as a new standard, bispecific antibodies and ADCs showing compelling early efficacy, and biomarker-driven strategies (PD-L1 CPS, HPV status, ctHPV-DNA, MRD) increasingly guiding treatment selection
References
- Neoadjuvant and Adjuvant Pembrolizumab in Locally Advanced Head and Neck Cancer. Uppaluri R, Haddad RI, Tao Y, et al. The New England Journal of Medicine. 2025;393(1):37-50. doi:10.1056/NEJMoa2415434.
- FDA approves neoadjuvant and adjuvant pembrolizumab for resectable locally advanced head and neck squamous cell carcinoma | FDA. Food and Drug Administration. 2025-06-13.
- Neoadjuvant and adjuvant pembrolizumab (pembro) plus standard of care (SOC) for resectable locally advanced head and neck squamous cell carcinoma (LA HNSCC): Efficacy by surgical outcomes in the phase 3 KEYNOTE-689 trial.. Adkins D, Haddad R, Tao Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6057. doi:10.1200/JCO.2026.44.16_suppl.6057.
- Perioperative or adjuvant PD-1/PD-L1 blockade with curative-intent multimodality therapy for locally advanced head and neck squamous cell carcinoma: A systematic review and meta-analysis of randomized trials.. Daher S, Daher H, Altal H, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):e18074. doi:10.1200/JCO.2026.44.16_suppl.e18074.
- Neoadjuvant ivonescimab (AK112, a PD-1/VEGF bispecific antibody) combined with nab-paclitaxel and cisplatin (AP) for resectable locally advanced head and neck squamous cell carcinoma (LA-HNSCC): An exploratory phase II study.. Kunyu Yang, Xiaomeng Zhang and Lu Wen. Journal of Clinical Oncology. 2026;44(Suppl 16):6014. doi:10.1200/JCO.2026.44.16_suppl.6014.
- Neoadjuvant immunotherapy in combination with chemotherapy in resectable locally advanced head and neck squamous cell carcinoma: Updated efficacy and safety data from a randomized phase II trial.. Liu L, Chen F, Li Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6091. doi:10.1200/JCO.2026.44.16_suppl.6091.
- Neoadjuvant adebrelimab plus chemotherapy in untreated locally advanced head and neck squamous cell carcinoma: Efficacy and biomarker insights from a single-arm phase 2 trial.. Fang R, Lei W, Huang B, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6106. doi:10.1200/JCO.2026.44.16_suppl.6106.
- Ficerafusp Alfa (BCA101) With Pembrolizumab for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: Two-Year Results of an Expansion Cohort of a Phase I/Ib Trial. Hanna GJ, Zandberg DP, Wong DJ, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2026;:JCO2502027. doi:10.1200/JCO-25-02027.
- A multicenter, randomized, double-blind, phase 2/3 study of ficerafusp alfa (BCA101) or placebo in combination with pembrolizumab for first-line treatment of HPV-negative, PD-L1–positive, recurrent or metastatic (R/M) head and neck squamous cell carcinoma (HNSCC): FORTIFI-HN01.. Ferrarotto R, Kaczmar J, Spigel D, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):TPS6129. doi:10.1200/JCO.2026.44.16_suppl.TPS6129.
- Petosemtamab (MCLA-158) with pembrolizumab as first-line (1L) treatment of PD-L1+ recurrent/metastatic (r/m) head and neck squamous cell carcinoma (HNSCC): Phase 2 trial. Herpen C, Daste A, Arrazubi V, et al. Journal of Clinical Oncology. 2025;43(Suppl 16):6024. doi:10.1200/JCO.2025.43.16_suppl.6024.
- LiGeR-HN Phase III Trials of Petosemtamab + Pembrolizumab and Petosemtamab Monotherapy in Recurrent or Metastatic HNSCC. Machiels JP, Fayette J, Haddad R, et al. Future Oncology (London, England). 2025;21(16):2007-2016. doi:10.1080/14796694.2025.2511470.
- A phase 1/2 study of the next-generation nectin-4–targeting antibody-drug conjugate CRB-701 (SYS6002) in patients with recurrent or metastatic head and neck squamous cell carcinoma.. Mantia C, Hanna G, Loriot Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6062. doi:10.1200/JCO.2026.44.16_suppl.6062.
- A randomized, non-comparative, multicenter phase II trial of neoadjuvant becotatug vedotin alone or combined with immune checkpoint inhibitors (penpulimab/ivonescimab) in resectable locally advanced head and neck squamous cell carcinoma.. Wei X, Xiang Z, Zeng Y, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):TPS6135. doi:10.1200/JCO.2026.44.16_suppl.TPS6135.
- Neoadjuvant HPV16-specific viral immunotherapy (HB200) plus chemotherapy with response-adapted de-escalation in HPV16+ oropharyngeal squamous cell carcinoma: TARGET-HPV trial.. Rosenberg A, Juloori A, Cursio J, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):6097. doi:10.1200/JCO.2026.44.16_suppl.6097.
- Emerging trends in research strategies in the first-line recurrent or metastatic head and neck cancer (R/M SCCHN) landscape: A top-level analysis by Oncofocus.. Shukla A, Keeshara V, Chamaria M, et al. Journal of Clinical Oncology. 2026;44(Suppl 16):e18029. doi:10.1200/JCO.2026.44.16_suppl.e18029.
- Recent Highlights and Breakthroughs in Immunotherapy for Head and Neck Cancers. Vuille JA, Szturz P. Current Opinion in Oncology. 2026;38(3):201-211. doi:10.1097/CCO.0000000000001211.
- Immunotherapy in Locally Advanced Head and Neck Squamous Cell Carcinoma: The Current Status and Future Outlook. Köylü B, Selçukbiricik F, Aksoy S, Güven DC. Critical Reviews in Oncology/Hematology. 2026;:105145. doi:10.1016/j.critrevonc.2026.105145.

