- Failure to identify a parathyroid gland during cervical exploration:
- Is most commonly explained by:
- Ectopic location rather than true absence
- Is most commonly explained by:
- Large anatomic and surgical series demonstrate that approximately 15% to 16% of parathyroid glands are ectopic:
- With predictable distributions:
- Based on embryologic origin (Taterra et al., Surg Radiol Anat, 2019):
- Consequently, a structured search strategy:
- Guided by embryology and prevalence data is recommended
- Consequently, a structured search strategy:
- Based on embryologic origin (Taterra et al., Surg Radiol Anat, 2019):
- With predictable distributions:
- General intra-operative principles:
- Careful inspection of the orthotopic field:
- Is mandatory before declaring a gland ectopic
- Approximately 80% to 90% of parathyroid glands are located within a few millimeters of the posterior thyroid capsule (Taterra et al., 2019):
- Gentle subcapsular dissection along the posterior surface of the thyroid should be completed before expanding the field
- Careful inspection of the orthotopic field:
- Intrathyroidal parathyroid glands:
- Account for 2% to 3% of all glands and up to 20% to 22% of ectopic glands, particularly inferior glands (Phitayakorn & McHenry, Am J Surg, 2006):
- For this reason, inspection and palpation of the thyroid specimen is considered standard practice in experienced centers (Noussios et al., Exp Clin Endocrinol Diabetes, 2012)
- Account for 2% to 3% of all glands and up to 20% to 22% of ectopic glands, particularly inferior glands (Phitayakorn & McHenry, Am J Surg, 2006):
- Reoperative series demonstrate that most “missed” glands:
- Are found in standard embryologic locations:
- Most commonly the tracheoesophageal groove, thyrothymic ligament, or superior mediastinum:
- Emphasizing the importance of a systematic rather than random exploration (Silberfein et al., Arch Surg, 2010)
- Most commonly the tracheoesophageal groove, thyrothymic ligament, or superior mediastinum:
- Are found in standard embryologic locations:
- Superior parathyroid gland – Evidence-Based search pattern:
- Typical location:
- Superior parathyroid glands:
- Fourth pharyngeal pouch origin:
- Exhibit limited migration and are therefore relatively constant in position
- Fourth pharyngeal pouch origin:
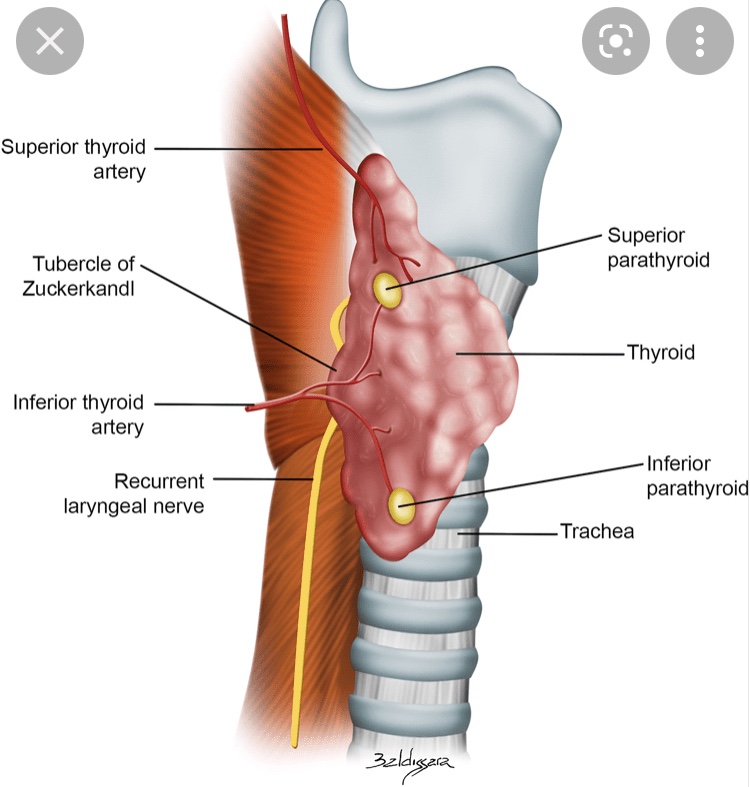
- They are typically located on the posterior aspect of the upper thyroid pole:
- Approximately 1 cm above the intersection of the recurrent laryngeal nerve (RLN) and the inferior thyroid artery:
- Frequently within the tracheoesophageal groove (Scharpf et al., Surg Oncol Clin N Am, 2016)
- Approximately 1 cm above the intersection of the recurrent laryngeal nerve (RLN) and the inferior thyroid artery:
- Superior parathyroid glands:
- Common ectopic locations:
- When ectopic:
- Superior parathyroid glands are most often displaced posteriorly, rather than inferiorly:
- Tracheoesophageal or para-esophageal groove the most common ectopic site for superior glands (Noussios et al., 2012; Taterra et al., 2019)
- Retro-esophageal or retro-pharyngeal space, particularly in undescended glands (Scharpf et al., 2016)
- Posterior mediastinum, where enlarged glands may descend along the esophagus but remain posterior in relation to the RLN (Phitayakorn & McHenry, 2006)
- Superior parathyroid glands are most often displaced posteriorly, rather than inferiorly:
- When ectopic:
- Stepwise surgical approach:
- If a superior gland is not identified in its orthotopic location, the recommended sequence is:
- Systematic exploration of the tracheoesophageal groove following the RLN superiorly
- Blunt dissection of the para- and retro-esophageal spaces
- Evaluation of the high posterior neck for undescended glands
- Inspection of the thyroid specimen for an intrathyroidal gland (Noussios et al., 2012; Silberfein et al., 2010)
- If a superior gland is not identified in its orthotopic location, the recommended sequence is:
- Typical location:
- Inferior parathyroid gland – evidence-based search pattern:
- Typical location:
- Inferior parathyroid glands:
- Third pharyngeal pouch origin
- Descend with the thymus and demonstrate significantly greater variability
- Orthotopically, they are most often located near the lower thyroid pole, anterior to the RLN, frequently within or adjacent to the thyrothymic ligament (Scharpf et al., 2016)
- Inferior parathyroid glands:
- Common ectopic locations:
- Inferior glands account for the majority of ectopic parathyroids:
- Intrathymic or within the cervical thymus:
- Approximately 30% of ectopic inferior glands (Phitayakorn & McHenry, 2006)
- Anterosuperior mediastinum, often contiguous with thymic tissue (Noussios et al., 2012)
- Intrathyroidal:
- Accounting for ~ 20% to 22% of ectopic inferior glands (Phitayakorn & McHenry, 2006)
- High cervical or carotid sheath locations, representing failed embryologic descent (Noussios et al., 2012)
- Intrathymic or within the cervical thymus:
- Inferior glands account for the majority of ectopic parathyroids:
- Stepwise surgical approach:
- When an inferior gland is not identified at the lower pole:
- The thyrothymic ligament should be followed inferiorly toward the thymus
- A limited cervical thymectomy should be performed when clinically appropriate:
- Given the high incidence of intrathymic glands
- The lower thyroid pole and specimen should be inspected for intrathyroidal tissue
- The carotid sheath and high cervical region should be explored in cases suspicious for undescended glands (Phitayakorn & McHenry, 2006; Silberfein et al., 2010)
- When an inferior gland is not identified at the lower pole:
- Typical location:
- Lessons from re-operative surgery:
- In contemporary re-operative parathyroidectomy series, previously missed glands were most commonly located in the:
- Tracheoesophageal groove
- Thyrothymic ligament
- Superior mediastinum
- Confirming that failure is usually related to incomplete exploration of predictable embryologic sites rather than unusual anatomy (Silberfein et al., Arch Surg, 2010)
- In contemporary re-operative parathyroidectomy series, previously missed glands were most commonly located in the:
- Key references:
- Taterra D, et al. The prevalence and anatomy of parathyroid glands: a meta-analysis. Surg Radiol Anat. 2019.
- Phitayakorn R, McHenry CR. Incidence and location of ectopic abnormal parathyroid glands. Am J Surg. 2006;191:418–423.
- Noussios G, et al. Ectopic parathyroid glands and their anatomical, clinical and surgical implications. Exp Clin Endocrinol Diabetes. 2012.
- Silberfein EJ, et al. Reoperative parathyroidectomy: location of missed glands. Arch Surg. 2010.
- Scharpf J, et al. Anatomy and embryology of the parathyroid glands. Surg Oncol Clin N Am. 2016.