- Definition:
- Triple negative breast cancer (TNBC) is a subtype of breast tumor lacking hormone receptors expression and HER2 gene amplification:
- Represents 24 % of newly diagnosed breast neoplasms
- TNBC is usually characterized by poor prognosis and lack of wide choice therapeutic agents due to the absence of targetable hormone receptors and HER2 expression:
- Therefore is considered a very interesting and challenging topic for breast cancer research
- TNBC is a functional term that defines a wide spectrum of entities:
- With different biology and clinical behavior, with marked genetic, transcriptional, histologic and clinical differences
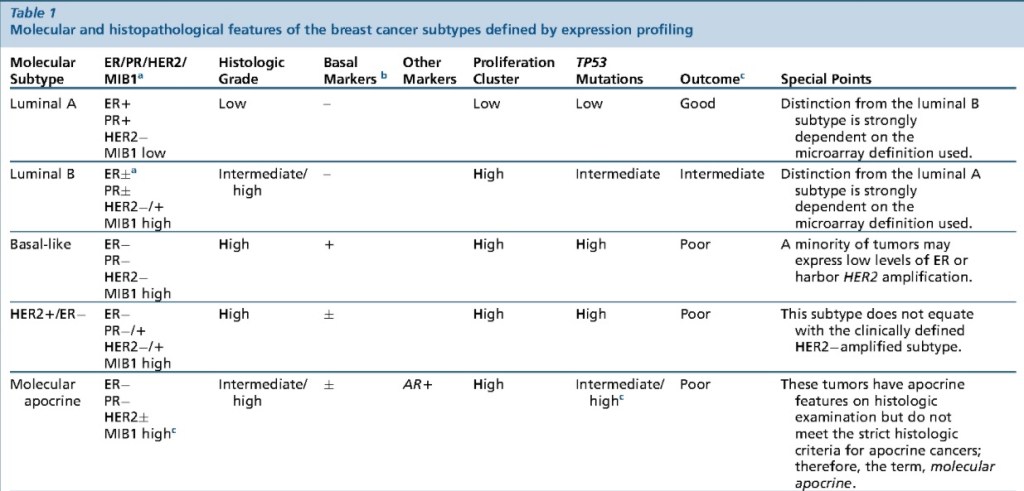
- The definition of a new classification for breast cancer based on its gene expression pattern divided breast tumors into four “intrinsic subtypes”:
- Luminal subtype:
- Divided in Luminal A and Luminal B:
- Characterized by estrogen receptor gene expression
- Divided in Luminal A and Luminal B:
- The HER2 subtype:
- Characterized by HER2 gene amplification
- The so-called basal-like subtype:
- A particular breast cancer showing positivity for basal and myoepithelial markers and lack of hormone receptors and HER2 gene amplification
- “Normal breast-like” subtype:
- With triple-negative phenotype but cellular derivation typical of normal breast epithelium
- Notably, both the basal-like and normal breast-like subtypes were already recognized as triple negative
- Luminal subtype:
- Triple negative breast cancer (TNBC) is a subtype of breast tumor lacking hormone receptors expression and HER2 gene amplification:
- All breast cancers arise in the terminal duct lobular units (the functional unit of the breast) of the collecting duct
- The histological and molecular characteristics:
- Have important implications for therapy:
- Several classifications on the basis of molecular and histological characteristics have been developed
- Have important implications for therapy:
- The histological subtypes described here (Figure) are the
most frequent subtypes of breast cancer:- Ductal carcinoma (now referred to
as ‘no special type’ (NST)) and lobular carcinoma:- Are the invasive lesions
- Their pre-invasive counterparts are:
- Ductal carcinoma in situ and lobular carcinoma in situ (or lobular neoplasia), respectively
- The intrinsic subtypes of Perou and Sorlie:
- Are based on a 50-gene expression signature (PAM50)
- The surrogate intrinsic subtypes are typically used clinically and are based on histology and
immunohistochemistry expression of key proteins:- Estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2
(HER2) and the proliferation marker Ki-67
- Estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2
- Tumors expressing ER and / or PR are termed ‘hormone receptor-positive’
- Tumors not expressing ER, PR and HER2 are called ‘triple-negative’
- The intrinsic subtypes of Perou and Sorlie:
- Ductal carcinoma in situ and lobular carcinoma in situ (or lobular neoplasia), respectively
- Ductal carcinoma (now referred to
- The normal breast terminal duct lobular unit:
- It is formed by two layers:
- Inner or luminal layer (epithelial cell layer)
- Outer or basal layer (myoepithelial cell layer)
- It is formed by two layers:

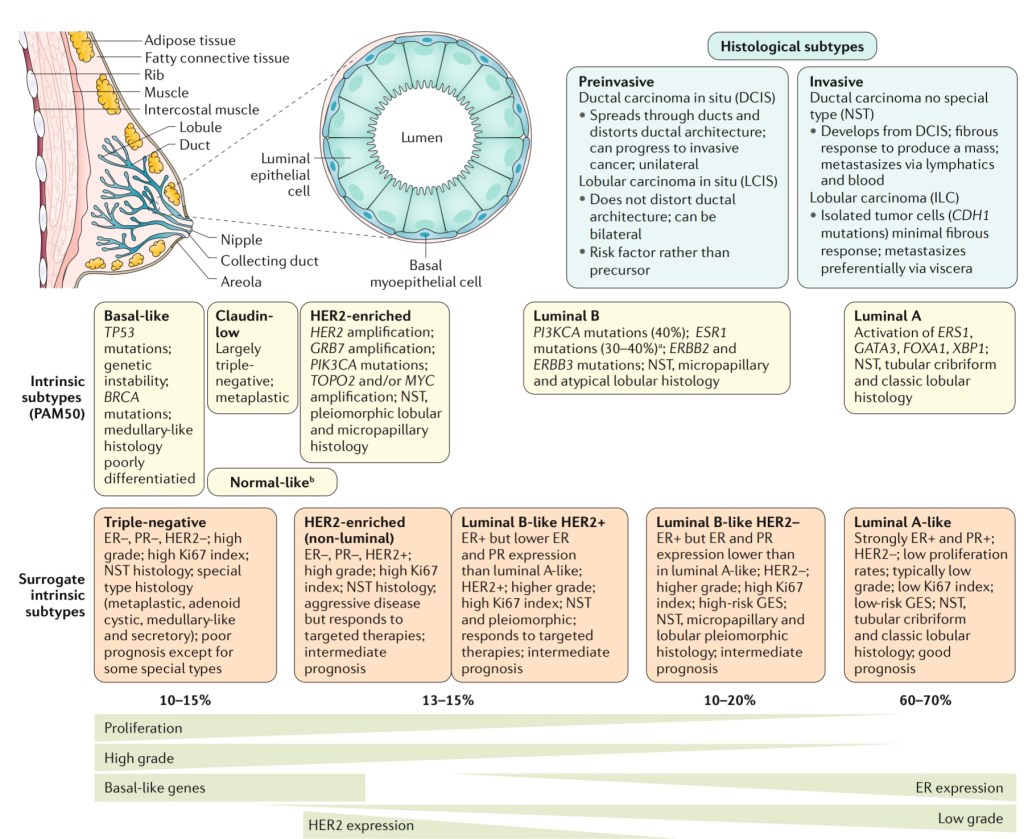
- Molecular subtypes that are triple negative:
- Basal-like:
- TP53 mutations
- Genetic Instability
- BRCA mutations
- Medullary-like histology
- Poorly differentiated
- Claudin-low:
- Largely triple negative
- Metaplastic
- Normal breast-like
- Molecular apocrine
- Interferon rich
- Basal-like:


- TNBC can be classified into:
- Low-grade and high-grade histologic types
- Several histologic types of low-grade TNBC, including:
- Salivary gland-like tumors of the breast and solid papillary carcinoma with reverse polarity:
- Are underpinned by specific / pathognomonic genetic alterations
- In contrast, acinic cell carcinoma and high-grade variants of TNBC have somatic genomic landscape similar to those of conventional TNBC
- Low- grade variants of metaplastic breast carcinomas (MBCs) are unlikely to be underpinned by specific genetic alterations; however, the genetic analyses performed to date included only a few or single cases
- Progression to high-grade TNBC has been described in most low-grade forms of TNBC:
- However, it occurs at a different rate
- Whereas fairly common in acinic cell carcinoma, it is a rare event in the salivary gland-like tumors of the breast and solid papillary carcinoma with reverse polarity
- It should be noted that evidence for the presence of PRKD1 E710D mutations or PRKD1/2/3 rearrangements in polymorphous carcinoma of the breast remains to be documented
- Salivary gland-like tumors of the breast and solid papillary carcinoma with reverse polarity:

