Invasive Lobular Carcinoma of the Breast
- Invasive lobular carcinoma:
- Is the most common special histological subtype of invasive breast carcinoma
- From an evolutionary point of view:
- These tumors arise from a family of non-obligate precursor lesions called:
- Atypical lobular hyperplasia (ALH) and lobular carcinoma in situ (LCIS):
- Which may be collectively termed:
- Lobular neoplasia (LN)
- Which may be collectively termed:
- Atypical lobular hyperplasia (ALH) and lobular carcinoma in situ (LCIS):
- These tumors arise from a family of non-obligate precursor lesions called:
- Even within this narrow spectrum of pre-invasive lesions and frank invasive carcinoma:
- There is significant morphological and biological heterogeneity
- The multistep model of breast cancer progression:
- Contends that although lobular carcinomas:
- Arise along the low-grade, ER-positive arm of the pathway (with low-grade, ER-positive ductal lesions):
- De-differentiation to higher grade lesions:
- Can occur through acquisition of alterations in oncogenes such as:
- ERBB2 and TP53:
- Producing a spectrum of heterogenous proliferations
- ERBB2 and TP53:
- Can occur through acquisition of alterations in oncogenes such as:
- De-differentiation to higher grade lesions:
- Arise along the low-grade, ER-positive arm of the pathway (with low-grade, ER-positive ductal lesions):
- Contends that although lobular carcinomas:
- Lobular neoplasia (LN):
- Are mostly an incidental finding:
- Comprise neoplastic proliferation of characteristically discohesive cells:
- Which fill and distend the terminal duct lobular units
- Comprise neoplastic proliferation of characteristically discohesive cells:
- LN encompasses both:
- ALH and LCIS:
- The boundary between the two is defined by:
- An arbitrary cut-off using a quantitative measure:
- Depending on the relative extent of involvement of the terminal duct lobular unit (TDLU):
- If more than 50% of the TDLU is occupied:
- The lesion is upgraded to LCIS
- If more than 50% of the TDLU is occupied:
- Depending on the relative extent of involvement of the terminal duct lobular unit (TDLU):
- An arbitrary cut-off using a quantitative measure:
- The boundary between the two is defined by:
- LN is considered to be a:
- Non-obligate precursor of invasive cancer with:
- ALH associated with a:
- 4 to 5 times increased relative risk for subsequent cancer
- ALH associated with a:
- LCIS associated with a:
- 8 to 10 times increased relative risk for subsequent cancer:
- The risk is bilateral:
- But predominates for the ipsilateral breast
- The risk is bilateral:
- 8 to 10 times increased relative risk for subsequent cancer:
- Non-obligate precursor of invasive cancer with:
- ALH and LCIS:
- Are mostly an incidental finding:
- Classic invasive lobular carcinoma (ILC):
- Typically demonstrates:
- Single cell infiltration and a characteristic targetoid pattern of growth with minimal associated stromal response
- This pattern of subtle invasion:
- Is such that the size of the tumor often exceeds the imaging findings:
- And obtaining clear surgical margins may be challenging
- Is such that the size of the tumor often exceeds the imaging findings:
- Although ILCs are generally palpable:
- A high false-negative mammography rate is possible:
- In 19% to 43%
- A high false-negative mammography rate is possible:
- In addition to the classic form of ILC:
- Which is typically histological grade 2:
- There are special morphological subtypes including:
- Pleomorphic
- Solid
- Alveolar
- Tubulo-lobular
- There are special morphological subtypes including:
- These variants are rarely seen as pure form:
- And are more likely to be present with the classical type
- Which is typically histological grade 2:
- Typically demonstrates:
- ILC and its subtypes are typified by:
- A loss of cellular adhesion:
- Frequently the result of biallelic inactivation (i.e. gene mutation combined with gene deletion) of the CDH1 gene:
- Encoding E-cadherin:
- Although other mechanisms of expression loss also feature
- Encoding E-cadherin:
- Frequently the result of biallelic inactivation (i.e. gene mutation combined with gene deletion) of the CDH1 gene:
- A loss of cellular adhesion:
- ILCs are normally estrogen (ER) and progesterone (PR) receptor positive:
- And as such patients are indicated for hormone therapy
- Whilst the biological characteristics of ILC afford patients a good prognosis in the short term:
- It has become clear that the longer-term prognosis of ILC is frequently worse than for patients with the more commonly diagnosed invasive breast carcinoma of no special type (IBC-NST; invasive ductal carcinoma, IDC)
- The metastatic presentation of ILC:
- Has long been considered unique:
- With a predilection for common sites (liver, lung, bone), but also gastrointestinal and gynecological sites of colonization:
- Recent studies further support this:
- Inoue et al. showed that lung metastases were less prevalent:
- But peritoneal metastases are significantly higher in ILC (assumed predominantly classic ILC) compared to ER-positive IBC-NST
- A recent study of metastatic spread to gynecological site:
- Demonstrated an association with ILC and young age at diagnosis and confirmed earlier reports of the wide metastatic colonization of ILC
- Inoue et al. showed that lung metastases were less prevalent:
- Recent studies further support this:
- Immunophenotyping:
- Showed a heterogeneous interplay between:
- Hormone receptors and their co-factors during progression, including:
- Frequent downregulation of PR expression and variable changes between AR, GATA3, and FOXA1 seen in different metastases within the same patient
- Hormone receptors and their co-factors during progression, including:
- Showed a heterogeneous interplay between:
- With a predilection for common sites (liver, lung, bone), but also gastrointestinal and gynecological sites of colonization:
- Has long been considered unique:
- Rarer presentations are increasingly being published in the literature:
- Further highlighting the peculiar natural history of ILC:
- For example, numerous case reports of ILC seeding as orbital metastases appear to suggest these are more likely to arise from an ILC than other types, and in a sole example of a mixed ductal-lobular carcinoma, only the lobular component was found in the orbital metastasis
- Further highlighting the peculiar natural history of ILC:
- The WHO Classificationrecognizes three variants of LCIS:
- Classic (CLCIS)
- Pleomorphic (PLCIS)
- Florid (FLCIS)
- The defining features of both PLCIS and FLCIS have recently been clarified:
- PLCIS:
- Is characterized by cells with enlarged nuclei (4× size of lymphocytes) or similar cytological features to those seen in high-grade ductal carcinoma in situ (DCIS)
- PLCIS:
- FLCIS:
- Is characterized by confluent expansive growth, and there must be marked distention of involved acini with little intervening stroma or an expanded acinus or duct approximately 40 to 50 cells in diameter
- PLCIS is therefore characterized by its degree of cytological atypia:
- Whereas FLCIS describes an architectural pattern (confluent, mass-like growth) with proliferation that is of classic type (CLCIS)
- Unlike CLCIS, PLCIS and FLCIS are more likely to have:
- Comedo-necrosis and calcifications and hence clinical and radiological presentations
- CLCIS:
- Is invariably ER and PR positive, and HER2 negative
- FLCIS exhibits a similar phenotype:
- Although may occasionally be HER2 positive
- PLCIS exhibits a more varied phenotype:
- With less frequent hormone receptor positivity, and an increased likelihood for HER2 overexpression:
- Particularly in the apocrine-type of PLCIS as well as a higher proliferative index
- With less frequent hormone receptor positivity, and an increased likelihood for HER2 overexpression:
- The natural history of PLCIS and FLCIS:
- Is as yet not well understood, and as such, relative risk of progression to frank invasive disease remains unclear, and we await long-term outcome data
- An accumulating volume of work has investigated the molecular characteristics of CLCIS and these special subtypes:
- The application of genomic technologies (copy number profiling, whole exome and targeted panel sequencing):
- To a large set of LCIS confirmed that these lesions were frequently:
- Clonally related to other more malignant lesions found to co-occur in the same specimen (i.e. DCIS and ILC):
- And that intralesion molecular heterogeneity was also identified within LCIS:
- Particularly among those lesions clonally related to DCIS and / or ILC
- And that intralesion molecular heterogeneity was also identified within LCIS:
- Clonally related to other more malignant lesions found to co-occur in the same specimen (i.e. DCIS and ILC):
- To a large set of LCIS confirmed that these lesions were frequently:
- The data further supports the idea that:
- LCIS shares molecular characteristics with its invasive counterpart:
- Suggesting they do indeed have a common clonal origin:
- And that LCIS is a non-obligate precursor of ILC
- Suggesting they do indeed have a common clonal origin:
- Considerable genomic diversity may arise in LCIS whilst the lesion is still confined within the ductal architecture:
- Accounting for some of the morphological and biological variability observed on the progression to invasive cancer
- Some of this intralesional LCIS heterogeneity:
- Accounts for the occurrence of PLCIS and FLCIS
- There is a striking similarity in the genomic profiles of CLCIS, PLCIS, and FLCIS (and invasive tumors):
- With recurrent gains of 1q and losses on 16q and CDH1 mutations:
- Suggesting they arise from a common etiology
- With recurrent gains of 1q and losses on 16q and CDH1 mutations:
- FLCIS and PLCIS with apocrine differentiation:
- Are more genomically complex than CLCIS and non-apocrine PLCIS:
- With an increase in the number of amplifications, genomic losses, and breakpoints
- Are more genomically complex than CLCIS and non-apocrine PLCIS:
- An increased frequency of ERBB2 / HER2 mutations or amplifications:
- Has been reported in PLCIS compared to classic LCIS
- LCIS shares molecular characteristics with its invasive counterpart:
- The application of genomic technologies (copy number profiling, whole exome and targeted panel sequencing):
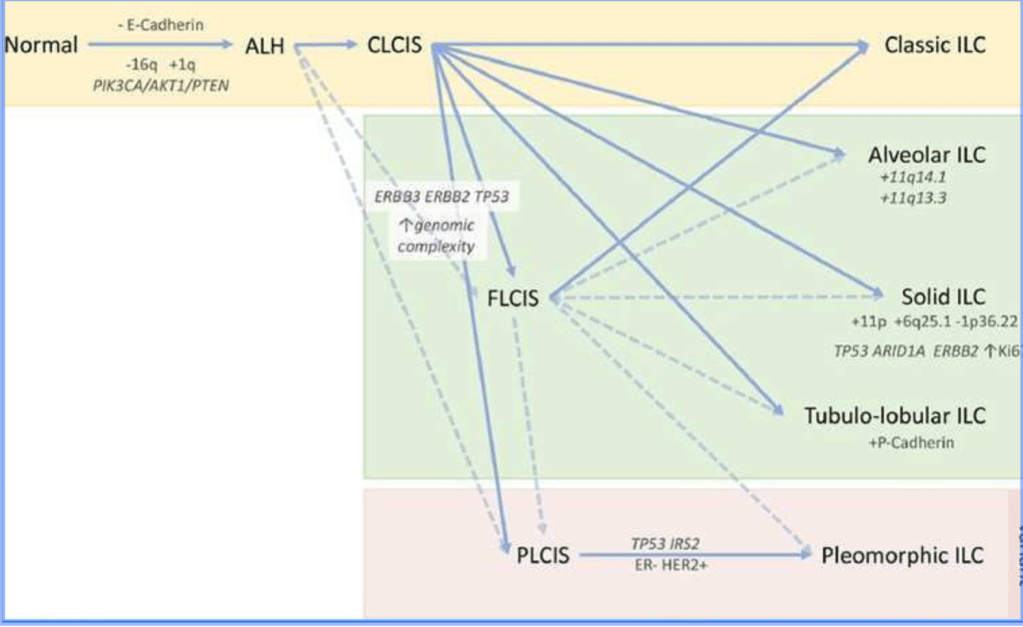
A lineage of ‘lobular’ disease evolves from a normal epithelial cell on a background of a loss of E-cadherin expression and function, and key early somatic alterations involving gain of chromosome 1q, loss of 16q, and mutations in PIK3CA, AKT1, or PTEN.
The morphological and molecular diversity of in situ and invasive lobular lesions is likely to be a result of the subsequently arising pattern of molecular alterations that drive progression.
Atypical lobular hyperplasia (ALH) is distinguishable from lobular carcinoma in situ (LCIS) based on the extent of proliferation within the lobule.
Pleomorphic LCIS (PLCIS) and florid LCIS (FLCIS) can emerge either from ALH (presumably) or from classic LCIS (CLCIS), with an increasing level of genomic
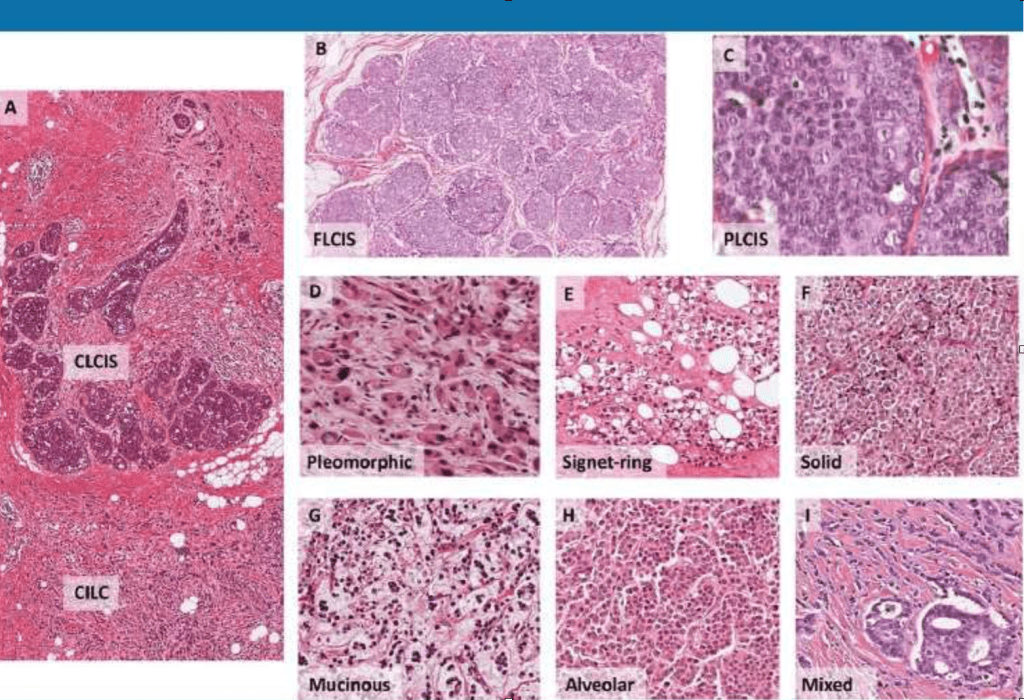
a. CLCIS and CILC (as marked), × 40 magnification.
b. FLCIS shows the cytology of CLCIS with marked distention of lobular units to form a confluent mass-like lesion, × 40 magnification.
c. PLCIS with cytological atypia—nuclear pleomorphism with large vesicular nuclei and nucleoli—at least some × 4 the size of lymphocytes; × 600 magnification.
d. PILC, characteristic discohesion but with high-grade pleomorphic nuclei, with pink, foamy cytoplasm typical of an apocrine phenotype, × 400 magnification.
e. ILC with signet ring cell morphology, × 200 magnification.
f. Solid with sheets of classic type cells, × 200 magnification.
g. ILC showing mucinous / histiocytoid
#Arrangoiz #BreastSurgeon #CancerSurgeon #SurgicalOnologist #MSMC #MountSinaiMedicalCenter #BreastCancer #InvasiveLobularCarcinoma #ILC #LobularNeoplasia #Mexico #Miami
