• Etiology:
• Iodine deficiency:
• Is the most common cause of goiter worldwide
• In mildly and moderately iodine-deficient regions in Denmark:
• Goiter (as determined by ultrasonography) is present in 15% and 22.6% of the population, respectively
• In the United States, where significant iodine deficiency does not exist:
• Multinodular goiter, chronic autoimmune (Hashimoto’s) thyroiditis, and Graves’ disease are more common causes of goiter:
• In older adults, multinodular goiter is most common
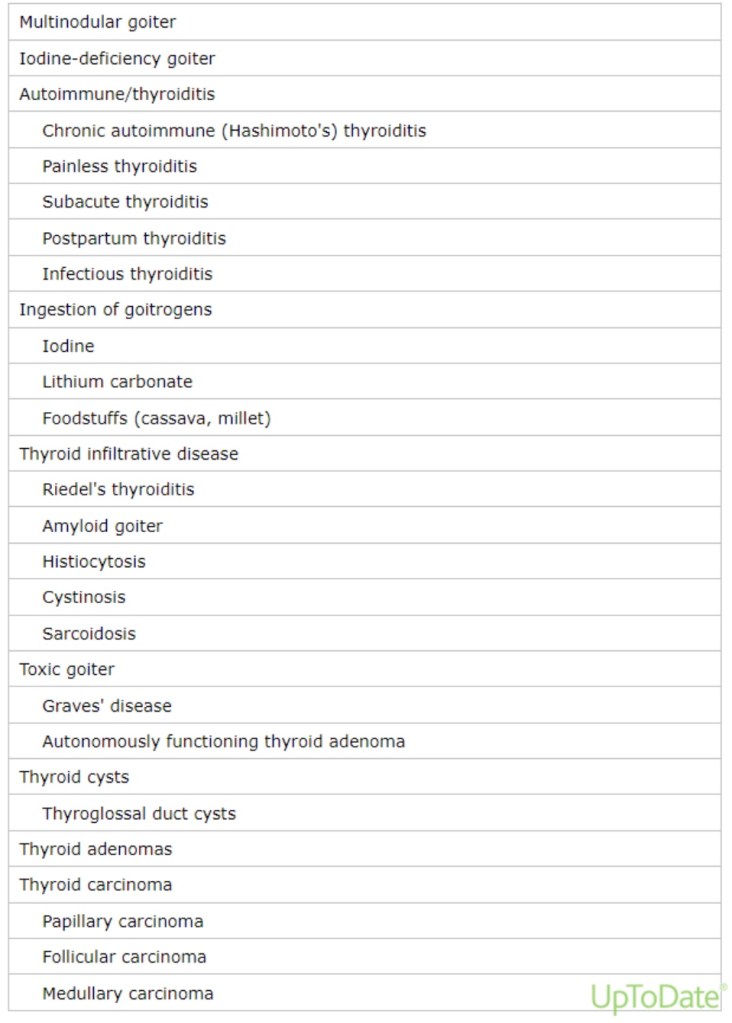
• Other less common causes of goiter include:
• Tumors
• Thyroiditis
• Infiltrative diseases
• The risk of thyroid cancer within a multinodular goiter:
• Is approximately 3% to 5%:
• Similar to the risk in a solitary thyroid nodule
• In a series of 718 patients operated on for goiter in Pakistan:
• 3% of patients were found to have a malignancy
• In a surgical series (with potential selection bias) of 3233 patients with multinodular goiter:
• In which all patients had preoperative ultrasounds and patients who had indeterminate, suspicious, or malignant (Bethesda 3 to 6) preoperative FNA were excluded:
• 31.7% had incidental thyroid cancers:
• Of which 56% were papillary microcarcinomas
• Pathophysiology:
• In patients with iodine deficiency or chronic autoimmune (Hashimoto’s) thyroiditis:
• An increase in thyroid-stimulating hormone (TSH) secretion:
• Is the predominant cause of goiter
• In contrast, most patients with sporadic nontoxic multinodular goiters:
• Have normal serum TSH concentrations:
• In these individuals, the thyroid enlargement is probably caused by several growth factors (including TSH):
• That act over time on thyroid follicular cells:
• That have different synthetic and growth potentials
• There is often a family history of goiter:
• Suggesting that genetic factors may also play a role
• The result is diffuse and later multinodular thyroid enlargement:
• Some nodules eventually become autonomous:
• Due to activating mutations in the TSH receptor or G proteins within the thyroid follicular cells
• The following observations support this sequence of events:
• Thyroid volume is larger in older patients
• The longer the patient has a goiter:
• The larger the size of the goiter
• The larger the size of the goiter:
• The lower the serum TSH concentration
• In patients with Graves’ disease:
• TSH receptor antibodies (TRAb):
• Stimulate the TSH receptor:
• To cause thyroid growth and excessive hormonal secretion