- Introduction:
- PASH may be mistaken for mammary angiosarcoma:
- But is not associated with an increased risk of developing:
- Angiosarcoma
- Invasive ductal carcinoma, or
- Other breast malignancies
- But is not associated with an increased risk of developing:
- There is no indication for genetic counseling or testing:
- Based on a diagnosis of PASH
- Excisional biopsy is not required:
- With concordant and benign findings on mammography and core biopsy
- PASH may be mistaken for mammary angiosarcoma:
- Pseudoangiomatous stromal hyperplasia (PASH):
- Is a benign proliferative breast disease that was first described by Vuitch et al.
- This lesion is characterized by:
- A dense, collagenous proliferation of mammary stroma:
- Forming inter-anastomosing capillary-like spaces
- A dense, collagenous proliferation of mammary stroma:
- It is thought that hormonal factors play an important role in PASH:
- According to Anderson et al:
- This lesion represents an important hyper-response to progesterone and estrogen
- According to Anderson et al:
- PASH is a common histological finding in breast biopsy specimens and can also be found in a normal breast:
- That is in association with proliferative or non-proliferative fibrocystic changes:
- But it is rarely a symptomatic lesion
- That is in association with proliferative or non-proliferative fibrocystic changes:
- Clinically, PASH can presents as:
- A solitary firm, mobile, palpable lump
- As multifocal nodules:
- In 60% of cases
- Can be discovered incidentally on imaging
- PASH can be found in:
- Teenage girls as well as in postmenopausal women with or without hormonal therapy replacement
- It is important to recognize this entity because it can be easily confused with:
- Other benign tumors, such as:
- Fibroadenoma
- Phyllode tumor
- With malignant tumors, such as:
- Angiosarcoma
- Other benign tumors, such as:
- Unfortunately, imaging features of PASH are non-specific:
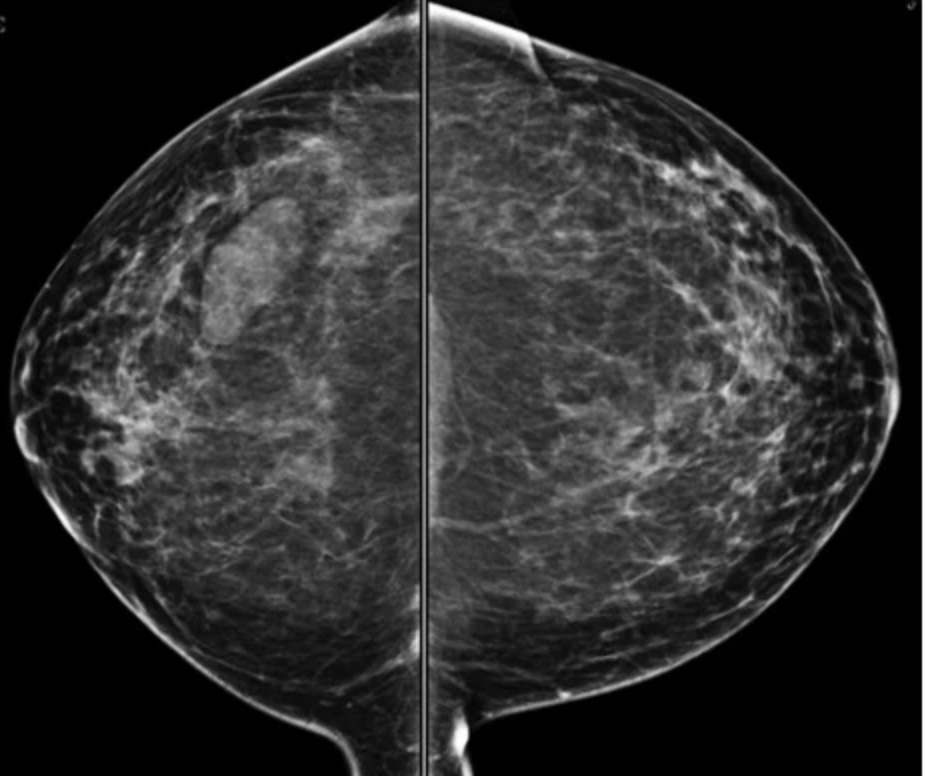
- On mammography:
- The most common appearance described is:
- A well-defined, uncalcified mass, with regular borders
- Spiculated borders, suspicious borders, and architectural distortion can also be seen:
- But are uncommon
- The most common appearance described is:
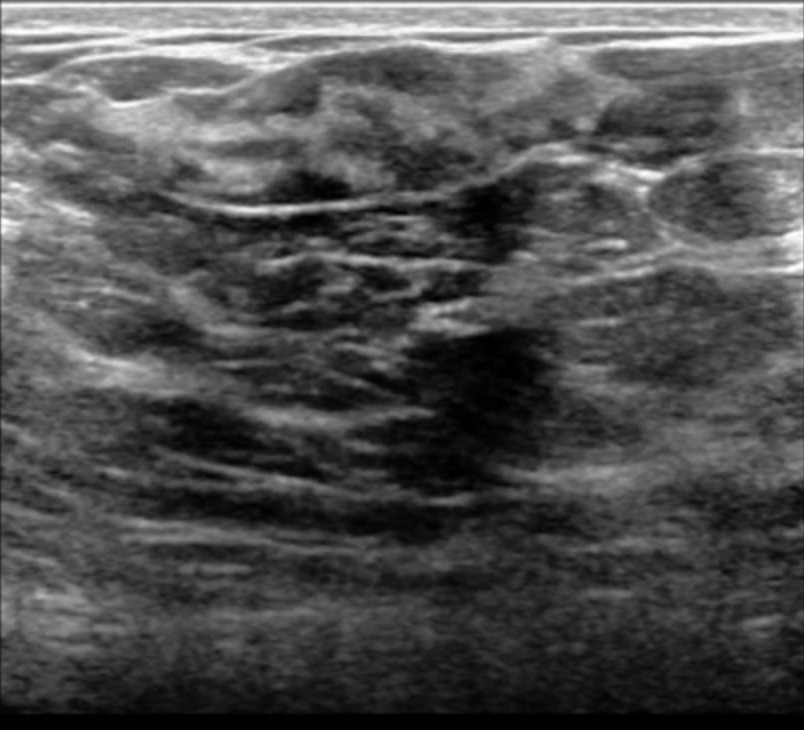
- On ultrasound:
- PASH tends to be:
- An oval, round hypoechoic mass or
- Can presents as a heterogeneous mass with cystic areas
- PASH tends to be:
- According to Cohen et al:
- When a focal lesion with well-defined borders, containing no calcifications on mammography or a well-defined hypoechoic mass on ultrasound is seen:
- PASH can be considered and included in the differential diagnosis
- When a focal lesion with well-defined borders, containing no calcifications on mammography or a well-defined hypoechoic mass on ultrasound is seen:
- On mammography:
- Clinically and on imaging, the differential diagnosis include:
- Fibroadenoma:
- Especially in young patient
- Phyllode tumor:
- In older women
- Fibroadenoma:
- Histologically:
- PASH can be very similar to low-grade angiosarcoma
- Definitive diagnosis is based on histology:
- But unlike low-grade angiosarcoma:
- PASH has no invasive features and contains no necrosis, mitoses, and no destruction of mammary epithelial structures
- But unlike low-grade angiosarcoma:
- Management of PASH depends on presentation:
- When PASH is incidentally discovered or when it is asymptomatic:
- It can be followed up yearly by ultrasound or mammography:
- For a period of 36 months
- It can be followed up yearly by ultrasound or mammography:
- Surgical procedures are indicated for:
- Symptomatic lesion with mechanical complaints
- Pain
- Apprehension for an alternative malignant lesion
- When PASH is incidentally discovered or when it is asymptomatic:
Imaging: bilateral MLO and CC views of the breasts. There is an ovoid mass in the right lower, outer quadrant.

- References:
- Celliers L, Wong DD, Bourke A. Pseudoangiomatous stromal hyperplasia: a study of the mammographic and sonographic features. Clin Radiol. 2010;65(2):145-149.
- Guray M, Sahin AA. Benign breast diseases: classification, diagnosis, and management. Oncologist. 2006;11(5):435-439.
- Hargaden GC, Yeh ED, Georgian-Smith D, Moore RH, Rafferty EA, et al. Analysis of the mammographic and sonographic features of pseudoangiomatous stromal hyperplasia. AJR Am J Roentgenol. 2008;191(2):359-363.
- Salvador R, Lirola JL, Domínguez R, López M, Risueño N. Pseudo-angiomatous stromal hyperplasia presenting as a breast mass: imaging findings in three patients. Breast. 2004;13(5):431-435.
#Arrangoiz #BreastSurgeon #BreastCancer #CancerSurgeon #Teacher #SurgicalOncologist #Mexico #Miami #PASH #PseudoangiomatousStromalHyperplasia
