- Introduction:
- Infectious thyroiditis is also known as:
- Acute thyroiditis
- Suppurative thyroiditis
- Bacterial thyroiditis
- Pyogenic thyroiditis
- Bacterial infections of the thyroid are extremely rare:
- With only:
- 224 cases having been reported in the literature from 1900 to 1980 (adult literature)
- 60 cases reported in the pediatric literature
- Bacterial infections:
- Are the most common causes of infectious thyroiditis
- The infections are generally:
- Suppurative and acute
- With only:
- Infectious thyroiditis caused by:
- Fungal and parasitic infections:
- Are more frequently chronic and indolent
- Fungal and parasitic infections:
- Infectious thyroiditis is also known as:
- Etiology and Pathogenesis:
- The thyroid gland’s high iodine content, significant vascularity, lymphatic drainage as well as its protective capsule:
- Provide the thyroid gland with notable resistance to infection
- The most common predisposing factor to infections of the thyroid appears to be:
- Preexisting thyroid disease has been observed in up to two thirds of women and one half of men with infectious thyroiditis:
- Simple goiter
- Nodular goiter
- Hashimoto’s thyroiditis
- Thyroid carcinoma
- Patients with the acquired immunodeficiency syndrome (AIDS):
- Are a population particularly at risk for bacterial thyroiditis:
- As with other opportunistic infections in AIDS patients, infections of the thyroid gland often are chronic and insidious in onset
- Are a population particularly at risk for bacterial thyroiditis:
- Preexisting thyroid disease has been observed in up to two thirds of women and one half of men with infectious thyroiditis:
- In the adult:
- Staphylococcus aureus and Streptococcus pyogenes are the offending pathogens:
- In more than approximately 80% of patients:
- And are the sole pathogen in over 70% of cases
- In more than approximately 80% of patients:
- Staphylococcus aureus and Streptococcus pyogenes are the offending pathogens:
- In children:
- Alpha- and beta-hemolytic Streptococcus and a variety of anaerobes:
- Account for approximately 70% of cases:
- Whereas mixed pathogens are identified in greater than 50% of cases
- Account for approximately 70% of cases:
- Alpha- and beta-hemolytic Streptococcus and a variety of anaerobes:
- Other thyroidal bacterial pathogens that have been shown to cause infectious thyroiditis include:
- Salmonella brandenburg
- Salmonella enteritidis
- Actinomyces naeslundi
- Actinobacillus actinomycetemcomitans
- Brucella melitensis
- Clostridium septicum
- Eikenella corrodens
- Enterobacter
- Escherichia coli
- Haemophilus influenzae
- Klebsiella sp.
- Pseudomonas aeruginosa
- Serratia marcescens
- Acinetobacter baumannii
- Staphylococcus nonaureus
- Pathogenesis of Acute Suppurative Thyroiditis:
- Bacterial:
- 68% of the cases
- Parasitic:
- 15% of the cases
- Mycobacterial:
- 9% of the cases
- Fungal:
- 5% of the cases
- Syphilitic:
- 3% of the cases
- Bacterial:
- Infection and suppuration may result from:
- Direct spread from a nearby infection
- Via the bloodstream
- Via the lymphatics
- The seminal observation regarding the pathogenesis of bacterial thyroiditis was made in 1979 when Takai et al.:
- Who reported seven cases of infectious thyroiditis:
- Caused by a fistula originating from the left pyriform sinus
- Subsequently, studies involving more than 100 patients with infectious thyroiditis:
- Have identified pyriform sinus fistulae:
- Primarily left-sided, in up to 90% of these patients, especially in those with recurrent episodes
- Have identified pyriform sinus fistulae:
- Who reported seven cases of infectious thyroiditis:
- Additional reports identified as routes of thyroidal infection:
- Infected embryonic cysts from the third and fourth brachial pouches
- Thyroglossal duct cysts
- On pathologic exam:
- The characteristic changes of acute bacterial inflammation, including :
- Necrosis and abscess formation:
- Are commonly found
- Necrosis and abscess formation:
- The characteristic changes of acute bacterial inflammation, including :
- The thyroid gland’s high iodine content, significant vascularity, lymphatic drainage as well as its protective capsule:
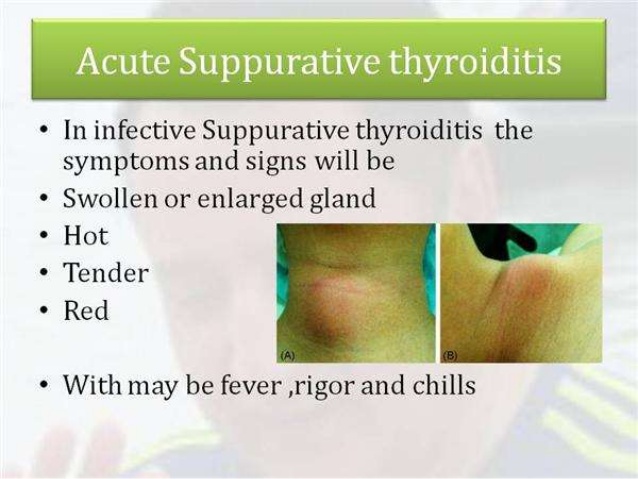
- Clinical Manifestations:
- Bacterial thyroiditis is often preceded by an upper respiratory infection:
- Which may induce inflammation of the fistula and promote the transmission of pathogens to the thyroid.
- Consistent with these observations:
- Bacterial thyroiditis is more common:
- In the late fall and late spring months
- Bacterial thyroiditis is more common:
- Over 90% of patients will present with:
- Thyroidal pain:
- The pain is often referred diffusely to adjacent structures
- Tenderness
- Fever
- Local compression resulting in dysphagia and dysphonia
- Systemic symptoms are frequently seen, such as:
- Fever
- Chills
- Tachycardia
- Malaise
- Thyroidal pain:
- Bacterial thyroiditis is often preceded by an upper respiratory infection:
- Laboratory Findings:
- Thyroid function tests are usually normal:
- However:
- Cases of hypothyroidism and thyrotoxicosis have been reported
- However:
- The polymorphonuclear leukocyte count and the sedimentation rate:
- Are usually elevated
- The organism frequently can be identified by:
- Gram stain and culture of a fine-needle aspiration in the region of suppuration:
- Although sterile cultures are seen in approximately 8% of cases
- Gram stain and culture of a fine-needle aspiration in the region of suppuration:
- Thyroid function tests are usually normal:
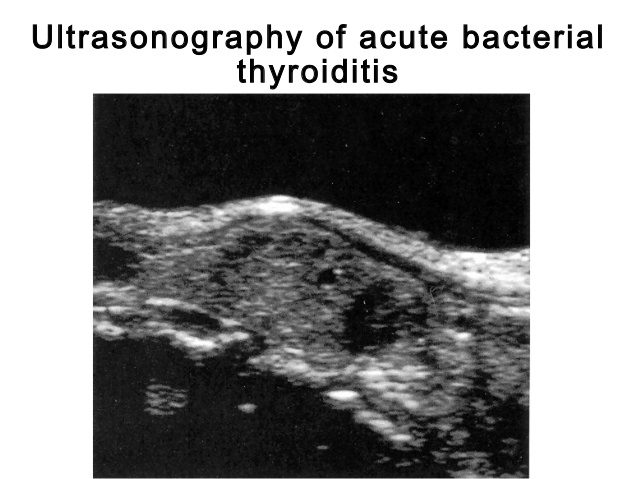
- Imaging:
- A nuclear medicine thyroid scan:
- May show the suppurative region as a “cold” area
- Ultrasound examination may reveal:
- A cystic or “complex” nodule
- A nuclear medicine thyroid scan:
- Diagnosis:
- The diagnosis is made with:
- A fine-needle aspiration
- Gram stain
- Culture
- Symptomatically:
- Infective thyroiditis may be difficult to differentiate from subacute thyroiditis in the early phases:
- Although the characteristic thyroid function changes in the latter disease should be helpful in discriminating the two
- Infective thyroiditis may be difficult to differentiate from subacute thyroiditis in the early phases:
- Leukocytosis and an elevated erythrocyte sedimentation rate are not discriminatory tests:
- As they are commonly observed in both subacute thyroiditis and infectious thyroiditis
- In general:
- Patients with bacterial thyroiditis have a greater febrile response than those with subacute thyroiditis
- Once abscess formation has occurred:
- The local redness, lymphadenopathy, hyperpyrexia, and leukocytosis should lead to the correct diagnosis
- Malignant neoplasms and hemorrhages into cysts:
- May sometimes present with manifestations that mimic this disorder
- The diagnosis is made with:
- Clinical Management:
- The prognosis of bacterial thyroiditis:
- Is often dependent on the prompt recognition and treatment of this disorder:
- As mortality may approach 100%:
- If the diagnosis is delayed and appropriate antimicrobial therapy is not instituted
- As mortality may approach 100%:
- Much depends on the identification of the microorganism:
- From the needle aspirate, incision, and drainage, or occasionally from blood culture
- If no organisms are seen on the Gram stain:
- Nafcillin and gentamicin or a third-generation cephalosporin is the appropriate initial therapy in adults
- A second-generation cephalosporin or clindamycin is reasonable in children
- If an abscess develops and prompt response to antibiotics does not occur:
- Incision and drainage are necessary:
- Sometimes partial lobectomy must be performed,:
- Especially if the disease is recurrent
- Sometimes partial lobectomy must be performed,:
- Incision and drainage are necessary:
- Usually the lesions heal with reasonable speed after initiation of the correct antimicrobial agent, and recurrences are uncommon.
- Mortality from acute bacterial thyroiditis has markedly improved from the 20% to 25% reported in the early 1900s:
- With the extensive review by Berger estimating an overall mortality of 8.6%
- In one review of more than 100 patients, mortality as a complication of acute bacterial thyroiditis was not listed
- Is often dependent on the prompt recognition and treatment of this disorder:
- The prognosis of bacterial thyroiditis:
#Arrangoiz
#Teacher
#Surgeon
#Cirujano
#ThyroidExpert
#ThyroidSurgeon
#CirujanodeTiroides
#ExpertoenTiroides
#ExpertoenParatiroides
#Paratiroides
#Hiperparatiroidismo
#CancerdeTiroides
#ThyroidCancer
#PapillaryThyroidCancer
