Epidemiology
- Invasive lobular carcinoma (ILC) is the second most common histologic form of breast cancer:Comprising 5% to 15% of invasive tumors.
- ILC is pathologically distinct from the much more common invasive ductal carcinoma (IDC):With a unique clinical biology and pathogenesis and resultant implications for diagnosis and treatment.
- The mean age at diagnosis of ILC is 57 years.
- Demonstrated risk factors include:Age at menarche (younger that 12 years)Age at first birth (older than 30 years)
- Hormone therapy:Emphasizing the role of estrogen exposure in disease pathogenesis, which is also observed in most IDCs but shows a more pronounced association in ILC.
- ILC also displays an increased propensity for multifocal / multicentric presentation.
- The incidence of ILC in the Western world over the past decades has corresponded to trends in the use of hormone replacement therapies:With a sharp increase between 1975 and 2000 and a decline between 2000 and 2004:But now with an increasing incidence since 2005 with an unclear etiology.
- Hereditary ILC is rare but may be seen as a secondary tumor in families with hereditary diffuse gastric cancer syndrome:Caused by a germline mutation in the tumor suppressor CDH1 gene.
- ILC otherwise accounts for a small minority of the breast cancers associated with known breast cancer susceptibility genes:Comprising less than 5% of breast cancers in patients with BRCA1 or TP53 mutations and less than 10% of breast cancers in those with BRCA2 mutations.
Molecular Basics and Pathogenesis
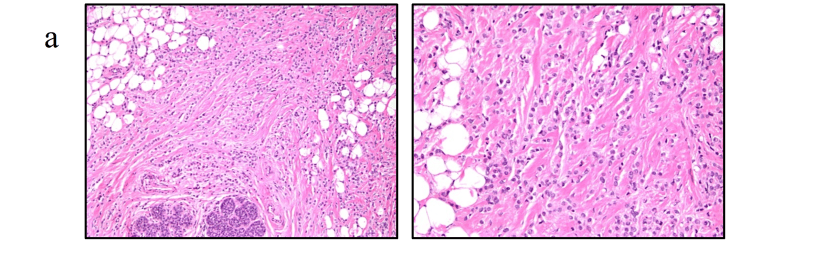
- Classic ILC is characterized by discohesive cells that infiltrate the breast stroma in a distinctive single-file (Indian-file) pattern, with a limited host inflammatory response:
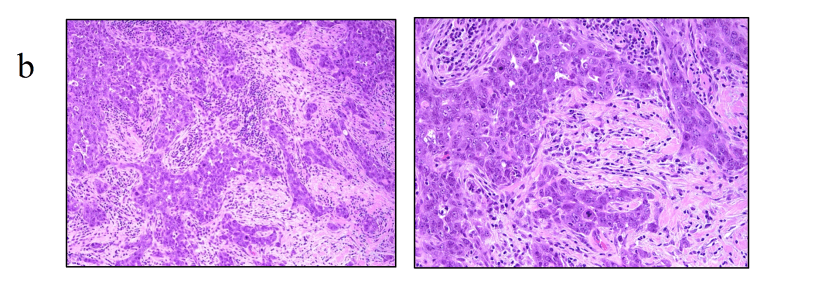
- Several variant (non-classic) forms of ILC have also been described, distinguished by:Morphology:Dispersed
-
- Alveolar
- Solid
- Trabecular
- Mixed
- Cytology:PleomorphicApocrine
- Histiocytoid
- Signet ring
- Tubulolobular
-
- Over 90% of ILCs are estrogen receptor (ER) positive, and at the level of the transcriptome, the majority of ILCs are classified as luminal A:This proportion is observed to be slightly lower in more aggressive ILC variants.
- HER-2 overexpression is rare:Seen in 3% to 5% of classic ILCs:Although it is more frequent in up to 10% of ILC variants:Particularly the pleomorphic subgroup, and recurrent ILCs: The more aggressive biology of the pleomorphic subgroup renders it a unique clinical entity, shown to present at a more advanced stage and more frequently metastasize.
- The tumor biology of ILCs, as with all breast cancers, is of focal importance in both surgical and systemic treatment, as well as long-term outcomes.
- Loss of E-cadherin expression is the most consistently reported hallmark feature of ILC:Seen in 80% to 90% of cases, and is believed to play an early and important role in disease pathogenesis.

- E-cadherin dysregulation originates from mutations in the CDH1 gene on chromosome 16q22.1:Reported to occur at a frequency ranging from 30% to 80% in ILC.
- E-cadherin is a calcium-dependent transmembrane protein that forms a crucial component of adherens-type junctions between epithelial cells, the loss of which predisposes to neoplastic proliferation.2 However, E-cadherin positivity does not, by itself, exclude a lobular neoplasm, and not all ILCs harbor CDH1 gene mutations. Several other novel mutations have recently been identified as more frequent in ILC compared with IDC by comprehensive molecular profiling of 817 breast tumors in The Cancer Genome Analysis (TCGA) study, seen both when comparing all ILCs with IDCs and when limiting comparison with luminal A samples. When comparing all cancers, alterations more frequently seen in ILC included CDH1 (63% in ILC versus 2% in IDC), P1K3CA (48% versus 33%), FOXA1 (7% versus 2%), RUNX1 (10% versus 3%), and TBX3 (9% versus 2%), respectively. Conversely, GATA3 mutations were enriched in IDC (5% in ILC versus 13% in IDC). Importantly, when the analysis was limited to luminal A samples only, several alterations remained significantly more common among luminal A ILCs versus luminal A IDCs, as summarized here
