- When patients are told they have a variant of unknown significance (VUS):
- It can often lead to anxiety and overtreatment
- It is important to counsel patients that a VUS:
- Is not clinically actionable and the majority of VUS are reclassified as benign
- Patients should be counseled to update their genetic counselors:
- As their family history changes and keep contact information up to date as variant reclassification does occur
- The American College of Medical Genetics has recommended that genetic testing classify genetic variants using the following classification schema:
- Deleterious (pathogenic)
- Suspected deleterious (likely pathogenic)
- Variant of Uncertain Clinical Significance
- Genetic variant, favor polymorphism (likely benign)
- Polymorphism (benign)
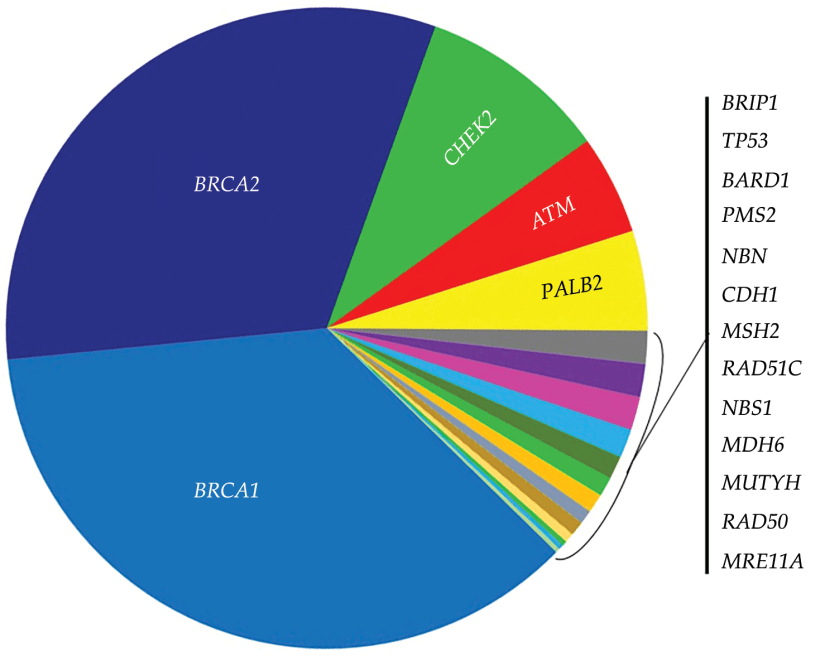
- While deleterious and suspected deleterious BRCA mutations:
- Are known to be associated with an increased risk of breast and ovarian cancer:
- Among breast cancer patients:
- It is estimated that 2% to 6% carry a BRCA 1 / 2 mutation
- Among epithelial ovarian cancer patients:
- It is estimated that 10% to 15% carry a BRCA 1 / 2 mutation
- The lifetime risk of breast cancer for BRCA 1 / BRCA 2 mutation carriers:
- Is approximately 45% to 80%
- The lifetime ovarian cancer risk is:
- 45% to 60% for BRCA 1 mutation carriers
- 11% to 35% for BRCA 2 mutation carriers
- Among breast cancer patients:
- Are known to be associated with an increased risk of breast and ovarian cancer:
- It is unknown whether a BRCA VUS mutation:
- Is associated with an increased risk due to limited available data
- As the use of genetic testing increases and as more of the population is tested:
- The knowledge base regarding variant pathogenicity constantly grows
- Given the amount of data available from many years of BRCA 1 / 2 testing:
- The prevalence of VUS among this population has declined to 2% to 5%:
- However, among moderate and low penetrance genes:
- The number of VUS continues to rise
- However, among moderate and low penetrance genes:
- The prevalence of VUS among this population has declined to 2% to 5%:
- As the data expand and knowledge regarding a variant evolves:
- A variant may be reclassified:
- In a recent study reported in the Journal of the American Medical Association:
- 25.4% of patients initially diagnosed with a VUS were reclassified over a 12-year period:
- Of these patients, 97% were downgraded to benign or likely benign
- Three percent of patients were upgraded to pathogenic or likely pathogenic variants
- Given this low risk of reclassification to pathogenic mutation:
- Risk-reducing mastectomy, salpingo-oophorectomy, or genetic testing of family members are not indicated for this patient
- 25.4% of patients initially diagnosed with a VUS were reclassified over a 12-year period:
- In a recent study reported in the Journal of the American Medical Association:
- There is currently no established effective screening protocol for pancreatic cancer, even among patients with a deleterious BRCA 2 mutation
- A variant may be reclassified:
- References
- Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405-424.
- Hall MJ, Reid JE, Burbidge LA, Pruss D, Deffenbaugh AM, Frye C, et al. BRCA1 and BRCA2 mutations in women of different ethnicities undergoing testing for hereditary breast-ovarian cancer. Cancer. 2009;115(10):2222-2233.
- Mersch J, Brown N, Pirzadeh-Miller S, Mundt E, Cox HC, Brown K, et al. Prevalence of variant reclassification following hereditary cancer genetic testing. JAMA. 2018;320(12):1266-1274.
#Arrangoiz #CancerSurgeon #BreastSurgeon #SurgicalOncologist #BreastCancer #BRCAMutation #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital
