- Breast cancer is the most frequent malignancy in women:
- Is a heterogeneous disease on the molecular level
- Over the past 10 to 15 years:
- Treatment concepts have evolved to take this heterogeneity into account:
- With emphasis being placed on:
- More biologically-directed therapies and treatment de-escalation to reduce the adverse effects of treatment
- Despite the inherent molecular heterogeneity, which is a driving principle of modern-day treatments:
- Some features such as the impact of locoregional tumor burden or metastatic patterns are shared and influence therapy
- With emphasis being placed on:
- Treatment concepts have evolved to take this heterogeneity into account:
- Early breast cancer:
- That is, cancer that is contained in the breast or that has only spread to the axillary lymph nodes:
- Is considered curable
- Improvements in multimodal therapy have led to:
- Increasing chances for cure in approximately 70% to 80% of patients
- By contrast, advanced (metastatic) disease is not considered curable using currently available therapeutic options:
- However, advanced breast cancer is a treatable disease:
- For which the main goals of therapy are to prolong survival and control symptoms with low treatment-associated toxicity:
- To maintain or improve quality of life (that is, improved quality-adjusted life expectancy).
- For which the main goals of therapy are to prolong survival and control symptoms with low treatment-associated toxicity:
- However, advanced breast cancer is a treatable disease:
- That is, cancer that is contained in the breast or that has only spread to the axillary lymph nodes:
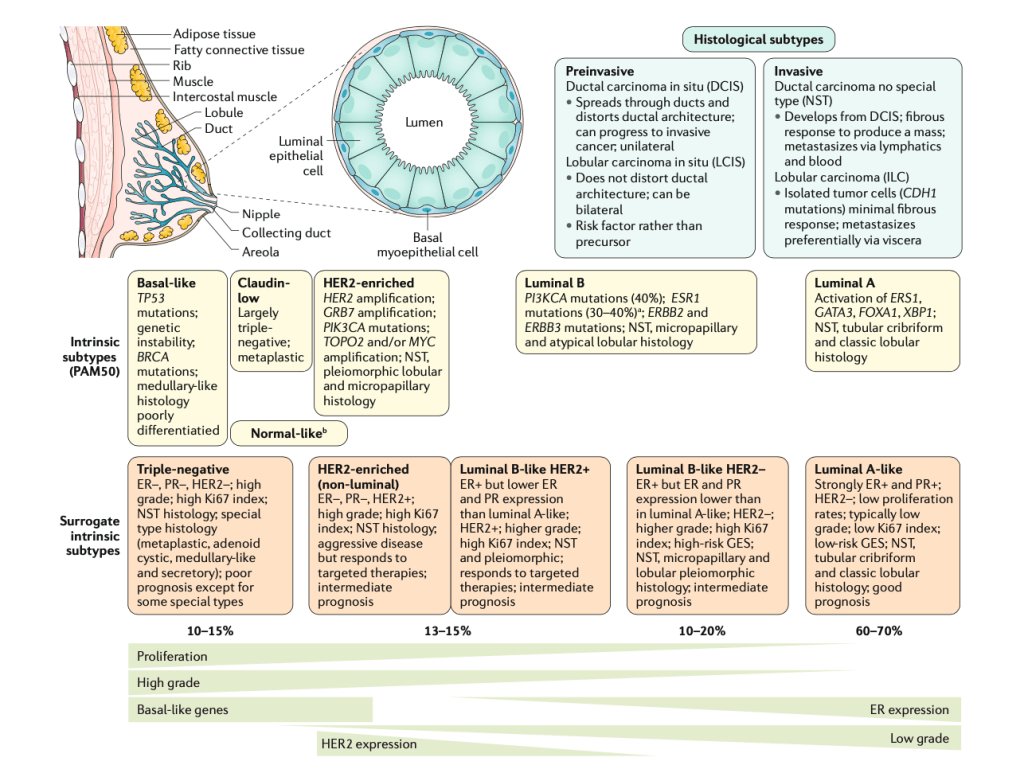
- All breast cancers arise in:
- The terminal duct lobular units (the functional unit of the breast) of the collecting duct
- The histological and molecular characteristics:
- Have important implications for therapy, and several classifications on the basis of molecular and histological characteristics have been developed
- The histological subtypes described here (top right) are the most frequent subtypes of breast cancer:
- Invasive:
- Ductal carcinoma (now referred to as ‘no special type’ (NST)):
- Develops from:
- DCIS
- Fibrous response:
- To produce a mass
- Metastasizes via:
- Lymphatics and blood
- Develops from:
- Lobular carcinoma:
- Isolated tumor cells:
- CDH1 mutations
- Minimal fibrous response
- Metastasizes preferentially:
- Via viscera
- Isolated tumor cells:
- Ductal carcinoma (now referred to as ‘no special type’ (NST)):
- Pre-invasive:
- Ductal carcinoma in situ:
- Spreads through ducts and distorts ductal architecture:
- Can progress to invasive cancer:
- Unilateral
- Can progress to invasive cancer:
- Spreads through ducts and distorts ductal architecture:
- Lobular carcinoma in situ (or lobular neoplasia):
- Does not distort ductal architecture:
- Can be bilateral
- Risk factor rather than precursor
- Does not distort ductal architecture:
- Ductal carcinoma in situ:
- Invasive:
- The intrinsic subtypes of:
- Perou and Sorlie are based on:
- A 50-gene expression signature (PAM50)
- Basal-like:
- TP53 mutations
- Genetic instability
- BRCA mutations
- Medullary-like histology
- Poorly differentiatied
- Claudin- low:
- Largely triple-negative
- Metaplastic histology
- HER2-enriched:
- HER2 amplification
- GRB7 amplification
- PIK3CA mutations
- TOPO2 and / or MYC amplification
- NST, pleiomorphic lobular and micropapillary histology
- Normal-like:
- Artefact:
- Expression of normal breast components:
- Due to low tumor cellularity
- Expression of normal breast components:
- Artefact:
- Perou and Sorlie are based on:
- The surrogate intrinsic subtypes:
- Are typically used clinically:
- Are based on histology and immunohistochemistry expression of key proteins:
- Estrogen receptor (ER)
- Progesterone receptor (PR)
- Human epidermal growth factor receptor 2 (HER2)
- The proliferation marker Ki67
- Are based on histology and immunohistochemistry expression of key proteins:
- Tumors expressing ER and / or PR are termed:
- Hormone receptor-positive
- Tumors not expressing ER, PR and HER2 are called:
- Triple-negative
- Triple-negative:
- 10% to 15% of the cases
- ER negative, PR negative, HER2 negative
- High grade
- High Ki-67 index
- NST histology
- Special type histology:
- Metaplastic
- Adenoid cystic
- Medullary-like
- Secretory
- Poor prognosis:
- Except for some special types
- HER2-enriched (non-luminal):
- 13% to 15% of the cases
- ER negative, PR negative, HER2 positive
- High grade
- High Ki-67 index
- NST histology
- Aggressive disease:
- But responds to targeted therapies
- Intermediate prognosis
- Luminal B-like HER2 Positive:
- 13% to 15% of the cases
- ER positive:
- But lower ER and PR expression than luminal A-like
- HER2 positive
- Higher grade
- High Ki-67 index
- NST and pleomorphic
- Responds to targeted therapies
- Intermediate prognosis
- Luminal B-like HER2 Negative:
- 10% to 20% of the cases
- ER positive:
- But ER and PR expression lower than in luminal A-like
- HER2 negative
- Higher grade
- High Ki-67 index
- High-risk gene expression signature (GES)
- NST, micro papillary and lobular pleomorphic histology
- Intermediate prognosis
- Luminal A-like:
- 60% to 70% of the cases
- Strongly ER positive and PR positive
- HER2 negative
- Low proliferation rates
- Typically low grade
- Low Ki-67 index
- Low-risk gene expression signature (GES)
- NST, tubular cribriform histology and classic lobular histology
- Good prognosis
- Are typically used clinically:
#Arrangoiz #CancerSurgeon #BreastSurgeon #CASO #CenterforAdvancedSurgicalOncology
