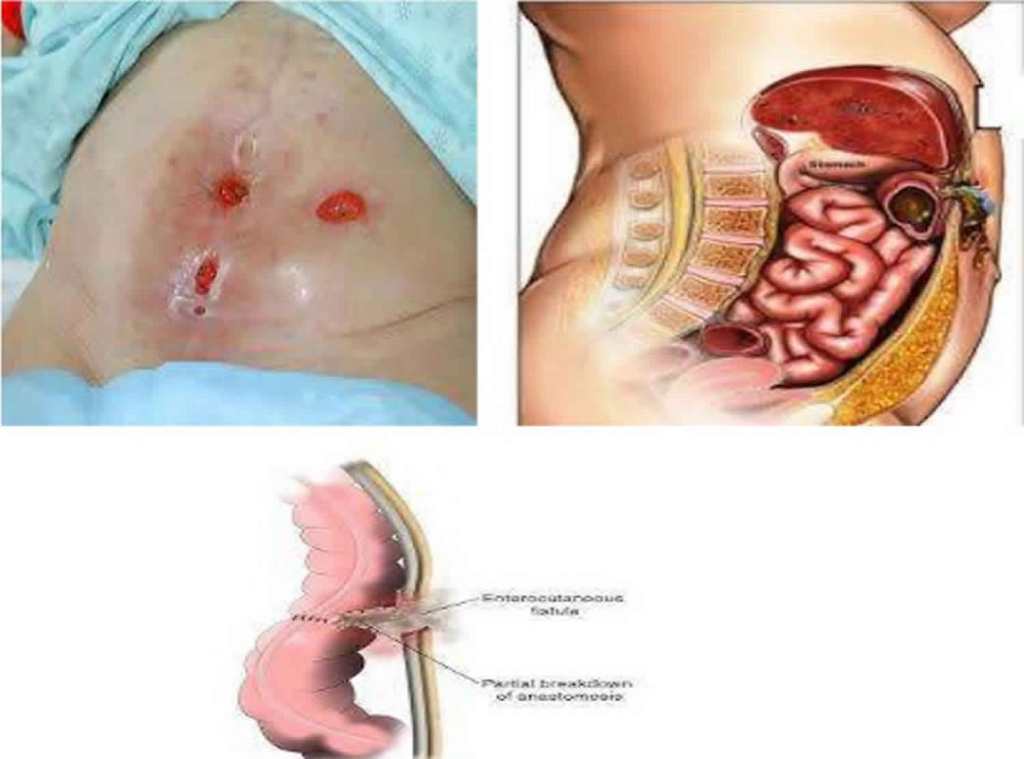
- An enterocutaneous fistula (ECF):
- Is an abnormal communication between the small or large bowel and the skin that allows the contents of the stomach or intestines to leak through an opening in the skin
Classification:
- Congenital types:
- Tracheoesophageal
- Vitellointestinal duct
- Patent urachus
- Rectovaginal
- Acquired:
- Trauma (postoperative)
- Radiation
- Malignancy,
- Infection
Two categories:
- Low-output fistula:
- Less than 500 mL/day
- High-output fistula:
- Equal or greater than 500 mL/day
Three categories:
- Low-output fistula:
- Less than 200 mL/day
- Moderate-output fistula:
- 200ml to 500 mL/day
- High-output fistula:
- Greater than 500 mL/day
- Etiology:
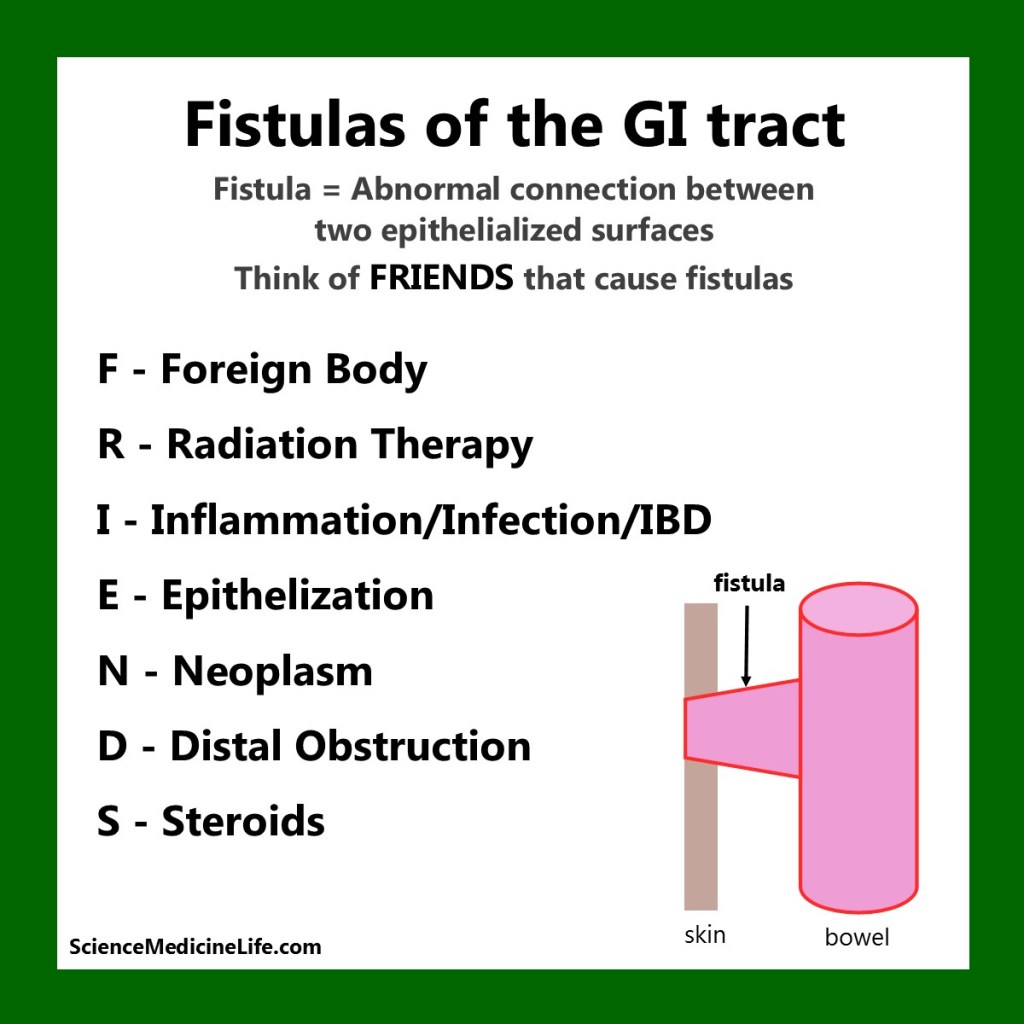
The mnemonic FRIENDS can be used to memorize characteristics which impede the closure of ECF:
- F Foreign body
- R Radiation
- I Infection or Inflammatory bowel disease
- E Epithelialization
- N Neoplasm
- D Distal obstruction
- S Short tract (less than 2 cm)
- Patients with enteric content exiting a wound on their abdomen are motivated to undergo operation:
- The majority will close spontaneously within approximately 6 weeks
- If it has not closed by 12 weeks:
- It is unlikely to do so and definitive surgery should be planned:
- The median time to definitive repair from fistula onset was 6 months (range 1 day to 28 months):
- The 6-month time course is commonly utilized by groups with significant experience treating fistulas, owing to the trend in encountering a less hostile abdomen than in the early phases
- Some evidence also suggests that somatostatin can be an effective treatment with respect to reducing closure time and improving the spontaneous closure rate of enterocutaneous fistulas
- The median time to definitive repair from fistula onset was 6 months (range 1 day to 28 months):
- It is unlikely to do so and definitive surgery should be planned:
- References:
- Lee SH (2012). “Surgical management of enterocutaneous fistula”. Korean Journal of Radiology. 13 Suppl 1: S17–S20. doi:10.3348/kjr.2012.13.S1.S17. PMC 3341456. PMID 22563283.
- Galie KL, Whitlow CB (2006). “Postoperative enterocutaneous fistula: when to reoperate and how to succeed”. Clinics in Colon and Rectal Surgery. 19: 237–246. doi:10.1055/s-2006-956446. PMC 2780112. PMID 20011327.
- Ross H (2010). “Operative surgery for enterocutaneous fistula”. Clinics in Colon and Rectal Surgery. 23: 190–194. doi:10.1055/s-0030-1262987. PMC 2967319. PMID 21886469.
- Stevens, P; Foulkes, RE; Hartford-Beynon, JS; Delicata, RJ (October 2011). “Systematic review and meta-analysis of the role of somatostatin and its analogues in the treatment of enterocutaneous fistula”. European Journal of Gastroenterology & Hepatology. 23 (10): 912–922. doi:10.1097/MEG.0b013e32834a345d. PMID 21814141.
- Metcalf C (1999). “Enterocutaneous fistulae”. Journal of Wound Care. 8 (3): 141–142. doi:10.12968/jowc.1999.8.3.25854.
#Arrangoiz #Surgeon #CancerSurgeon #CASO #CenterforAdvancedSurgicalOncology #PalmettoGeneralHospital
