- Mechanisms / Pathophysiology of Breast Cancer:
- The exact mechanism by which breast cancer is initiated:
- Is unknown:
- However, much effort has been made to molecularly characterize breast cancer and delineate its formation and progression
- Is unknown:
- At the cell of origin level:
- The clonal evolution model:
- In which mutations accumulate
- Epigenetic changes in tumor cells occur
- The ‘fittest’ cells survive
- The cancer stem cell model:
- In which only the precursor cancer cells:
- Initiate and sustain progression
- Cancer stem cells may also evolve in a clonal fashion
- Initiate and sustain progression
- In which only the precursor cancer cells:
- The clonal evolution model:
- At the morphological level:
- There is a continuum of lesions and genetic modifications from normal glands to cancer
- The exact mechanism by which breast cancer is initiated:
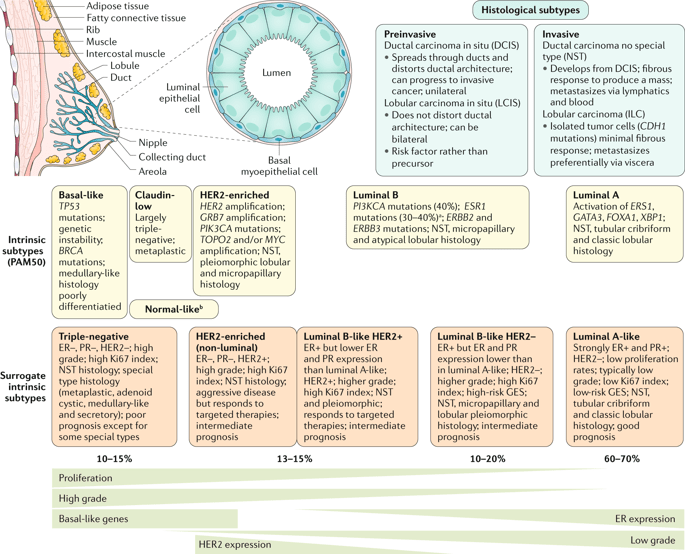
- All breast cancers arise in the:
- Terminal duct lobular units (the functional unit of the breast) of the collecting duct
- The histological and molecular characteristics have:
- Important implications for:
- Therapy:
- Several classifications on the basis of molecular and histological characteristics have been developed:
- The most frequent histological subtypes of breast cancer include:
- Invasive lesions:
- Ductal carcinoma (now referred to as ‘no special type’ (NST))
- Lobular carcinoma
- Preinvasive counterparts are:
- Ductal carcinoma in situ
- Lobular carcinoma in situ (or lobular neoplasia)
- Invasive lesions:
- The most frequent histological subtypes of breast cancer include:
- Several classifications on the basis of molecular and histological characteristics have been developed:
- Therapy:
- Important implications for:
- The intrinsic subtypes of Perou and Sorlie:
- Are based on:
- A 50-gene expression signature:
- PAM50
- A 50-gene expression signature:
- Are based on:
- The surrogate intrinsic subtypes:
- Are typically used clinically:
- Are based on:
- Histology
- Immunohistochemistry:
- Looking for the expression of key proteins:
- Estrogen receptor (ER)
- Progesterone receptor (PR)
- Human epidermal growth factor receptor 2 (HER2)
- The proliferation marker Ki67
- Looking for the expression of key proteins:
- Tumors expressing ER and / or PR are termed:
- Hormone receptor-positive
- Tumors not expressing ER, PR and HER2 are called:
- Triple-negative
- Are based on:
- Are typically used clinically:
- At the molecular level:
- There is evidence showing that breast cancer evolves along two divergent molecular pathways of progression:
- Mainly related to:
- ER expression
- Tumor grade
- Proliferation:
- These are described in the intrinsic classification
- Mainly related to:
- There is evidence showing that breast cancer evolves along two divergent molecular pathways of progression:
- Intrinsic classification (Intrinsic Subtypes PAM50):
- Basal-like:
- TP-53 mutations
- Genetic instability
- BRCA mutations
- Medullary-like histology
- Poorly differentiatied tumors
- Claudin- low:
- Largely triple-negative
- Metaplastic
- Basal-like:
- HER2-enriched:
- HER2 amplification
- GRB7 amplification
- PIK3CA mutations
- TOPO2 and/or MYC amplification
- NST, pleiomorphic lobular, and micro-papillary histology
- Normal-like:
- Artefact:
- Expression of normal breast components due to low tumour cellularity
- Artefact:
- Luminal B:
- PI3KCA mutations (40%)
- ESR1 mutations (30% to 40%):
- Induced by aromatase inhibitor targeted therapy
- ERBB2 and ERBB3 mutations
- NST, micropapillary and atypical lobular histology
- Luminal A
- Activation of ERS1, GATA3, FOXA1, XBP1
- NST, tubular, cribriform, and classic lobular histology
- Surrogate intrinsic subtypes:
- Triple-negative:
- ER negative, PR negative, HER2 negative
- High grade
- High Ki67 index
- NST histology
- Special type histology:
- Metaplastic
- Adenoid cystic
- Medullary-like
- Secretory
- Poor prognosis:
- Except for some special types
- HER2-enriched (non-luminal):
- ER negative, PR negative, HER2 positive
- High grade
- High Ki67 index
- NST histology
- Aggressive disease:
- But responds to targeted therapies
- Intermediate prognosis
- Luminal B-like HER2 positive:
- ER positive:
- But lower ER and PR expression than luminal A-like
- HER2 positive
- Higher grade
- High Ki67 index
- NST and pleiomorphic
- Responds to targeted therapies
- Intermediate prognosis
- ER positive:
- Triple-negative:
- Luminal B-like HER2 Negative:
- ER positive:
- But ER and PR expression lower than in luminal A-like
- HER2 negative
- Higher grade
- High Ki67 index
- High-risk GES (gene expression signature)
- NST, micropapillary and lobular pleiomorphic histology
- Intermediate prognosis
- Luminal A-like:
- Strongly ER positive and PR positive
- HER2 negative
- Low proliferation rates
- Typically low grade
- Low Ki67 index
- Low-risk GES (gene expression signature)
- NST, tubular, cribriform, and classic lobular histology
- Good prognosis
- ER positive:
- Rodrigo Arrangoiz MS, MD, FACS cirujano oncology y cirujano de mamá de Sociedad Quirúrgica S.C en el America British Cowdray Medical Center en la ciudad de Mexico:
- Es experto en el manejo del cáncer de mama.

👉Es miembro de la American Society of Breast Surgeons:

Training:
• General surgery:
• Michigan State University:
• 2004 al 2010

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• Fox Chase Cancer Center (Filadelfia):
• 2010 al 2012

• Masters in Science (Clinical research for health professionals):
• Drexel University (Filadelfia):
• 2010 al 2012

• Surgical Oncology / Head and Neck Surgery / Endocrine Surgery:
• IFHNOS / Memorial Sloan Kettering Cancer Center:
• 2014 al 2016


