A meta-analysis demonstrated that a positive surgical margin (defined as the presence of invasive disease or ductal carcinoma in situ on ink):
Is associated with at least a twofold increase in the risk of ipsilateral breast tumor recurrence (odds ratio 1.96):
Which has been confirmed by other series
Although a boost may partially mitigate the effect of a positive surgical margin:
The risk of a local failure remains higher than in a patient with a cleared surgical margin treated with whole-breast irradiation
Furthermore, a randomized clinical trial showed that increasing the boost dose does not nullify the increased risk of local recurrence associated with a positive surgical margin (standard boost dose: 17.5% vs. increased boost dose: 10.8%, P>0.1):
This is true regardless of the type and fractionation pattern of the radiotherapy
Neither favorable tumor biology (including receptor status) nor the administration of systemic therapy:
Can completely offset the effect of a positive margin
The patient should be counseled on the higher rates of local recurrence:
With a known positive margin
American Society for Radiation Oncology (ASTRO) 2018 boost guidelines:
Recommend a boost for patients:
Less than 50 years
51 years to 70 years old with:
High-grade disease or positive margins
Patients with positive margins are considered “unsuitable” by the ASTRO recommendations for accelerated partial breast radiation therapy
References
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21(3):717-730.
DiBiase SJ, Komarnicky LT, Heron DE, Schwartz GF, Mansfield CM. Influence of radiation dose on positive surgical margins in women undergoing breast conservation therapy. Int J Radiat Oncol Biol Phys. 2002; 53(3):680-686.
Moran MS, Schnitt SJ, Giuliano AE, et al; Society of Surgical Oncology; American Society for Radiation Oncology. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stage I and II invasive breast cancer. J Clin Oncol. 2014;32(14):1507-1515.
Barelink H, Maingon P, Poortmans PM, et al. Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3. Lancet Oncol. 2015;16(1):47-56.
Smith BD, Bellon JR, Blitzblau R, et al. Radiation therapy for the whole breast: executive summary of an American Society for Radiation Oncology (ASTRO) evidence-based guideline. Pract Radiat Oncol. 2018;8(3):145-152.
Correa C, Harris EE, Leonardi MC, et al. Accelerated partial breast irradiation: executive summary for the update of an ASTRO evidence-based consensus statement. Pract Radiat Oncol. 2017;7(2):73-79.
What are the rates of axillary pathologic complete response (pCR) for different breast cancer subtypes in patients with initially clinically node-positive breast cancer
Findings:
This systematic review and meta-analysis, including 33 unique studies with 57 531 unique patients:
Showed that the hormone receptor (HR)–negative / ERBB2-positive subtype:
Was associated with the highest axillary pCR rate (60%)
The remaining subtypes were associated with the following axillary pCR rates in decreasing order:
59% for ERBB2-positive
48% for triple-negative
45% for HR-positive / ERBB2-positive
35% for luminal B
18% for HR-positive / ERBB2-negative
13% for luminal A
Meaning:
These data can help estimate axillary treatment response in the neoadjuvant setting and thus select patients for more or less invasive axillary procedures
Importance:
An overview of rates of axillary pathologic complete response (pCR) for all breast cancer subtypes, both for patients with and without pathologically proven clinically node-positive disease, is lacking
Objective:
To provide pooled data of all studies in the neoadjuvant setting on axillary pCR rates for different breast cancer subtypes in patients with initially clinically node-positive disease
Data Sources:
The electronic databases Embase and PubMed were used to conduct a systematic literature search on July 16, 2020
The references of the included studies were manually checked to identify other eligible studies
Study Selection:
Studies in the neoadjuvant therapy setting were identified regarding axillary pCR for different breast cancer subtypes in patients with initially clinically node-positive disease (ie, defined as node-positive before the initiation of neoadjuvant systemic therapy)
Data Extraction and Synthesis:
Two reviewers independently selected eligible studies according to the inclusion criteria and extracted all data
All discrepant results were resolved during a consensus meeting
To identify the different subtypes, the subtype definitions as reported by the included articles were used
The random-effects model was used to calculate the overall pooled estimate of axillary pCR for each breast cancer subtype
Main Outcomes and Measures:
The main outcome of this study was the rate of axillary pCR and residual axillary lymph node disease after neoadjuvant systemic therapy for different breast cancer subtypes, differentiating studies with and without patients with pathologically proven clinically node-positive disease
Results:
This pooled analysis included 33 unique studies with 57 531 unique patients and showed the following axillary pCR rates for each of the 7 reported subtypes in decreasing order:
60% for hormone receptor (HR)–negative /ERBB2 (formerly HER2)–positive
59% for ERBB2-positive (HR-negative or HR-positive)
48% for triple-negative
45% for HR-positive / ERBB2-positive
35% for luminal B
18% for HR-positive / ERBB2-negative
13% for luminal A
No major differences were found in the axillary pCR rates per subtype by analyzing separately the studies of patients with and without pathologically proven clinically node-positive disease before neoadjuvant systemic therapy
Conclusions and Relevance:
The HR-negative / ERBB2-positive subtype was associated with the highest axillary pCR rate
These data may help estimate axillary treatment response in the neoadjuvant setting and thus select patients for more or less invasive axillary procedures
Can decrease the size of a primary tumor to allow for breast conservation, eliminate nodal metastasis in some patients, and provide prognostic information:
The optimal timing of sentinel lymph node biopsy (SLNB) for patients treated with NAC has been controversial
Clinical staging of the axilla with SLNM / SLNB:
Is feasible both before and after chemotherapy
SLNB prior to NAC:
May be a more accurate approach than after NAC
Chemotherapy:
May alter lymphatic drainage through fibrosis of lymphatic channels:
Decreasing the accuracy of SLNB
SLNB before NAC has a lower false negative rate and provides more accurate staging:
Which could determine radiation fields
Unfortunately, SLNB prior to NAC:
Requires an additional operation
Could delay the initiation of chemotherapy
Fails to decrease the rate of ALND
It also given by the effect of chemotherapy on axillary metastasis
These concerns have led to interest in performing SLNB after NAC
Several recent prospective trials have examined the accuracy of SLNB after NAC:
The American College of Surgeons Oncology Group (ACOSOG) / Alliance Z1071:
Enrolled women with T0 to T4, N1 to N2 clinical disease:
Who underwent neoadjuvant chemotherapy
All patients underwent pre-NAC axillary needle biopsy
Forty-one percent of patients had a:
Pathologic complete response in the axilla
After chemotherapy:
Patients underwent both SLNB and ALND
A sentinel lymph node could not be identified:
In 7% of patients
The overall false negative rate was 13% (12.6%):
Which did not meet the preset target of 10%
The false negative rate was 21% in patients with two or fewer sentinel lymph nodes identified:
But dropped to 9.1%:
When greater than three sentinel lymph nodes were sampled
In the Sentinel Lymph Node Biopsy in Patients with Breast Cancer Before and After Neoadjuvant Chemotherapy (SENTINA) trial:
1,022 patients underwent SLNB before NAC:
With a detection rate of 99%
For patients who were evaluated after NAC and converted from cN+ to ycN0:
The sentinel lymph node detection rate was only 80%:
With a false negative rate of 14.2%
As seen in ACOSOG Z1071:
The false negative rate:
Was much higher in patients with only one node removed (24%):
Than in those with three or more sentinel nodes removed (7%)
The false negative rate was also improved:
By the use of radiocolloid and blue dye together:
Compared with blue dye alone:
False negative rate of 9% versus 16%
The Sentinel Node Biopsy following NeoAdjuvant Chemotherapy (SN FNAC) study:
Enrolled patients with cT0 to cT3 with cN1 to cN2 biopsy-proven breast cancer treated with NAC
Following chemotherapy, patients underwent clinical and ultrasound examination followed by SLNB and completion ALND
The overall post-NAC SLNB false negative rate was:
8% in 153 patients
When only one sentinel lymph node was evaluated:
The false negative rate was again unacceptably high:
At 20%
On the basis of these three trials:
Resecting only one sentinel node:
Is associated with an unacceptably high false negative rate
The false negative rate after NAC may be lowered with the use of:
Dual tracers and resecting three or more sentinel nodes
Placing clips in positive lymph nodes before chemotherapy:
Decreases the false negative rate:
If the clipped node is then resected during SLNB
The sentinel lymph node identification rate after NAC:
Is significantly improved with increased surgeon experience:
Suggesting that a learning curve is needed to obtain accurate SLNB after NAC
SLNB after NAC:
Has the potential to decrease the number of women who receive ALND
A study of 288 prospectively identified clinically node-positive patients:
Reported that 132 became clinically node negative after NAC
The clinically node-negative patients were then eligible for SLNB:
48% had negative sentinel lymph nodes and were able to avoid an ALND
Current ASCO recommendations state that:
SLNB should be offered to patients who have received preoperative neoadjuvant systemic therapy and have clinically negative lymph nodes:
However, no large studies have examined local recurrence rates or survival:
When ALND is omitted in patients who convert from node positive to node negative after NAC
The safety of avoiding ALND in these patients:
Has not been demonstrated
The National Surgical Adjuvant Breast and Bowel Project (NSABP) B51 and Alliance A011202 are two sister studies:
Examining the role of SLNB, ALND, and nodal radiation in patients who receive NAC
The results of these trials will help identify patients who can safely avoid ALND after NAC
Has been the most extensively studied causative factor in the development of thyroid cancer
Factors that increase the risk for developing PTC after radiation exposure include:
Female gender
Radiation for childhood cancer (rather than benign conditions)
A family history of thyroid cancer
In one study, younger age at exposure and dose of radiation administered:
Significantly influenced the risk of development of cancer
Polybrominated Diphenyl Ethers
Some have proposed a potential role of polybrominated diphenyl ethers (PBDEs) in the development of thyroid cancer
These ubiquitous flame retardants may be found in plastics, electrical appliances, televisions, computers, building supplies, foams, carpets, and upholstery
PBDEs and their metabolites may accumulate in human tissues and bear a striking structural similarity to thyroxine
These compounds have been shown to be potent endocrine disrupters, with thyroid and estrogen effects being the most common
Although there has been no direct link between an increased risk of thyroid cancer and PBDEs, their increased oncogenic potential in other tissues, has made them an attractive candidate for further study in thyroid cancer
Obesity
Obesity and overweight were linked to nearly 18% of all cancer cases and 16% of cancer deaths in 2014
Several studies have identified a significantly higher risk of thyroid cancer in overweight and obese patients
The inflection point in the incidence of thyroid cancer occurred in the mid-1970s; there was a similar change in the trend for obesity rates in the United States just a few years prior:
Over time the slopes of these two conditions have remained nearly parallel:
Consequently, some have postulated a potential causal relationship, although the mechanism is elusive
Obesity affects the secretion of:
Adipokines by adipose tissue, including increased leptin and decreased adiponectin
Through complex molecular signaling, these adipokines interact with key factors in carcinogenesis, including:
Cell proliferation, angiogenesis, and antiinflammatory cytokines
Further studies are necessary to delineate the role of obesity in the development of thyroid cancer, particularly as the incidence of obesity continues to climb throughout Europe, North America, and Asia
Hereditary Syndromes
The majority of thyroid cancers are sporadic:
However, approximately 5% of non-medullary thyroid cancers are hereditary
These hereditary cases have been divided into two groups:
Those tumors associated with a familial cancer syndrome, such as familial adenomatous polyposis, Gardner syndrome, Cowden disease, Carney complex type 1, or Werner syndrome
Those with thyroid tumors as the primary feature, such as familial non-medullary thyroid cancer
Nipple discharge is the third most common breast-related complaint:
After breast pain and breast nodule
During their reproductive years:
Up to 80% of women will have an episode of nipple discharge
Most nipple discharge:
Is of benign origin
The primary goals of evaluation and management are to:
Differentiate patients with benign nipple discharge from those who have an underlying:
Papilloma, high-risk lesion, or cancer and to manage patients with underlying pathologic nipple discharge
Types and causes of nipple discharge:
Based on the characteristics of presentation nipple discharge is categorized as:
Normal milk production (lactation)
Physiologic nipple discharge (galactorrhea)
Pathologic (suspicious) nipple discharge
Lactation:
The normal secretory products of the breast are:
Milk and colostrum
During pregnancy and the postpartum period:
The mammary glands develop and produce milk:
In response to a number of physical and biochemical forces
Milk secretion can continue for at least six months after delivery or after cessation of breastfeeding
Physiologic nipple discharge (galactorrhea):
Is defined as nonpathologic nipple dischargeunrelated to pregnancy or breastfeeding
Galactorrhea:
Is usually manifested as bilateral milky nipple discharge involving multiple ducts
The nipple discharge, although usually bilateral and white or clear:
May also be unilateral and a variety of other colors, including yellow (straw colored), green, brown, or gray, but not bloody
Galactorrhea is often caused by hyperprolactinemia, which may be secondary to medications, pituitary tumors, endocrine abnormalities, or other medical conditions
Pathologic (suspicious) nipple discharge:
Secretory production of fluids other than milk may be due to a pathological process in the breast
The discharge is usually:
Unilateral and localized to a single duct, persistent, and spontaneous
It can be serous (clear or yellow), sanguineous (bloody), or serosanguineous (blood tinged)
Common etiologies of pathologic nipple discharge include:
Benign Papilloma:
Is the most common cause of pathologic nipple discharge:
52% to 57% of the cases
A papilloma is a papillary tumor growing from the lining of the breast duct
The discharge associated with a papilloma can range from clear to grossly bloody
Solitary papillomas:
Can occasionally harbor areas of atypia or ductal carcinoma in situ (DCIS)
Duct ectasia:
Is another common benign cause of pathologic nipple discharge
Seen in approximately 14% to 33% of pathologic nipple discharge cases
Cancer:
Cancer is found in 5% to 15% of cases of pathologic nipple discharge
The most common malignancy associated with nipple discharge in the absence of other findings is DCIS
Infection:
Purulent nipple discharge can be seen in association with periductal mastitis
Clinical evaluation:
A thorough history and physical examination should be performed in all women with nonlactational nipple discharge to determine if it is physiologic or pathologic
History:
The clinical history is most helpful in distinguishing physiologic from pathologic nipple discharge
While a complete medical history should be obtained, specific areas to address are:
The appearance of the discharge:
Bloody versus nonbloody
Frequency of the discharge
Whether the discharge is spontaneous or provoked by manipulation of the breast and / or nipple-areolar complex
Whether the discharge is:
Unilateral or bilateral
Uniductal or multiductal
Physiologic nipple discharge:
Is usually bilateral and multiductal and occurs with breast manipulation
The risk of cancer is higher when the discharge is:
Spontaneous
Bloody
Unilateral
Uniductal
Associated with a breast mass
Occurs in a woman over 40 years of age
A history of recent trauma should also be elicited:
Trauma can include mammographic imaging with compression as well as vigorous manipulation of the nipple
Recent onset of amenorrhea or other symptoms of hypogonadism (hot flashes, vaginal dryness):
Should prompt consideration of hyperprolactinemia
Several classes of medications can cause hyperprolactinemia:
First generation antipsychotics
Second generation antipsychotics
Cyclic antidepressants
SSRI antidepressants
Other antidepressants
Antiemetic or gastrointestinal
Anticoagulants can cause blood nipple discharge in patients who sustain trauma to the breasts, even that as mild as mammographic manipulation
Physical examination:
A complete breast examination should be performed
The specific goals of the examination are to:
Note the symmetry and contour of the breasts, position of the nipples, scars, and vascular pattern as well as any evidence of skin retraction, dimpling, edema or erythema, ulceration or crusting of the nipple, and changes in skin color
In particular, the skin covering the breast and nipple-areolar complex should be examined for lesions that may be staining the woman’s clothes and mimicking nipple discharge:
Some examples are Paget disease, insect bites, local infections, and eczema:
Suspicious skin lesions should be biopsied
Elicit discharge from a nipple and identify the involved duct or ducts:
Pressure in a clockwise fashion around the areola can help identify a specific site or duct that is producing the discharge
If fluid is elicited, the location of the duct(s) should be noted
If no discharge is elicited, a warm compress placed on the breasts will enhance the chances of detecting mammary secretion
Gentle, firm pressure should be applied to the base of the areola (not on the nipple), at the site where the newborn’s mouth is normally applied
Massage from the periphery towards the nipple-areolar complex may also help
It is important to observe whether the discharge comes from one or more ducts on the nipple:
A good light and magnifying lens can help with this identification
Detect enlarged axillary or supraclavicular lymph nodes
Delineate and document breast masses
Identify localized areas of tenderness and relate them to areas of pain noted by the woman and to other physical findings
For patients with bilateral discharge:
The physical examination should include:
Checking for a chiasmal syndrome (eg, bitemporal field loss) and signs of hypothyroidism or hypogonadism
Diagnostic evaluation:
Patients with suspected physiologic nipple discharge require laboratory evaluation, whereas those with suspected pathologic nipple discharge should undergo imaging studies
Physiologic discharge:
Nipple discharge that is bilateral and nonbloody is likely physiologic, which requires medical evaluation for possible hyperprolactinemia, but no specific breast imaging, provided that, for women, routine screening mammography is up to date
Some non-bloody-appearing discharge may still contain heme, and heme-occult testing may be considered
Laboratory evaluation (galactorrhea workup) should include a:
Pregnancy test, prolactin levels, renal and thyroid function tests, and appropriate follow-up with an endocrinologist if there are abnormal findings
Further endocrinological evaluation is also indicated for other systemic abnormalities, such as menstrual irregularity, infertility, headaches, visual disturbances, or symptoms of hypothyroidism
Pathologic discharge:
After clinical evaluation, all patients presenting with one of the following should undergo breast imaging to search for any underlying abnormality in the duct (or elsewhere in the breast) and direct surgical intervention:
Unilateral nipple discharge
Bloody nipple discharge
Nipple discharge associated with a mass or skin lesions
Laboratory tests for galactorrhea are not indicated for evaluation of suspected pathologic nipple discharge
Mammography and ultrasound:
For patients who present with pathologic nipple discharge, I usually start with diagnostic mammography and / or focused breast ultrasonography
Age is predictive of the risk of cancer in women with nipple discharge:
In one series of women with isolated nipple discharge malignancy was present in:
3% of those less than 40 years of age
10% of those 40 to 60 years of age
32% of those over 60 years of age
In men, nipple discharge is associated with an even higher incidence of breast cancer (23% to 57%), and nipple discharge may be their only clinical manifestation
Consequently, the choice and sequence of imaging modalities will depend on age and sex of the patient:
Women ≥ 40 years of age should undergo both diagnostic mammography and focused breast ultrasonography:
Patients who have had a recent mammogram (less than 6 months) or are pregnant may undergo breast ultrasonography alone
Women between 30 and 39 years of age should undergo diagnostic mammography first, followed by breast ultrasonography if necessary
Women less than 30 years of age should undergo breast ultrasonography first; mammography is only performed if the initial ultrasound shows a suspicious finding or if the patient is genetically predisposed to hereditary breast cancer
Given the rarity of cases and higher risk of breast cancer than women, men with pathologic nipple discharge should undergo both diagnostic mammography and breast ultrasonography to assist in diagnosis and guidance for biopsy if necessary
Mammography (digital with or without tomosynthesis):
Is the first-line imaging modality for evaluation of pathologic nipple discharge in most practices
Although it is the best modality for identifying suspicious lesions in the breast, mammography may fail to show cancers or high-risk lesions that are small, lack calcifications, or are entirely intraductal
The sensitivity and specificity of mammography for detection of cancer or high-risk lesions such as papilloma or atypia range from 7% to 10% and 94% to 100%, respectively
Focused ultrasonography:
Provides a useful tool for the diagnosis of ductal disease as it is directed to the periareolar area and provides visualization of dilated ducts and any nodules inside them
Ultrasound is especially useful for identifying lesions within the mammary ducts; it allows visualization of ductal pathology as small as 0.5 mm in diameter
When evaluating pathologic nipple discharge, ultrasound can identify 63% to 69% percent of lesions not visible on mammography
Ultrasound is also used to guide percutaneous biopsy of lesions and/or wire localization for surgery
Although ultrasound is more sensitive than mammography, it is less specific in differentiating benign from malignant lesions:
In a series of 52 patients with suspected ductal disease, ultrasonography had a sensitivity of 97% and a specificity of 60% with a positive predictive value of 95%
Magnetic resonance imaging:
Patients with pathologic nipple discharge but negative mammogram and ultrasound may undergo breast magnetic resonance imaging (MRI)
The use of breast MRI does have the risk of identifying additional findings that may lead to further imaging and biopsy, most of which are benign
Breast MRI is a relatively sensitive imaging modality with moderate specificity
Contrast-enhanced MRI has demonstrated sensitivities of 93% to 100% for invasive cancers as well as benign papillary lesions; however, specificity has been reported to be as low as 37%
The role of MRI in the evaluation of nipple discharge is evolving. Some studies support the use of MRI over ductoscopy due to its higher sensitivity and specificity; however, this remains an area of controversy
A meta-analysis comparing MRI versus galactography for pathologic nipple discharge found a higher diagnostic accuracy for MRI in cancer detection
MRI is also capable of identifying an etiology of discharge that is remote from the vicinity of the nipple
If MRI is going to be used in this setting, it should be done in a facility that has MRI-guided biopsy capabilities
Less commonly used studies:
At institutions where it is available, galactography (ductography) or ductoscopy may also be performed to evaluate pathologic nipple discharge in patients who have negative mammogram and ultrasound
However, these studies are less widely available, and any lesions identified are not accessible to needle biopsy and, therefore, require surgical excision with the duct
Galactography is a delicate, technically challenging study that can only be performed if the nipple discharge is reproducible on physical examination
During a galactography examination, the discharging nipple orifice is cannulated and injected with a small amount of contrast material, which allows a subsequent mammogram to visualize a filling defect
The intraductal lesion will appear as an intraductal filling defect, a complete ductal obstruction, or a wall irregularity
Although peripheral intraductal masses have been reported, the vast majority of intraductal masses are centrally located, near, or immediately deep to the nipple-areolar complex
In one study, galactography was associated with a sensitivity of 76% and specificity of 11%
The positive predictive value of galactography in this series was 19%
A successful galactography may help locate the lesion, which can aid the surgeon in more precisely localizing the proper area at the time of surgery, thereby limiting the amount of tissue excised
However, the absence of a lesion on galactogram does not exclude a cancer
Galactography should not be performed in patients with mastitis or a breast abscess, as it could worsen the inflammation
Galactography can cause mastitis if too much contrast material is injected or if too much pressure is used during injection, resulting in perforation of the duct and extravasation of contrast material
Magnetic resonance (MR) galactography is a different technique than standard breast MRI
It utilizes heavy T2 weighting, which accentuates the visibility of fluid-containing structures
No directly instilled or intravenous contrast material is necessary
MR galactography provides a three-dimensional image and can show the precise shape and location of the abnormal duct and lesion in the breast
However, this technique will not reveal ducts that are not dilated or those with low signal intensity on heavily T2-weighted images due to hemorrhage or the presence of proteinaceous contents within the duct
Mammary ductoscopy is another minimally invasive method for evaluation and treatment of nipple discharge
As with galactography, ductoscopy also requires a reproducible discharge and the ability to cannulate and dilate the discharging duct
Since first introduced in 1988, the size and resolution of endoscopes have improved significantly over time
With the aid of submillimeter endoscopes and air (Asia) or saline (North America) distention of the duct, it is possible to visualize the intraductal lesions that cause pathologic nipple discharge
When a solitary intraductal lesion is identified, it is either surgically excised or biopsied, both through a separate skin incision
Surgical excision is guided by transillumination from the ductoscope; when biopsy is planned, the tip of the ductoscope is identified with ultrasound so that percutaneous biopsy of lesions located near the scope tip can be carried out
Multiple intraluminal lesions are associated with a much higher rate of clinically occult cancer and, when encountered, should be widely excised
Cytology of the discharge or of a ductal lavage specimen is not recommended, because the result does not impact management:
Technically, it would be difficult to distinguish crenated or apoptotic cells from atypical cells, and abnormal cytologic findings cannot be easily localized to a specific lesion
Breast biopsy:
Imaging does not reliably differentiate cancers or high-risk lesions (eg, papilloma or atypia) from benign lesions that cause nipple discharge
Thus, abnormalities detected on mammography, ultrasonography, or MRI:
Require image-guided core needle biopsy with clip placement to mark the biopsied lesion:
The biopsy result will dictate further treatment
Skin punch biopsy:
Women sometimes may report finding a stain or spot of blood on their brassiere or underclothing. Although they may complain of nipple discharge, skin lesions on the nipple may be found instead:
Such lesions can have the appearance of dermatitis or eczema with erythematous lesions that weep or bleed
This presentation merits careful examination of the skin around the nipple and nipple-areolar complex, and a skin punch biopsy should be performed as these can be the first signs of Paget disease of the breast:
Paget disease is an uncommon form of breast cancer, characterized clinically by an eczematoid appearance with nipple crusting, scaling, or erosion.
Pathologic nipple discharge during pregnancy and lactation:
Bloody nipple discharge can be seen in up to 20% of women during the second or third trimester of pregnancy and lactation
The cause is usually hypervascularity of developing breast tissue, which is benign and requires no treatment
However, the evaluation of breast complaints in pregnancy and lactation can be complicated by the changing breast examination
Surgical evaluation is warranted for those with persistent bloody nipple discharge
Women who develop persistent pathologic nipple discharge during pregnancy should undergo breast ultrasonography:
If the result is negative, they can be followed, and further workup performed after delivery if their symptoms persist
If a suspicious lesion is identified on ultrasound, then an ultrasound-guided core needle biopsy can be performed, and they should be treated according to the result of the biopsy
Some women have bloody nipple discharge during the first days of lactation:
This is more common with the first pregnancy, and it is thought to be caused by the increased vascularization of the lobules and ducts with the onset of milk production
There is no contraindication to infants consuming milk that contains a little blood
If bloody nipple discharge persists for more than one week, other causes of bloody milk should also be considered and the patient should be formally evaluated for pathologic nipple discharge
Treatment:
Physiologic nipple discharge, or galactorrhea, is often caused by hyperprolactinemia, which may be secondary to medications, pituitary tumors, endocrine abnormalities, or other medical conditions:
If the patient is taking a medication that has been associated with galactorrhea (eg, metoclopramide, phenothiazines, selective serotonin reuptake inhibitors [SSRIs]) and the breast evaluation is otherwise negative, the patient should be educated that this is a side effect of the medication
If the symptom of ongoing nipple discharge is bothersome to the patient, the medication can be tapered or changed in consultation with the prescribing clinician. In other cases, continuing the medication is appropriate (eg, antipsychotic drugs)
Transient idiopathic galactorrhea (with normal prolactin level) can also occur, usually in premenopausal women:
If the workup is otherwise negative, the woman can be reassured that it is benign and be reassessed in two to three months
Pathologic nipple discharge:
For nonlactating individuals with pathologic nipple discharge, I recommend surgical management after a full evaluation has been completed
The extent of the surgery will depend on the result of the imaging studies and biopsy
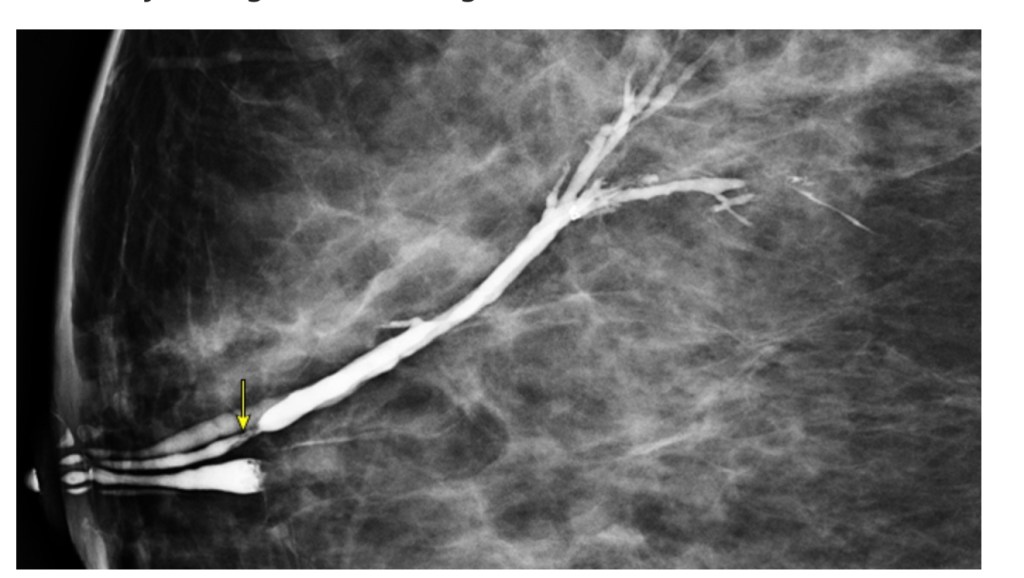
The ultrasound of the left breast shows a solitary dilated duct (A, arrow) with a filling defect consisting of soft tissue echoes within the duct (B, overlaid in green). These findings are consistent with a benign papilloma.Mammary ductogram with filling defect (arrow) indicating an intraductal mass.
The ABC trials established the use of non-anthracycline containing regimen:
Docetaxel and cyclophosphamide (TC) as adjuvant therapy in early breast cancer
In clinical practice, TC is commonly used in:
Stage I Triple Negative (TN)
Stage I,II hormone positive breast cancer
However, no specific recommendations exist in literature, regarding the number of cycles that can be used:
For example TC 4 vs TC 6
The aim of this study, was to determine if TC 4 is non-inferior to TC6 when used as adjuvant therapy in early breast cancer
Methods:
They retrospectively reviewed 143 patients who were diagnosed with early breast cancer, between 2007 to 2017, at there institution who had received either TC 4 or TC 6 as adjuvant therapy
The number of cycles the patients received were based on provider preference
The two groups (TC 4, TC 6) were compared in regard to stage of cancer at diagnosis based on AJCC 7th edition-stratified by TNM staging for hormone positive and T staging only for TN, grade of adverse events, recurrence and death from breast cancer
Median follow up was 5 years
Results:
Out of the 143, 102 (71.3%) received TC 4 and 41 (28.7%) received TC 6
Among the hormone positive, 42 were stage I and out of which 32 (76.2%) received TC 4 and 10 (23.8%) received TC 6 and there were 24 stage II patients, out of which 17 (70.8%) received TC 4 and 7 (29.2%) received TC 6
Among the TN group, there were 64 who were T1, out of which 45 (70.3%) received TC 4 and 19 (29.7%) received TC 6, while there were 12 T2 patients, out of which 7 (58.3%) received TC 4 and 5(41.7%) received TC 6
Recurrence of breast cancer was seen in 5 (4.9%) in TC 4 and 3 (7.3%) in TC 6, p=0.569
Death due to breast cancer was seen in 2 (1.9%) in TC 4 and 1 (2.4%) in TC 6, p=0.856
Adverse events were seen in 86 (84.3%) in TC 4 and 39 (95.1%) in TC 6,p=0.078
Adverse events of Grade 3 or higher were seen in 10 (9.8%) in TC 4 and 11 (26.8%) in TC6, p=0.09
Conclusions: In this limited series, TC 4 appears to be equally effective to TC 6, with fewer adverse events of any grade and lower incidence of Grade 3 or higher side effects which was statistically significant
Although the proportion of patients who received TC 4 were higher in these series, the percentage of patients who received TC 6 was higher in stage II for hormone positive and T2 for TN when compared to Stage 1 and T1 respectively
They also found a higher percentage of recurrence and death due to breast cancer in TC 6 which was not statistically significant and this likely a reflection of the fact that as mentioned above patient with a higher stage at diagnosis tended to receive 6 cycles as compared to 4 cycles and therefore had a higher chance of recurrence in the future
Giuliano AE, Ballman K, McCall L, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: long-term follow-up from the American College of Surgeons Oncology Group (Alliance) ACOSOG Z0011 randomized trial. Ann Surg. 2016;264:(3):413-420.
Neuman HB, Schumacher JR, Francescatti AB, et al. Risk of synchronous distant recurrence at time of locoregional recurrence in patients with stage II and III breast cancer (AFT-01). J Clin Oncol. 2018;36(10):975-980.
Wapnir IR, Price KN, Anderson SJ, et al. Efficacy of chemotherapy for ER-negative and ER-positive isolated locoregional recurrence of breast cancer. Final analysis of the CALOR Trial. N Engl J Med. 2018;36(11):1073-1079.
Qiang JK, Sutradhar R, Everett K, et al. Association between serum thyrotropin and cancer recurrence in differentiated thyroid cancer: a population-based retrospective cohort study. Thyroid. Epub 2024 Dec 26; doi: 10.1089/thy.2024.0330. PMID: 39723994.
Background:
In addition to surgery (thyroidectomy with or without lymphadenectomy) and radioactive iodine treatment (RAIT), patients with differentiated thyroid cancer (DTC) may benefit from thyroid hormone therapy that suppresses TSH to reduce the risk of recurrence
The 2015 American Thyroid Association (ATA) guidelines recommend:
Maintaining TSH levels below 0.1 mU/L in patients with high-risk DTC:
As this has been shown to improve survival in these patients
The level of TSH suppression should be adjusted based on:
Comorbidities and response to treatment
However, TSH suppression is not without risks, and has been associated with an increased risk of:
Osteoporosis
Atrial fibrillation
A reduced quality of life
In patients with low-risk DTC:
The ATA guidelines recommend maintaining TSH levels between 0.5 and 2.0 mU/L:
As further TSH suppression in these cases increases the risks associated with subclinical hyperthyroidism without affecting cancer recurrence rates
The present study aimed to evaluate whether a broadened TSH range up to 4.0 mU/L is equally safe in terms of DTC recurrence as compared with the recommended low-normal TSH goal range (0.5–2.0 mU/L)
Methods:
A retrospective, population-based cohort study was conducted using data from the Ontario Cancer Registry, covering the period from 2007 to 2018
Serum TSH values and their measurement dates were obtained from the Ontario Laboratories Information System, which captures nearly all outpatient laboratory tests in Ontario
The study included patients ≥ 18 years of age, diagnosed with DTC, and with available follow-up information, including at least one TSH value recorded during follow-up
Patients were followed for TSH measurements and DTC recurrence starting from the index date, defined as 12 months after thyroidectomy
The primary outcome was the time from the index date to DTC recurrence
Recurrence was defined as death due to DTC or the need for additional treatment, including new surgery (thyroidectomy or neck dissection) or RAIT, after the index date
TSH was treated as a time-dependent covariate, updated every 90 days if a new TSH measurement was available
TSH levels were classified into mutually exclusive categories, with TSH >2 to ≤4 mU/L as the primary exposure and TSH 0.5–2 mU/L as the reference category
Secondary exposures included TSH <0.5 mU/L and TSH >4 mU/L
Results:
A total of 26,336 patients were included; 21% underwent hemi-thyroidectomy, 41% total thyroidectomy, and 38% total thyroidectomy combined with RAIT
The median follow-up was 5.9 years (interquartile range [IQR], 3.6–8.6) from the index date and the median TSH was 0.6 mU/L (IQR, 0.1–1.8)
During the follow-up period, there were 2,817 cases of DTC recurrence (10% of the cohort), including 103 DTC-specific deaths (0.3%)
No significant increase in recurrence risk was observed with each additional 3 months of cumulative exposure to TSH levels between 2 and 4 mU/L as compared with 0.5–2 mU/L (hazard ratio [HR] 0.99, confidence interval [CI], 0.97–1.02; P = 0.55):
However, a significantly higher risk of DTC recurrence was associated with each additional 3 months of cumulative exposure to TSH levels > 4 mU/L as compared with 0.5–2 mU/L (HR, 1.07; CI, 1.04–1.09; P<0.01)
The risk of composite recurrence increased in a dose-dependent manner with longer exposure to TSH >4 mU/L:
For instance, after 4 years of cumulative exposure to TSH > 4 mU/L:
The adjusted HR was 2.86 (CI, 1.88–4.08)
These findings were consistent when analyses were stratified by baseline treatment and when the index date was adjusted from 12 to 18 months
Conclusions:
Patients with low-risk DTC may safely maintain TSH levels within the higher normal range without increasing the risk of thyroid tumor recurrence:
Accordingly, serum TSH targets could be broadened to 0.5 to 4 mU/L in patients with low-risk DTC
Summary:
This large, population-based cohort study provides evidence that maintaining TSH levels between 2 and 4 mU/L in low-risk DTC patients results in recurrence rates similar to those of the 0.5–2 mU/L range recommended by the 2015 ATA guidelines
Although earlier observational studies proposed a threshold of 2 mU/L as optimal for differentiating recurrence-free survival from thyroid carcinoma–related deaths and recurrences, confirmatory large-scale studies have been lacking
As such, guidelines were based largely on low-quality evidence
The potential for broadening TSH target ranges also carries significant health care implications:
Managing thyroid cancer in the United States is projected to cost over $3.5 billion by 2030
Relaxing TSH targets could reduce health care costs by decreasing the frequency of blood tests and lessening the need for intensive monitoring
From a clinical standpoint, a less stringent TSH range could improve patient compliance
Fewer blood tests would not only reduce stress but could also enhance quality of life
A more uniform dosing regimen, without the need for frequent adjustments to maintain a strict TSH target, could simplify treatment and make it more manageable for patients
A broader TSH range is particularly beneficial for frailer patients, particularly those with comorbidities like atrial fibrillation or osteoporosis, since it may reduce the risk of inadvertently causing subclinical hyperthyroidism
On the other hand, TSH should not exceed 4 mU/L
In this study, a TSH > 4 mU/L was associated with a higher risk of DTC recurrence, and previous studies also linked TSH > 4 mU/L to increased risks of cardiovascular disease, dysrhythmias, and fractures as compared with patients whose TSH levels are within the reference range
Despite its findings, this study has some limitations
It does not provide detailed pathological data, which hampers our ability to precisely assess the ATA risk classification of these tumors
Additionally, recurrences were recorded only if they required treatment, meaning that some recurrences may not have been captured
This highlights the need for further comprehensive studies, especially with longer follow-up periods, to confirm these results
This is particularly important in patients who undergo lobectomy, where the optimal TSH target and the decision to start levothyroxine remain areas of ongoing debate
In conclusion, this study provides valuable reassurance regarding a broader TSH range of 0.5 to 4 mU/L; however, further research is needed to refine treatment protocols and guide clinical decision-making.
Key points:
In patients with low-risk differentiated thyroid cancer (DTC), TSH levels from 0.5 to 4 mU/L were not associated with an increase in cancer recurrence in a retrospective population-based analysis
There was an increased risk of recurrence in patients with low-risk DTC when TSH was > 4 mU/L, whereas maintaining TSH levels within the higher normal range may be safe and does not increase the risk of thyroid tumor recurrence
Broadening the serum TSH target to 0.5 to 4 mU/L in patients with low-risk DTC could be considered
References:
McGriff NJ, Csako G, Gourgiotis L, et al. Effects of thyroid hormone suppression therapy on adverse clinical outcomes in thyroid cancer. Ann Med. 2002; 34(7-8):554-564.
Diessl S, Holzberger B, Mäder U, et al. Impact of moderate vs stringent TSH suppression on survival in advanced differentiated thyroid carcinoma. Clin Endocrinol (Oxf) 2012;76(4):586-592.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016;26:1-133. 4. Jonklaas J, Sarlis NJ, Litofsky D, et al. Outcomes of patients with differentiated thyroid carcinoma following initial therapy. Thyroid2006;16(12):1229-1242.
It is important to stage patients with locoregional recurrences:
As approximately one-third:
Will present with synchronous distant metastasis
If the staging workup is negative:
A complete axillary dissection should be performed if possible
If surgical resection is not possible:
Systemic therapy should be offered:
To potentially allow surgical resection
Radiation should be performed if feasible for recurrences as well:
Depending on the prior extent of radiation delivered
In addition, complete breast imaging:
Should be performed to ensure there is no in-breast recurrence as well
The use of systemic therapy should be offered after a multidisciplinary discussion taking into account tumor phenotype and prior therapies already received by the patient
Wapnir et al:
Demonstrated in the CALOR trial that in ER negative (ER-) isolated recurrences:
Giuliano AE, Ballman K, McCall L, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: long-term follow-up from the American College of Surgeons Oncology Group (Alliance) ACOSOG Z0011 randomized trial. Ann Surg. 2016;264:(3):413-420.
Neuman HB, Schumacher JR, Francescatti AB, et al. Risk of synchronous distant recurrence at time of locoregional recurrence in patients with stage II and III breast cancer (AFT-01). J Clin Oncol. 2018;36(10):975-980. 3. National Comprehensive Cancer Network (NCCN) Breast CancerOnline: https://www.nccn.org/professionals/physician_gls/recently_updated.aspx. Accessed September 15, 2020
Wapnir IR, Price KN, Anderson SJ, et al. Efficacy of chemotherapy for ER-negative and ER-positive isolated locoregional recurrence of breast cancer. Final analysis of the CALOR Trial. N Engl J Med. 2018;36(11):1073-1079.
Should take into account the specific variant identified
Most of the risk data is based on frameshift variants:
Such as 1100delC:
With an estimated absolute lifetime breast cancer risk of 20% to 40%
The risks associated with other types of CHEK2 variants are not as well defined:
However, breast cancer risks associated with the specific missense variant Ile157Thr have been studied in more depth
Data from multiple studies, such as a large case-control study including 10,860 breast cancer patients from The CHEK2 Breast Cancer Case-Control Consortium:
Found a significantly increased risk of breast cancer with the 1100delC variant (OR 2.34; 95% CI 1.72-3.20; p=0.0000001)
Another similar study including 44,777 breast cancer patients:
Also demonstrated a significantly increased risk for breast cancer with the 1100delC variant (OR 2.26; 95% CI 1.90-2.69; p=2.3×10-20)
Unlike the 1100delC variant:
The Ile157Thr variant has been associated with a more modest elevation in risk for breast cancer
A meta-analysis of case-control studies, including 26,336 cases and 44,219 controls, demonstrated an association of the Ile157Thr variant with breast cancer (OR=1.58; 95% CI 1.42-1.75; p<0.000001)
Current National Comprehensive Cancer Network guidelines regarding frameshift CHEK2 variants:
Recommend beginning annual mammograms at 40 years old
Considering breast MRI starting at 30 to 35 years old
Evidence is inadequate to recommend risk reducing mastectomy (RRM)
On the other hand, supplementary breast cancer risk management for patients with the missense variant Ile157Thr is not suggested:
However, management should still be personalized based on family history, for instance:
Beginning breast imaging 5 to 10 years earlier than the youngest family member diagnosed with breast cancer
CHEK2 Breast Cancer Case-Control Consortium. CHEK2*1100delC and susceptibility to breast cancer: A collaborative analysis involving 10,860 breast cancer cases and 9,065 controls from 10 studies. Am J Hum Genet. 2004;74(6):1175-1182. doi:10.1086/421251