Haymart MR, Banerjee M, Stewart AK, Koenig RJ, Birkmeyer JD, Griggs JJ. Use of radioactive iodine for thyroid cancer. JAMA. 2011;306(7):721–728.
Type:
Observational cohort using the National Cancer Database (NCDB) and SEER registries from 2004 to 2008
Population:
189,219 adult patients with well-differentiated thyroid cancer (papillary or follicular) who underwent total thyroidectomy at 981 U.S. cancer centers
Objectives:
Analyze trends in RAI usage from 1990 to 2008
Identify patient-, tumor-, and hospital-level predictors of RAI administration
Assess variation in use across centers, adjusted for disease severity
Key Findings:
Rising Use Over Time
RAI utilization increased significantly across all tumor sizes between 1990 and 2008
Variation Driven by Non-Clinical Factors
Patient / tumor characteristics explained ~21% of variation in RAI use
Hospital traits (type, volume) accounted for ~17%, and 29% remained unexplained, suggesting practice pattern influence
Disease Stage and Use:
Compared to Stage IV:
Patients with Stage I disease were much less likely to receive RAI (OR 0.34), but Stage II / III use was similar to Stage IV (OR ~1)
Regional Disparities:
Rate of RAI use for low-, medium-, and high-risk disease varied by region (49% to 66%):
Indicating inconsistency in treatment approaches
Clinical Implications:
Overuse concern:
Increasing RAI use even in low-risk settings raises questions about overtreatment
Practice patterns matter:
Institutional priorities and physician preferences strongly influenced whether patients received RAI, beyond tumor biology
Guideline alignment needed:
The lack of deficit-stage conformity highlights a need to standardize RAI delivery based on risk stratification, not provider bias
Takeaway for Expert Surgeons:
Recognize that RAI is often employed inconsistently, even for Stage II to III disease, despite limited evidence of benefit in these groups
Encourage benchmarking and quality initiatives within institutions to ensure RAI administration aligns with ATA risk-based guidelines
Educate multidisciplinary teams that evidence-based risk stratification should dictate RAI use, minimizing unnecessary exposure for patients with lower-stage disease
If multi-gland disease (MGD) in primary HPT is known preoperatively:
Genetic testing should be considered prior to operation:
As this may further change the operative approach
There are two distinct operative approaches in MGD:
Total parathyroidectomy with auto-transplantation (TP)
Sub-total parathyroidectomy (STP):
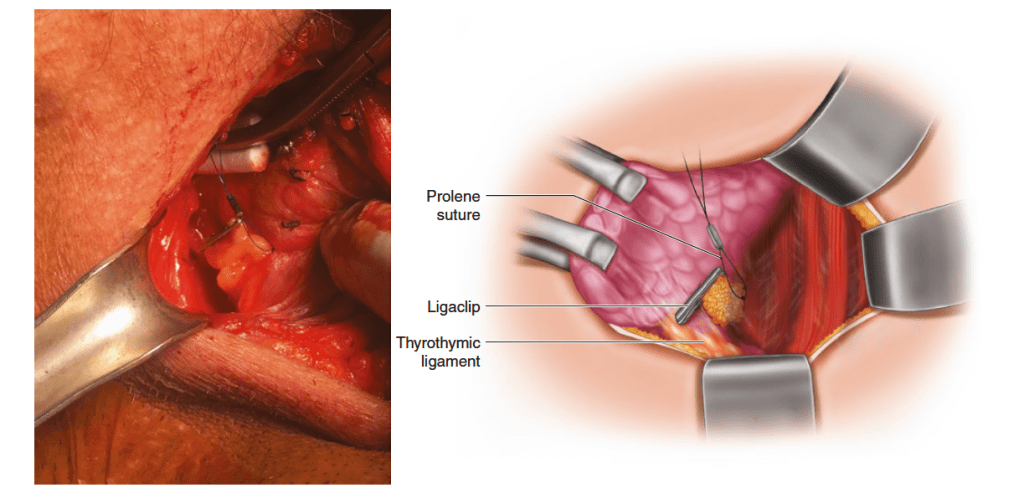
In a sub-total parathyroidectomy, the most normal appearing gland is chosen to be the remnant (ideally an inferior gland):
Which is then cut back to approximately the size of a normal gland
The gland is subsequently tagged with a Prolene suture:
Cut 1 to 2 cm long with a Hemoclip on the ends:
Which will aid in identification should re-exploration be required
Care should be taken not to compromise the vascular supply of the gland with this suture
Tagging of the remnant gland in sub-total parathyroidectomy. The gland chosen to be the remnant has been cut back to approximately the size of a normal gland. The gland is subsequently tagged with a Prolene suture, cut 1 to 2 cm long with a Hemaclip on the ends, which will aid in identification should re-exploration be required. Care should be taken not to compromise the vascular supply of the gland with this suture
Each approach carries different risks, benefits, and indications, as shown in the Table:
Which should always be considered with regard to the patient and his or her underlying pathology (e.g., genetic syndrome, tertiaryHPT)
Risks, benefits, and indications for sub-total and total parathyroidectomy
Other important considerations when dealing with MGD include:
Cervical thymectomy:
Due to the increased risk of ectopic supernumerary glands in MGD
Cryo-preservation of resected tissue:
Should be performed to protect against the rare, though devastating, complication of permanent hypoparathyroidism due to graft or remnant failure
If available, iPTH can be used to help guide the extent of resection in sub-total:
Aiming for a greater than 90% reduction at the completion of the operation
Close observation postoperatively for hypoparathyroidism and hungry bone syndrome regardless of approach
While all patients with symptomatic primary hyperparathyroidism (PHPT) should consider surgery (95% of patients are usually symptomatic when appropriate history is taken):
It is also indicated in some asymptomatic patients (5% of the cases of PHPT):
The normal feedback on parathyroid hormone production by extracellular calcium seems to be lost:
Resulting in a change in the set point
In primary hyperparathyroidism from parathyroid hyperplasia:
An increase in the cell numbers is probably the cause of the change in the set point
The chronic excessive resorption of calcium from bone caused by excessive parathyroid hormone can result in:
Osteopenia
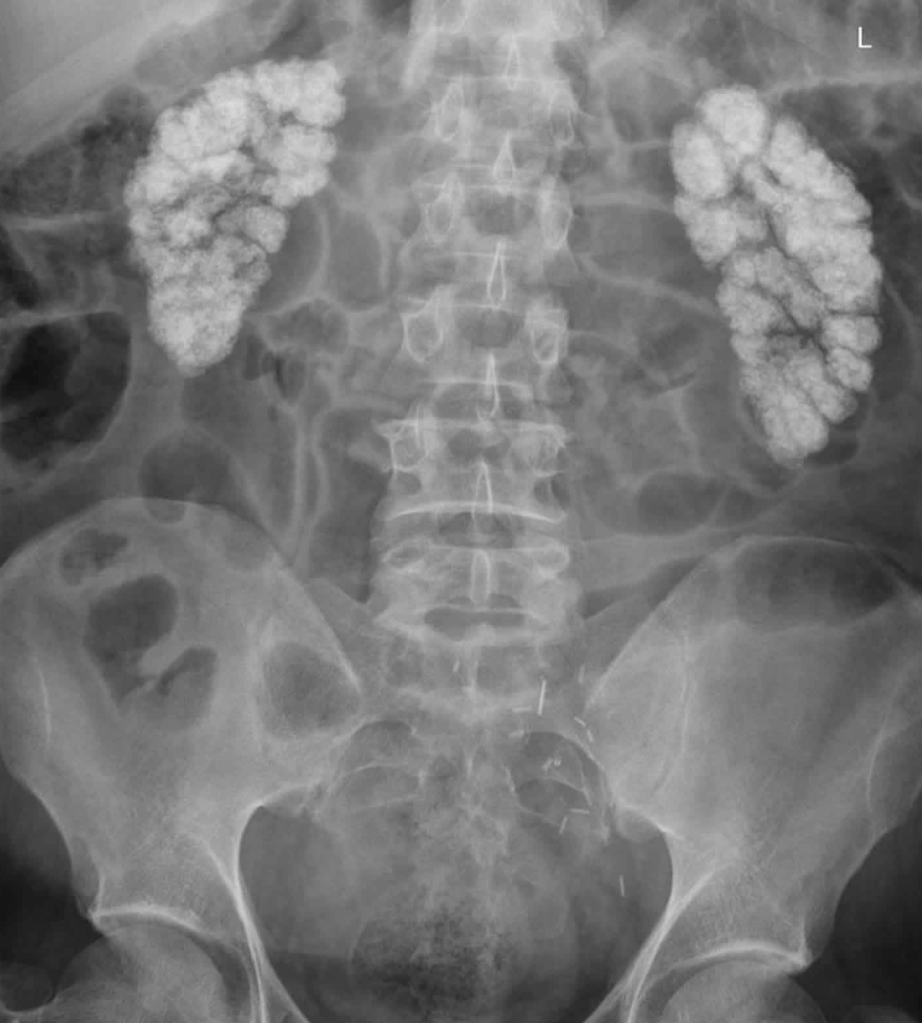
In severe cases, this may result in osteitis fibrosa cystica:
Which is characterized by subperiosteal resorption of the distal phalanges, tapering of the distal clavicles, salt-and-pepper appearance of the skull, and brown tumors of the long bones
This is not commonly seen now
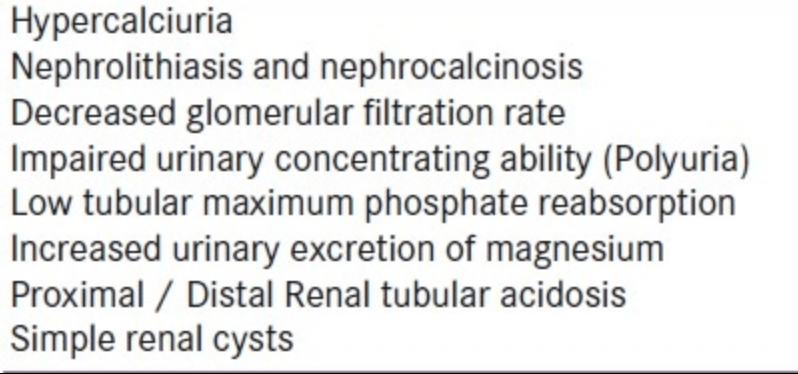
In addition, the chronically increased excretion of calcium in the urine:
Can predispose to the formation of renal stones
The other symptoms of hyperparathyroidism:
Are due to the hypercalcemia itself:
And are not specific to hyperparathyroidism
These can include:
Muscle weakness
Fatigue
Volume depletion
Nausea and vomiting
In severe cases, coma and death
Neuropsychiatric manifestations are particularly common and may include:
Depression
Confusion
Subtle deficits that are often characterized poorly and may not be noted by the patient (or may be attributed to aging)
Increased calcium can increase gastric acid secretion, and persons with hyperparathyroidism:
May have a higher prevalence of peptic ulcer disease
Rare cases of pancreatitis have also been attributed to hypercalcemia
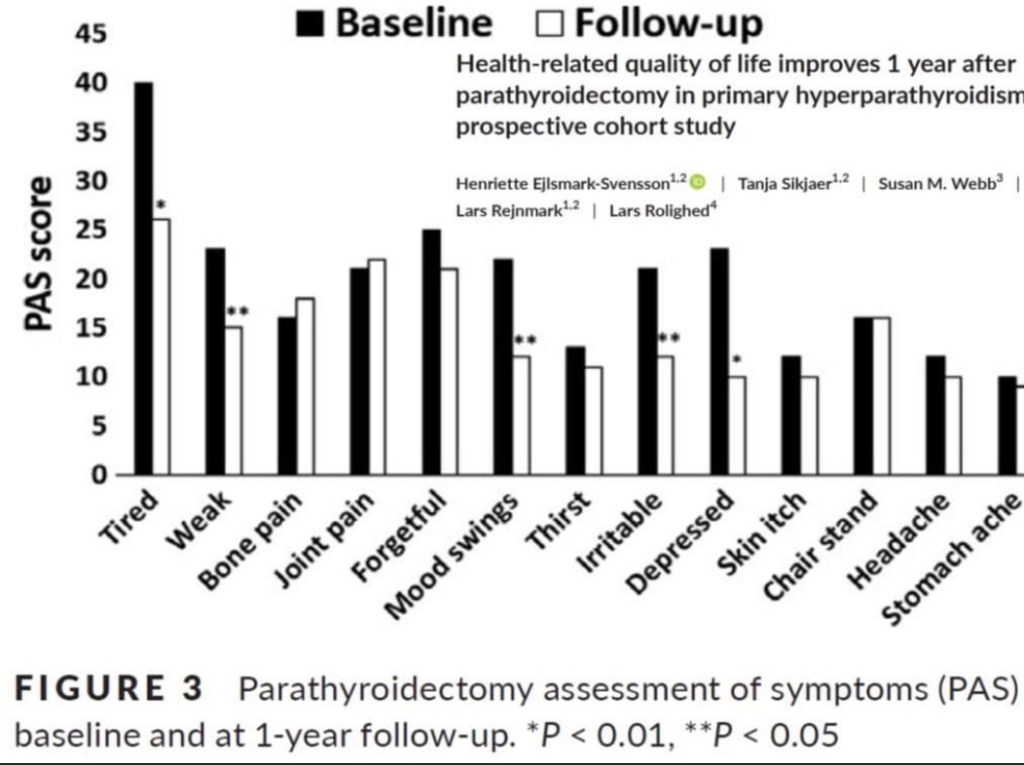
A prospective cohort study by Ejlsmark-Svensson et al:
Reported that in patients with primary hyperparathyroidism, quality-of-life questionnaire scores were significantly lower:
In association with moderate-severe hypercalcemia:
Than in relation to mild hypercalcemia:
However, quality of life did not seem to be related to the presence of organ-related manifestations of primary hyperparathyroidism, such as osteoporosis, renal calcifications, and renal function impairment
This suggests that hypercalcemia is the primary driver of an impaired quality of life
Retrospective Low–Intermediate Series (6) (Italy, 2024):
RAI reduced recurrence by 42%:
9.6% vs 15.9% using inverse‑probability regression in patients with ≥ 2 intermediate risk factors
Polish Prospective RAI Dose Trial (Arch Med Sci, 2022): (7)
Intermediate-risk group receiving 60 vs 100 mCi:
Had similar excellent response (~ 85%), low structural recurrence (~ 6.5%), and excellent long-term outcomes
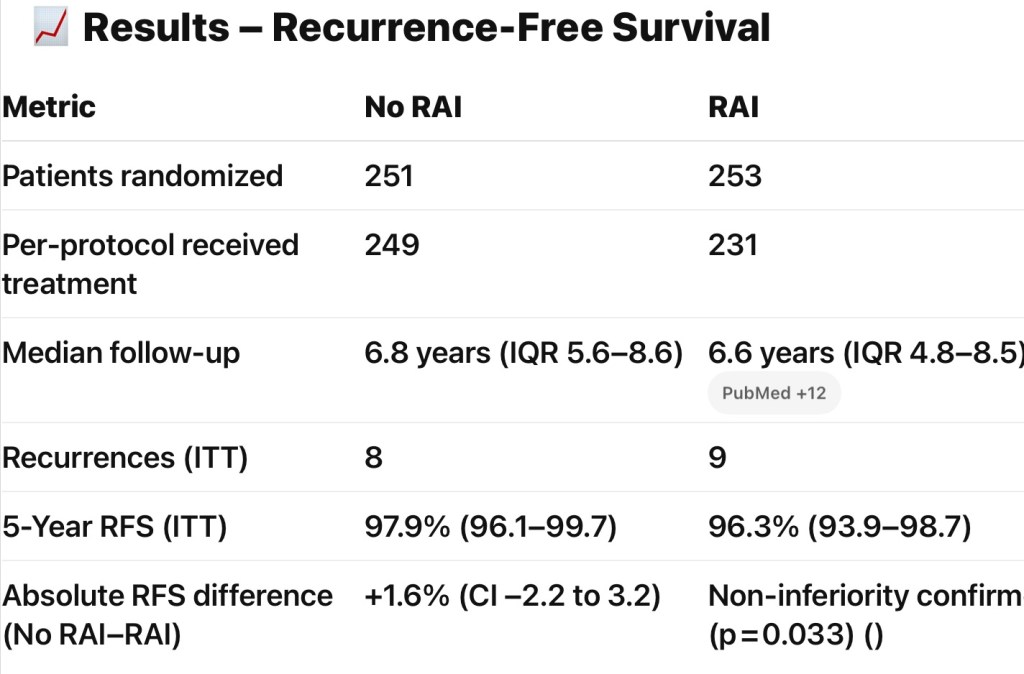
Prospective / Clinical Trials:
No RCTs isolating intermediate-risk exist:
However, the rhTSH + RAI Prep trial included many intermediate-risk patients (n ≈ 307) and found non-inferiority of rhTSH vs withdrawal for RAI effectiveness (8)
Guideline Position Statements:
The 2015 ATA guidelines recommend selective use of RAI in intermediate-risk DTC based on individual risk features, with a weak recommendation and low-quality evidence (1)
The 2022 European Thyroid Association / EANM consensus also supports personalized RAI use in this group, prioritizing shared decision-making and individual risk-benefit assessment (9)
Clinical Take‑Home Points:
Selective RAI yields a survival / recurrence benefit:
Strongest in older patients or those with > 1 intermediate risk feature
Low-intermediate risk (e.g., single small node, microscopic ETE):
1. Haugen BR, et al. 2015 ATA Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1–133.
2. Nixon IJ, et al. The impact of RAI on survival in intermediate-risk patients: SEER analysis. Ann Surg Oncol. 2012;19(6):2025–33.
3, Haymart MR, et al. Radioactive iodine in thyroid cancer: SEER-based outcomes. JAMA. 2011;306(7):721–8.
4. Mazzaferri EL, et al. Management of differentiated thyroid cancer: Mayo Clinic experience. J Clin Endocrinol Metab. 2001;86(4):1447–63.
5. Lam AK, et al. RAI impact on lymph node recurrence: Hong Kong cohort study. Cancer. 2005;103(5):920–9.
6. Prete A, et al. Benefit of RAI in intermediate-risk DTC patients with multiple features. Endocrine. 2024;84(1):123–131.
7. Piciu D, et al. Prospective evaluation of 60 vs 100 mCi in intermediate-risk thyroid cancer. Arch Med Sci. 2022;18(4):1002–1012.
8. Mallick U, et al. Preparation for RAI: rhTSH vs withdrawal in low- and intermediate-risk patients. Lancet. 2012;379(9825):823–830.
9. Luster M, et al. EANM/ETA consensus on RAI therapy in thyroid cancer. Eur J Nucl Med Mol Imaging. 2022;49(1):13–25.