Vermorken JB, Remenar E, van Herpen C, et al. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med. 2007;357(17):1695–704. 【TAX 323】
Posner MR, Hershock DM, Blajman CR, et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med. 2007;357(17):1705–15. 【TAX 324】
NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers. Version 2.2025.
Hitt R, et al. Phase III study comparing TPF with PF in locally advanced head and neck cancer. J Clin Oncol. 2005;23(34):8636–45.
Colevas AD, et al. Chemotherapy options for patients with cisplatin-ineligible head and neck cancer. J Clin Oncol. 2018;36(19):1942–50.
RNA whole-transcriptome classifier optimized as a rule-out test:
XA adds variants / fusions if GSC is Suspicious PMCVeracyte
ThyroSeq v3 GC:
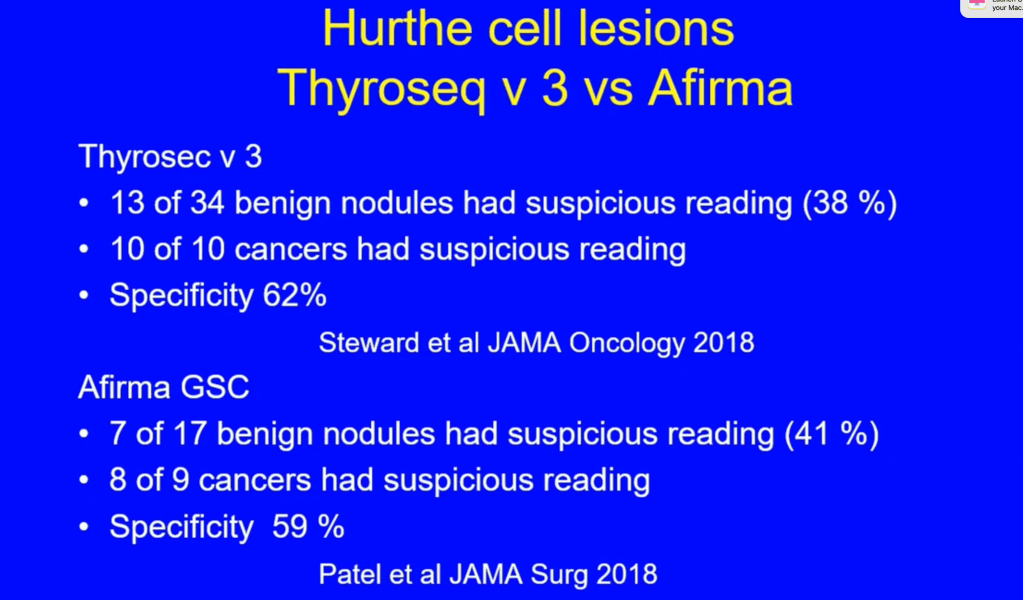
DNA / RNA next-gen panel across many genes (mutations, fusions, copy-number alterations, helpful in oncocytic cell lesions / Hürthle cell lesions) designed for rule-out + rule-in and therapy-relevant profilingJAMA NetworkThyroSeq
ThyGeNEXT + ThyraMIR v2 (Interpace):
Two-step oncogene panel → reflex miRNA classifier; aims for balanced rule-out with stronger rule-in when driver / miRNA high-risk pattern is present PMCThygenext Thyramir
Performance (typical ranges in Bethesda III–IV):
Afirma GSC:
High sensitivity / NPV in VS and real-world cohorts:
PPV modest to moderate
Many studies report:
NPV ~ 94% to 97%
PPV ~ 45% to 65%
Real-world series show improved yield vs validation PMCScienceDirect
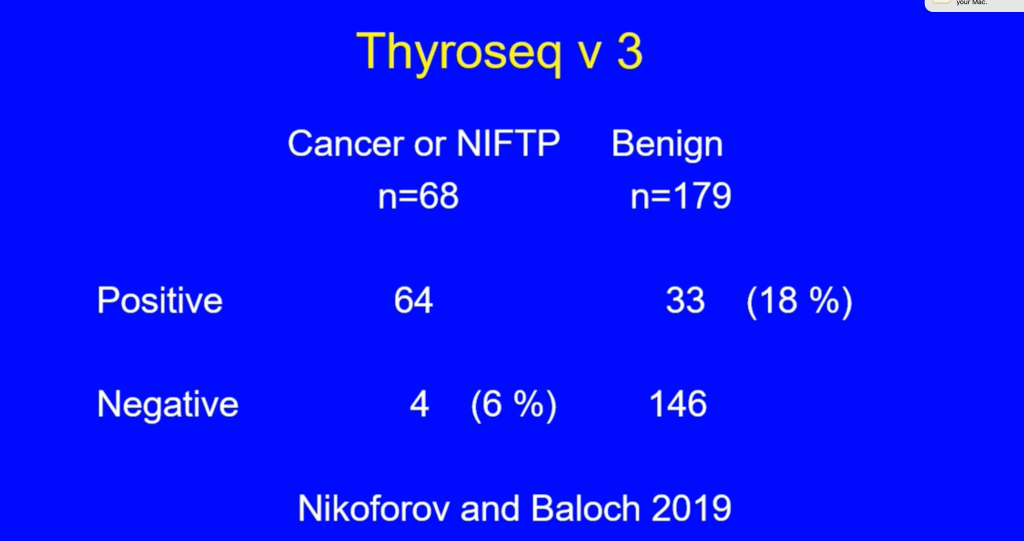
ThyroSeq v3:
Validation and multi-center series show high sensitivity / NPV with higher PPV than Afirma in several cohorts:
2025 systematic review suggests high surgical avoidance rates among platforms PMCResearchGate
Prognostic/management information (actionability):
Afirma GSC + XA:
If Suspicious, XA reports fusions / variants (e.g., RET, NTRK, ALK):
Which can guide targeted therapy decisions down the line
GSC itself primarily aids avoiding surgeryVeracyte
ThyroSeq v3:
Reports BRAF, RAS, TERT-p, RET / NTRK/ ALK, gene expression and copy-number profiles:
Useful for risk stratification (e.g., TERT / BRAF V600E for aggressiveness) and for operative planning (extent, LN assessment) and potential targeted options
If you want both strong rule-out and richer “what kind of cancer is this if positive?” detail to guide extent of surgery and future therapy:
ThyroSeq v3 generally provides more granular prognostic / actionable data (TERT/driver profile, CNA burden, Hürthle copy-number signature) and often a higher PPV than Afirma
This makes it my usual pick when operative planning may hinge on genotype JAMA NetworkThyroSeq
If you favor a stepwise, cost-conscious approach with meaningful rule-in capability when drivers /miRNA are high-risk:
ThyGeNEXT + ThyraMIR v2 is reasonable:
Pooled data show competitive NPV and good surgical-avoidance rates PMCResearchGate
Practical take for your clinic:
For Bethesda III to IV nodules with indeterminate US where you want to minimize unnecessary operations and inform extent if positive:
ThyroSeq v3 is the most versatile single test today
For surgeon’s “rule-out first” workflows with straightforward nodules and low pretest risk:
Afirma GSC is perfectly acceptable:
Add XA if suspicious and you want therapy targets.
For equivocal cases where a rule-in signal would materially change from surveillance to surgery, or when prior testing is ambiguous:
ThyGeNEXT + ThyraMIR v2 is a solid option
Interpretation & Take-Home
Best Rule-Out (Highest NPV and Sensitivity):
Afirma GSC (real-world meta-analysis: SN ~97%, NPV ~99%) and ThyroSeq v3 (UCLA trial: SN 97%, NPV 99%) are essentially neck-and-neck in ruling out malignancy. Both demonstrate excellent reliability in avoiding unnecessary surgeries.
Better Rule-In (Higher PPV):
ThyroSeq v3 edges ahead slightly with PPV ~64% versus Afirma’s ~57% in comparable settings, meaning a positive result is more likely to indicate true malignancy.
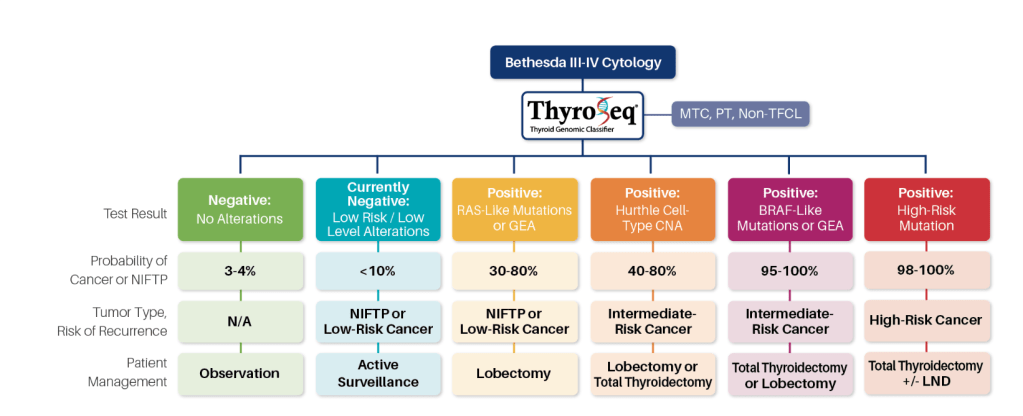
ThyroSeq® test results refine cancer probability in thyroid nodules with indeterminate cytology, informing the most appropriate management of these patients
According to NCCN guidelines, if molecular testing, in conjunction with clinical and ultrasound features, predicts a risk of cancer comparable to the risk of malignancy seen in a benign FNA cytology (roughly 5% or less):
Active surveillance can be considered
Therefore, in those clinical situations where the pretest probability of cancer in nodules with Bethesda III and IV cytology is less than 44%:
A negative ThyroSeq test results would confer the cancer probability of 5% or less:
Justifying observation in lieu of surgical management in appropriately selected cases
Because the probability of cancer in such nodules is comparable to benign FNA cytology, the management of patients may follow the recommendations for nodules with benign cytology:
Which, based on the 2015 ATA guidelines, should be determined based on ultrasound (US) pattern (Recommendation #23)
In nodules with Bethesda V cytology and negative ThyroSeq result:
The residual cancer risk of ~20% does not allow to avoid surgical management:
Thyroid lobectomy may be sufficient initial treatment for many of these patients
Currently Negative Results:
Test results are reported as currently negative:
When the sample is found positive for a low risk and / or low-level gene mutation, DNA copy number alterations (CNA) or gene expression alterations (GEA) that alone is not sufficient for full cancer development
Although at the time of sampling most of these nodules are benign:
Some of them may undergo clonal expansion and acquire additional mutations
In the absence of suspicious US features or other clinical risk factors:
Many of these patients are likely to benefit from active surveillance with repeat of clinical exam and potentially FNA and molecular testing in 1 year
Positive RAS-Like or GEA Results:
ThyroSeq test positive for an isolated RAS mutation or RAS-like alteration (e.g. BRAF K601E mutation, THADA fusion, RAS-like GEA):
Indicates that the nodule is a tumor (not hyperplasia) and predicts, depending on the specific alteration:
A 30% to 80% probability of either a low-risk cancer or a pre-cancerous tumor, NIFTP
Many of these nodules may be managed by therapeutic lobectomy:
Which is currently recommended by the ATA guidelines for low-risk papillary and follicular carcinomas (Recommendation #35) and NIFTP
Positive BRAF-Like of GEA Results:
ThyroSeq test positive for an isolated BRAF V600E or BRAF V600E-like alteration (e.g. RET / PTC, BRAF fusions, BRAF V600E-like GEA):
Confers a very high (greater than 95%) probability of cancer
According to the ATA guidelines:
BRAF-mutated unifocal intrathyroidal carcinoma less than 1 cm in size has low risk for recurrence:
Therefore may be treated with thyroid lobectomy alone
Whereas 1 cm to 4 cm BRAF-positive PTC is an intermediate-risk tumor:
Where total thyroidectomy or lobectomy should be considered based on clinical and US findings
Postive Oncocytic Cell Type (formely Hurthle Cell Type) CNA Results:
ThyroSeq test positive for isolated oncocytic cell type / Hürthle cell-type copy number alterations (CNA) confers, in different nodule size groups:
A 40% to 80% probability of Hürthle Cell carcinoma:
Whereas the rest of these nodules are benign Hurthle Cell adenomas
Positive High Risk Mutations Results:
ThyroSeq test positive for multiple high-risk mutations (e.g. BRAF V600E and TERT) confers a very high probability of cancer and predicts an increased risk of disease recurrence by the ATA guidelines and of tumor-related mortality
Most of these patients would likely benefit from total thyroidectomy, with possible consideration for regional lymph node dissectionif one of the mutations is BRAFV600E
A unique feature of ThyroSeq as compared to other molecular tests for thyroid FNA samples is that, in addition to the diagnostic utility:
It provides information that helps to prognosticate cancer pre-operatively
Based on the current thyroid cancer management guidelines from the ATA, cancer risk stratification is important in:
Determining the appropriate extent of surgery (lobectomy vs total thyroidectomy ), radioactive iodine (RAI) administration, and intensity of follow-up
Most thyroid cancers are indolent and these patients are at low risk for disease recurrence after cancer removal:
These patients can be treated by lobectomy and are unlikely to benefit from RAI ablation and TSH suppression
Similarly, surgical excision of a pre-cancer tumor:
NIFTP, by lobectomy is likely to be curative since the risk of tumor recurrence is less than 1%
On the other hand, patients with high-risk cancers would benefit from up-front total thyroidectomy:
Which facilitates post-operative RAI administration and disease monitoring
ThyroSeq is the only molecular test that provides cancer risk assessment pre-operatively based on the analysis of multiple mutational markers associated with cancer prognosis
Specifically, finding of single RAS mutations or RAS-like mutations without other higher-risk mutations tested by ThyroSeq is associated with:
A low risk for recurrence
Whereas identification of isolated BRAF V600E and other BRAF V600E-like mutations is associated with:
An intermediate risk for disease recurrence (Yip et al. Ann Surg, 2015)
Identification of TERT promoter mutations, and specifically the co-occurrence of TERT with other, early driver mutations or finding of multiple cancer driver mutations is associated with:
A high risk for cancer recurrence (Nikiforov YE. Endocrine Practice, 2017)
Importantly, cancer prognostication requires the analysis of all genes associated with thyroid cancer behavior which are included in the ThyroSeq panel
For example, the finding of RAS mutation by a small panel of genes carries no prognostic information, because while an isolated RAS mutation confers a low risk of disease reoccurence:
The coexistence of RAS with TERT or TP53 gene mutations is a molecular signature of a high-risk cancer (Nikiforova et al. 2016)
In addition, the ThyroSeq test is able to diagnose a high-risk cancer in nodules which may be very small and have no particularly worrisome ultrasonographic features:
As an illustration, a tumor as small as 0.6 cm may already have a molecular signature of aggressive thyroid cancer developed (Shrestha RT et al. Thyroid. 2015)
Parathyroid tissue emits intrinsic autofluorescence in the NIR spectrum:
Peaking at around 820 to 830 nm
The specific fluorophore responsible is still under investigation:
But mitochondrial content and calcium-sensing receptors have been implicated
Key Milestones in the Literature:
2011:
First Description:
Paras et al., J Biomed Optics: Described intrinsic autofluorescence of parathyroid glands using NIR light in animal models and humans
Sensitivity and specificity for parathyroid detection were promising:
Initially ~ 80% to 90%
2015 to 2018:
Early Clinical Studies:
McWade et al., Surgery (2016):
Showed high sensitivity (97%) and specificity (95%) in parathyroid identification using NIR autofluorescence
Autofluorescence was effective without contrast agents
Faster identification of parathyroids during thyroidectomy
2018 to 2021:
Commercial Devices & Validation Fluobeam®, PTeye®, and EleVision IR became available
Systematic reviews and meta-analyses (e.g., Demarchi et al., 2019, Ann Surg Oncol) confirmed:
Higher parathyroid identification rates
Reduced inadvertent parathyroidectomy
Improved preservation of gland vascularity
2021 to 2024:
Comparative & Outcome Studies:
Meta-analyses (e.g., Wang et al., Langenbecks Arch Surg, 2022):
NIR autofluorescence vs. white light: reduced transient hypocalcemia (RR ~ 0.42)
Time to identify parathyroid was significantly shorter (mean ~ 4 min faster)
Zhao et al., JAMA Otolaryngol Head Neck Surg (2023):
Showed that NIR imaging decreased inadvertent excision and increased confidence in preserving parathyroids
Combination with Indocyanine Green (ICG) angiography has been studied to assess gland viability after identification
Clinical Applications:
Parathyroid preservation in thyroidectomy
Localization in reoperative neck surgery
Autotransplantation planning
Training tool for junior surgeons
Limitations:
Autofluorescence intensity can vary between patients and may be affected by lighting, fat tissue, or gland pathology
Does not assess vascularization; ICG angiography is needed for viability
Cost and device availability may be limiting factors in community hospitals
Conclusion:
Autofluorescence has emerged as a reliable, non-invasive, and real-time tool for parathyroid gland identification
The technique has consistently shown benefits in reducing complications such as hypocalcemia, minimizing gland devascularization, and enhancing surgical efficiency
Combining NIR autofluorescence with ICG fluorescence may offer a comprehensive approach to both identifying and preserving functional parathyroid glands
Key References:
Paras C et al. J Biomed Opt. 2011;16(6):067004.
McWade MA et al. Surgery. 2016;159(3):865-871.
Demarchi MS et al. Ann Surg Oncol. 2019;26(1):165-172.
Wang X et al. Langenbecks Arch Surg. 2022;407(2):655–664.
Zhao H et al. JAMA Otolaryngol Head Neck Surg. 2023;149(4):359–367.
Is the standard of care for patients with locally advanced head and neck squamous cell carcinoma (HNSCC):
With the most widely accepted regimen being cisplatin 100 mg/m² administered intravenously every 3 weeks for up to three cycles during radiotherapy
This approach is supported by multiple large randomized trials demonstrating survival benefit in patients with good performance status and is endorsed by major guidelines, including those from the American Society of Clinical Oncology and NCCN.
The rationale for exploring low-dose weekly cisplatin (20 to 50 mg/m²):
Stems from the significant acute and chronic toxicities associated with the high-dose regimen, including:
Nephrotoxicity, ototoxicity, and myelosuppression:
Which can limit compliance and preclude delivery of the intended cumulative dose
Weekly regimens are hypothesized to:
Improve tolerability and allow more patients to achieve a cumulative cisplatin dose of at least 200 mg/m²:
Which is considered important for optimal tumor control
Efficacy: Survival and Disease Control:
Meta-analyses and large retrospective studies indicate that overall survival and response rates are similar between high-dose and low-dose cisplatin regimens in the definitive chemoradiation setting:
For example, a large population-based study in US veterans found no significant difference in overall survival between high-dose (100 mg/m² every 3 weeks) and low-dose (40 mg/m² weekly) cisplatin:
Though high-dose was associated with greater toxicity
Similarly, systematic reviews and meta-analyses have not demonstrated a meaningful survival difference between the two dosing strategies in either definitive or postoperative settings
However, some studies and clinical guidelines suggest that high-dose cisplatin may offer superior locoregional control and overall survival:
Particularly in altered fractionation or postoperative settings
For instance, randomized trials and meta-analyses have reported improved locoregional control and, in some analyses, overall survival with high-dose regimens, especially when combined with altered fractionation radiotherapy
The American Society of Clinical Oncology recommends the every-3-week high-dose regimen as the standard:
Noting that weekly regimens lack level I evidence and may be associated with inferior outcomes in some studies
Achieving a cumulative cisplatin dose of ≥ 200 mg/m² is consistently associated with better survival and locoregional control:
Regardless of the dosing schedule
Toxicity and Compliance:
High-dose cisplatin regimens are associated with increased rates of severe hematologic, renal, and ototoxic toxicities compared to weekly low-dose regimens
In contrast, weekly low-dose cisplatin is generally better tolerated and associated with improved compliance, with more patients able to complete the planned cumulative dose
Notably, patients with low skeletal muscle mass are at higher risk for dose-limiting toxicity with high-dose cisplatin and may particularly benefit from weekly regimens to improve compliance and reduce toxicity
However, some studies have reported increased rates of grade 3 to 4 dysphagia and weight loss with weekly regimens in the postoperative setting
Guideline Recommendations and Ongoing Controversies:
Current US and international guidelines, including those from the American Society of Clinical Oncology:
Continue to endorse high-dose cisplatin (100 mg/m² every 3 weeks) as the standard regimen for concurrent chemoradiation in eligible patients
Weekly low-dose cisplatin is widely used in clinical practice, particularly for patients with comorbidities or poor performance status, but is considered investigational pending results from ongoing prospective trials
The optimal dosing schedule remains an area of active research, and further adequately powered randomized trials are needed to clarify the relative efficacy and toxicity of these regimens, especially in specific subgroups such as HPV-positive, elderly, or comorbid patients
In summary, high-dose cisplatin every 3 weeks remains the standard of care for concurrent chemoradiation in locally advanced HNSCC, with weekly low-dose regimens offering a reasonable alternative for selected patients, particularly those at higher risk for toxicity or with difficulty tolerating high-dose therapy
References:
Head and Neck Cancer. Chow LQM. The New England Journal of Medicine. 2020;382(1):60-72. doi:10.1056/NEJMra1715715.
Management of the Neck in Squamous Cell Carcinoma of the Oral Cavity and Oropharynx: ASCO Clinical Practice Guideline. Koyfman SA, Ismaila N, Crook D, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2019;37(20):1753-1774. doi:10.1200/JCO.18.01921.
Low-Dose vs. High-Dose Cisplatin: Lessons Learned From 59 Chemoradiotherapy Trials in Head and Neck Cancer. Szturz P, Wouters K, Kiyota N, et al. Frontiers in Oncology. 2019;9:86. doi:10.3389/fonc.2019.00086.
Concurrent Chemoradiotherapy With Cisplatin Given Once-a-Week Versus Every-Three Weekly in Head and Neck Squamous Cell Carcinoma: Non-Inferior, Equivalent, or Superior?. Gupta T, Kannan S, Ghosh-Laskar S, Agarwal JP. Oral Oncology. 2022;134:106130. doi:10.1016/j.oraloncology.2022.106130.
Cisplatin Every 3 Weeks Versus Weekly With Definitive Concurrent Radiotherapy for Squamous Cell Carcinoma of the Head and Neck. Bauml JM, Vinnakota R, Anna Park YH, et al. Journal of the National Cancer Institute. 2019;111(5):490-497. doi:10.1093/jnci/djy133.
Weekly Low-Dose Versus Three-Weekly High-Dose Cisplatin for Concurrent Chemoradiation in Locoregionally Advanced Non-Nasopharyngeal Head and Neck Cancer: A Systematic Review and Meta-Analysis of Aggregate Data. Szturz P, Wouters K, Kiyota N, et al. The Oncologist. 2017;22(9):1056-1066. doi:10.1634/theoncologist.2017-0015.
Low Dose Cisplatin Weekly Versus High Dose Cisplatin Every Three Weeks in Primary Chemoradiotherapy in Head and Neck Cancer Patients With Low Skeletal Muscle Mass: The CISLOW-study Protocol. Schaeffers AWMA, Devriese LA, van Gils CH, et al. PloS One. 2023;18(11):e0294147. doi:10.1371/journal.pone.0294147.
Comparison of Standard-Dose 3-Weekly Cisplatin and Low-Dose Weekly Cisplatin for Concurrent Chemoradiation of Patients With Locally Advanced Head and Neck Squamous Cell Cancer: A Multicenter Retrospective Analysis. Lee SY, Choi YS, Song IC, et al. Medicine. 2018;97(21):e10778. doi:10.1097/MD.0000000000010778.
Altered Fractionation Radiotherapy Combined With Concurrent Low-Dose or High-Dose Cisplatin in Head and Neck Cancer: A Systematic Review of Literature and Meta-Analysis. Szturz P, Wouters K, Kiyota N, et al. Oral Oncology. 2018;76:52-60. doi:10.1016/j.oraloncology.2017.11.025.
Comparison of Weekly Administration of Cisplatin Versus Three Courses of Cisplatin 100 mg/M(2) for Definitive Radiochemotherapy of Locally Advanced Head-and-Neck Cancers. Rades D, Seidl D, Janssen S, et al. BMC Cancer. 2016;16:437. doi:10.1186/s12885-016-2478-8.
Schumm MA, Nikiforov YE, Nikiforova MN, et al. Association of BRAF V600E allele frequency with clinicopathologic outcomes in papillary thyroid cancer. J Clin Endocrinol Metab. Epub 2024 Nov 14:dgae774; doi: 10.1210/clinem/dgae774. PMID: 39541427.
Key Points:
BRAF V600E mutation:
Is the most common mutation detected in papillary thyroid carcinoma (PTC)
It is detected in a large variety of cancers, from low- to high-risk tumors
This study suggests that the reason for this variability may be related to the allele frequency (AF) of the mutation:
The proportion of DNA molecules in the sample that carry the mutation
Among 73 patients with an isolated BRAF V600E mutation detected via ThyroSeq v3 molecular testing:
Those with an AF ≥ 35%:
Had a significantly higher risk of recurrence and worse recurrence-free survival
These findings support a more refined approach to managing this common mutation:
Allowing for better preoperative risk assessment:
Patients with low AF may be candidates for lobectomy or active surveillance:
While those with high AF or other risk factors may benefit from more aggressive treatment
Background:
The BRAF V600E mutation is the most common genetic alteration in papillary thyroid cancer (PTC) and is typically reported as either present or absent in clinical practice:
However, allele frequency (AF), which is the proportion of mutated cells within a tumor, varies and may provide additional prognostic insights
This study highlights how advances in molecular diagnostics now allow measurement of AF, offering a potential tool for refining the tumor risk stratification
Methods:
This retrospective cohort study included 73 patients with Bethesda V / VI thyroid nodules confirmed to have BRAF V600E who had surgery with a diagnosis of PTC
Quantitative AF data were obtained through ThyroSeq v3 molecular testing and analyzed in relation to clinicopathologic features
Markers of aggressive tumor behavior included tumor size ≥ 2 cm, gross extrathyroidal extension (ETE), and lymph node metastases
The primary outcomes were disease recurrence and recurrence-free survival (RFS)
Results:
Among the patients with an isolated BRAF V600E mutation:
Median patient age was 45 years
66% were female
88% patients had Bethesda VI cytology
The median BRAF AF was 25.5% (range, 0.5 to 47.3)
Higher AF levels:
Were associated with more aggressive tumor characteristics, including:
Larger tumor size and the presence of gross ETE
Patients with AF ≥ 35%:
Had a significantly higher risk of recurrence and worse RFS (hazard ratio, 7.40; 95% CI, 1.4–38.1)
Overall, after 4.1 years of follow-up:
9.4% of patients experienced disease recurrence, with most cases occurring in those with elevated AF
Allele frequency was not significantly linked to lymph node metastases or positive surgical margins
Conclusions:
Tumors with high BRAF V600E AF were associated with more gross ETE and increased recurrence risk
Preoperative knowledge of AF levels may help guide individualized treatment decisions
BRAF V600E mutation is very common in PTC:
Detected in approximately 50% of cases, and is associated with a wide spectrum of disease, from low- to high-risk tumors
Although it is frequently associated with extrathyroidal extension, lymph node metas- tases, and radioiodine (RAI)-refractory disease:
This mutation is also present in small, indolent tumors and even in occult disease identified at autopsy
This variable clinical presentation has led to ongoing controversy over whether the presence of BRAF mutation, identified either preoperatively or on the pathology report, should guide treatment decisions
For instance, some authors argue that microscopic PTCs are less suitable for active surveillance if they harbor a BRAF mutation
Also, the efficacy of RAI therapy in BRAF-mutated PTC has been questioned, with some studies demonstrating reduced effectiveness, while others report favorable clinical outcomes
The current study is intriguing, as it offers a potential explanation for the variable clinical behavior of BRAF-mutated tumors
Schumm et al. evaluated 73 patients with Bethesda V / VI thyroid nodules positive for BRAF V600E mutation, assessing the allele frequency (AF) of the mutation
This analysis was made possible by the ThyroSeq molecular test, which, in addition to detecting mutations, provides a quantitative assessment of mutation frequency:
For example the proportion of DNA molecules containing the mutation among all DNA molecules obtained from a given fine-needle aspiration sample
The authors identified a clear correlation between AF and tumor aggressiveness, with a clinically actionable threshold of ≥ 35% associated with a higher risk of recurrence
These findings align with several recent studies that demonstrated a correlation between BRAF V600E AF (tested on surgical specimens) and aggressive histologic features
In clinic, patients often express concern upon learning they carry a BRAF mutation, as most online materials and social network groups emphasize its association with aggressive disease and reduced RAI responsiveness
This often leads to overtreatment, even in cases with otherwise low-risk features
The present study introduces a potentially valuable preoperative tool to better stratify risk and guide clinical decisions:
Such as the extent of surgery and the appropriateness of active surveillance
It improves the utility of molecular testing, as BRAF mutations alone have limited prognostic value when reported as binary (yes / no) results, when adjusted for tumor and patient characteristics
Using this approach, a more aggressive treatment strategy can be reserved only for patients with high AF or those with dual BRAF and TERT promoter mutations (which are associated with a more aggressive clinical course)
Conversely, patients with low AF will be suitable for lobectomy or active surveillance
In addition to AF, there are several promising molecular prognostic tools, such as gene expression profiles associated with vascular invasion or sodium–iodide symporter expression, which have the potential to further individualize management based on preoperative genomic analysis
The future looks promising, with increasingly tailored treatment strategies driven by advances in preoperative workup
References:
Schumm MA, Nikiforov YE, Nikiforova MN, et al. Association of BRAF V600E allele frequency with clinicopathologic outcomes in papillary thyroid cancer. J Clin Endocrinol Metab. Epub 2024 Nov 14:dgae774; doi: 10.1210/clinem/dgae774.
Ramone T, Ghirri A, Prete A, et al. Molecular profiling of low-risk papillary thyroid carcinoma (mPTC) on active surveillance. J Clin Endocrinol Metab 2024;dgae575; doi: 10.1210/clinem/dgae575.
Huang Y, Qu S, Zhu G, et al. BRAF V600E mutation-assisted risk stratification of solitary intrathyroidal papillary thyroid cancer for precision treatment. J Natl Cancer Inst 2017;110(4):362-370; doi: 10.1093/jnci/djx227.
Kim KJ, Kim SG, Tan J, et al. BRAF V600E status may facilitate decision-making on active surveillance of low-risk papillary thyroid microcarcinoma. Eur J Cancer 2020;124:161-169; doi: 10.1016/j.ejca.2019.10.017.
Ge J, Wang J, Wang H, et al. The BRAF V600E mutation is a predictor of the effect of radioiodine therapy in papillary thyroid cancer. J Cancer 2020;11(4):932–939; doi: 10.7150/jca.33105.
Zhu G, Deng Y, Pan L, et al. Clinical significance of the BRAF V600E mutation in PTC and its effect on radioiodine therapy. Endocr Connect 2019; doi: 10.1530/EC-19-0045.
Huang J, Wang J, Xv J, et al. Genetic alterations and allele frequency of BRAF V600E and TERT mutation in papillary thyroid carcinoma with intermediate-to-high recurrence risk: a retrospective study. Clin Exp Med 2024;24(1):76; doi: 10.1007/s10238-024-01320-4.
Blazekovic I, Samija I, Perisa J, et al. Association of BRAF V600E mutant allele proportion with the dissemination stage of papillary thyroid cancer. Biomedicines 2024;12(3):477; doi: 10.3390/biomedicines12030477.
Abdulhaleem M, Bandargal S, Pusztaszeri MP, et al. The impact of BRAF V600E mutation allele frequency on the histopathological characteristics of thyroid cancer. Cancers (Basel) 2023;16(1):113; doi: 10.3390/cancers16010113.
“Surgical Management of Invasive Differentiated Thyroid Cancer: An Evidence-Based Review”:
Published in: Thyroid, 2016; Vol 26(9): 1156–1166 [DOI: 10.1089/thy.2015.0567]
Objective:
To provide an evidence-based review on the frequency, clinical implications, and management strategies of invasive differentiated thyroid cancer (DTC) involving adjacent structures of the neck.
Key Findings:
Frequency of Invasion(based on pooled data and institutional experience):
Recurrent Laryngeal Nerve (RLN): ~ 47% of locally advanced cases
Strap Muscles: ~ 40%
Trachea: ~ 21%
Esophagus: ~ 12%
Larynx: ~ 3%
Carotid Artery: ~ 2%
RLN and strap muscle invasion were:
The most common sites of local extension.
Surgical Management Recommendations:
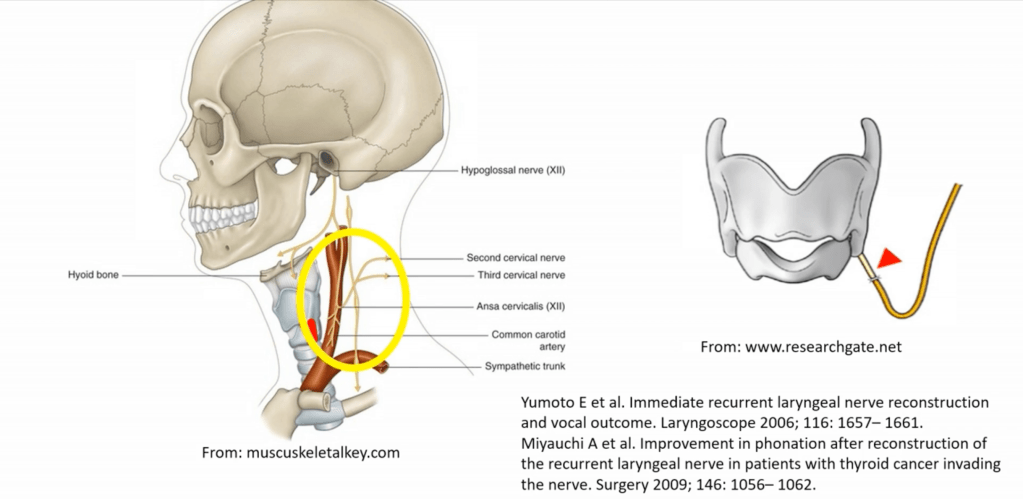
Recurrent Laryngeal Nerve (RLN):
If functional and partially encased:
Consider nerve preservation via shaving
If non-functional or fully invaded:
Resection is advised with or without reinnervation techniques
Postoperative vocal cord assessment is mandatory
American Head and Neck Society (AHNS) Consensus Statement:
Tumor may be shaved off so that the RLN is spared (consensus)
Reference:
Shindo ML et al. Management of invasive well-differentiated thyroid cancer: An American Head and Neck Society Consensus Statement: AHNS Consensus Statement. Head Neck 2014 36: 1379-1390.
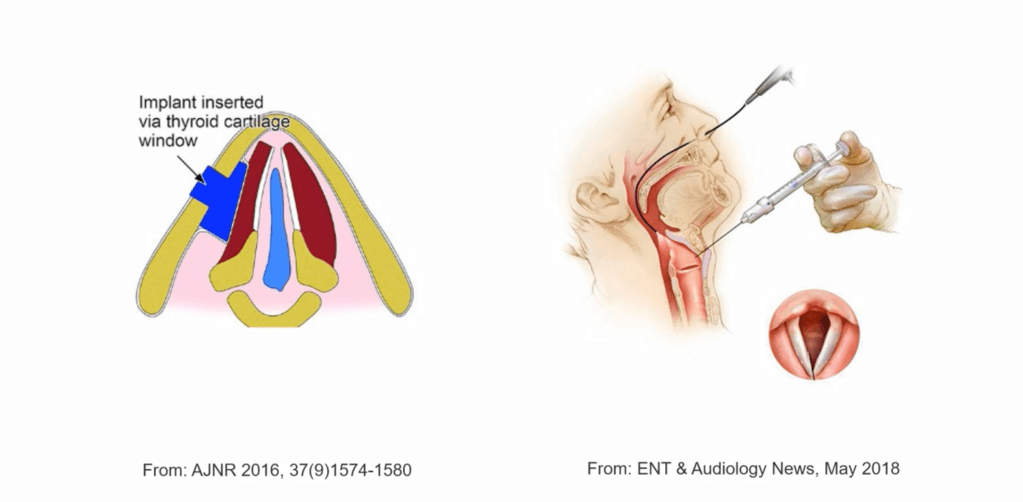
If the nerve is sacrified RLN reconstruction is advisable or thyroplasty or cord injection.
Surgical Management Recommendations:
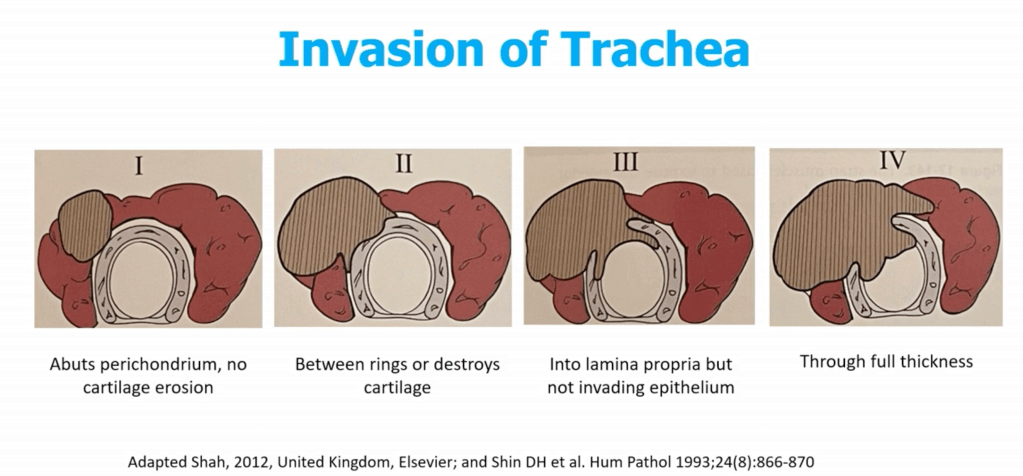
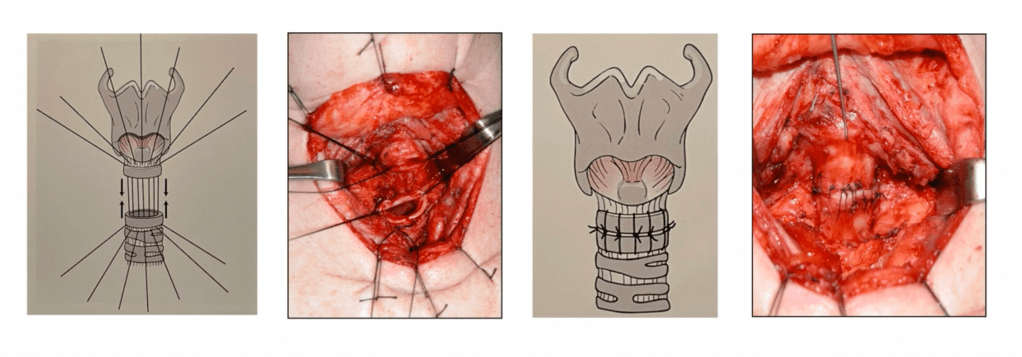
Trachea:
Shaving of superficial invasion is acceptable
Full-thickness invasion may require window or segmental resection (e.g., tracheal reconstruction):
Multi-disciplinary planning often needed
Main methods of management:
Shave:
Used when tumor invades perichondrium or cartilage only:
Tangential excision with minimal invasion leaving mucosa intact
Preserves tracheal framework
Disadvantages:
Confirming negative margins intraoperatively
Lack of continuous plane underneath the external perichondrium
Tumor spread into the tracheal lumen via lymphatics that communicate in the intercartilaginous space
Local control:
Around 95% if tumor does not penetrate beyond the perichondrium
Window Resection:
Limited by the length and circumference of the trachea to mantain stability:
Need to resect < 1/3 of the circumference
Partial resection of < 3 rings
Often for McCaffrey Stage II to III
Primary closure rarely possible
Needs to be reconstructed with muscle flap or patch graft
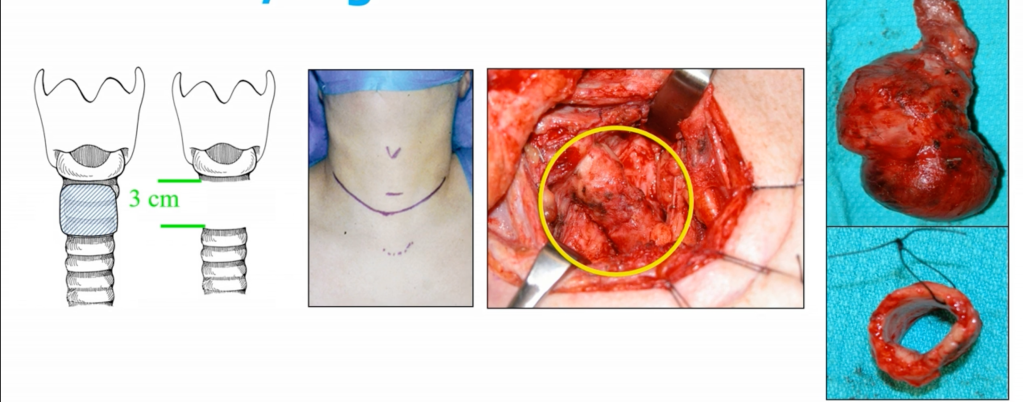
Sleeve / Segmental Resection:
En bloc removal of ≥ 2 tracheal rings:
Up to 5 cm to 6 cm or 5 to 7 rings
End-to-end primary anastomosis under neck flexion
May include cricotracheal or laryngotracheal resection if involvement is proximal
Technical Considerations:
Maximum safe length for tension-free anastomosis: ~4.5 to 6 cm (5 to 7 rings)
Requires preoperative anesthesia planning for airway control
Neck flexion with chin-to-chest sutures post-op
Close monitoring for anastomotic dehiscence, tracheomalacia, or RLN injury
Outcomes:
5-year disease-specific survival:
~ 60% to 75% after R0 sleeve resection
Morbidity:
Risk of vocal cord paralysis, anastomotic leak, or stenosis
Local control better with segmental vs shave resection in deeply invasive tumors
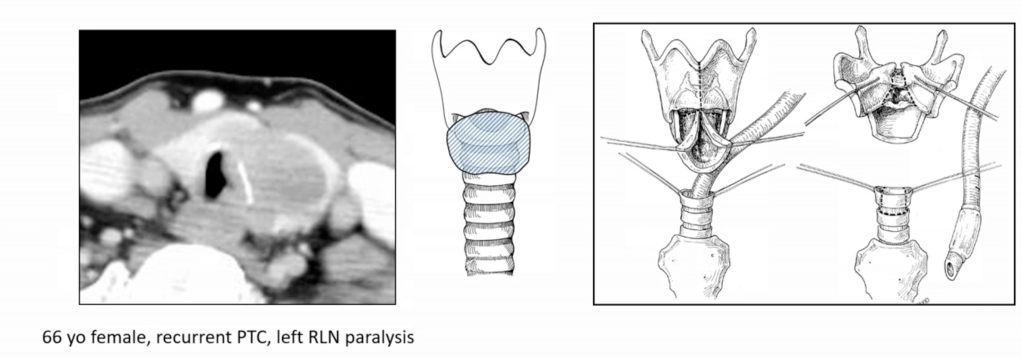
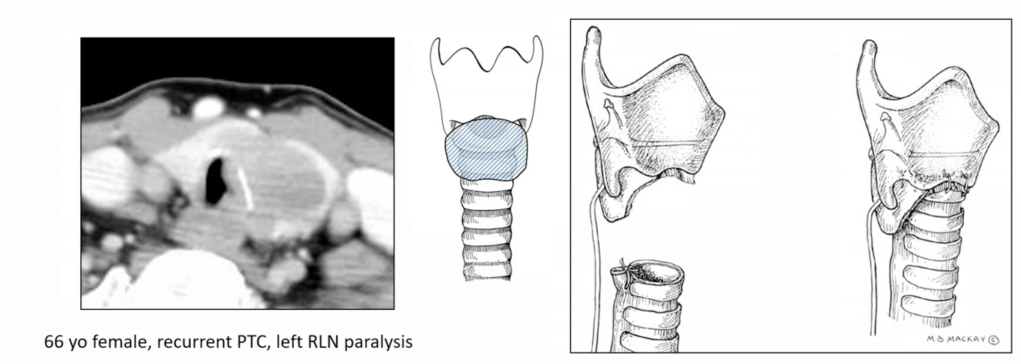
Cricotracheal Resection
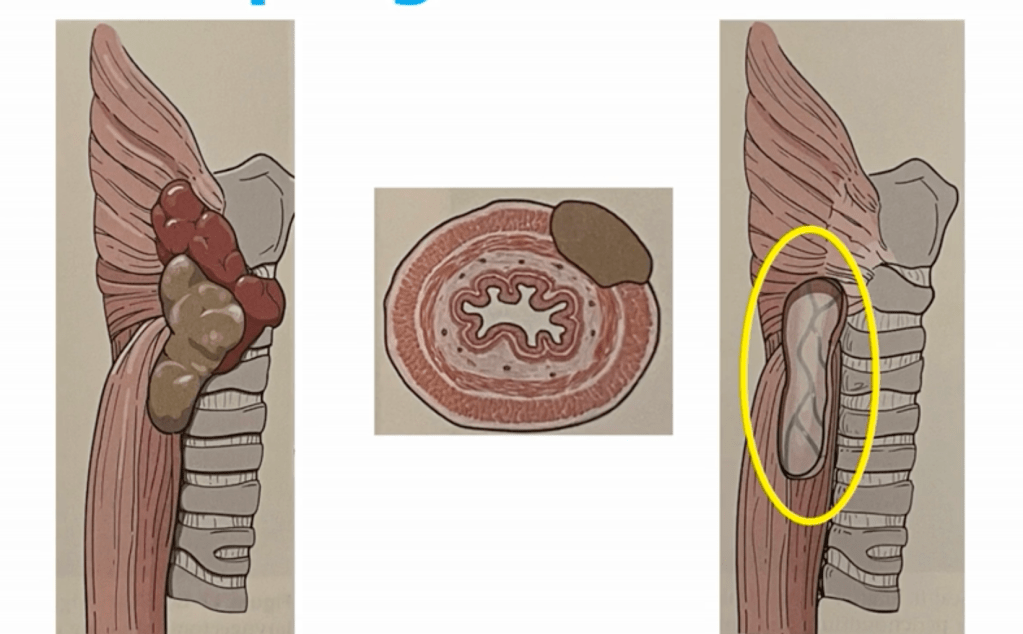
Esophagus:
Esophageal invasion occurs in approximately 5% to 15% of patients with locally advanced differentiated thyroid cancer (DTC) or poorly differentiated thyroid cancer:
Particularly with posterior capsular extension from the thyroid gland:
It is most often associated with invasion of the cervical esophagus and less frequently with thoracic extension
Assessment and Staging:
Preoperative Workup:
CT scan with contrast:
Assess loss of fat plane and wall thickening
Endoscopic ultrasound (EUS) or esophagoscopy:
Assess mucosal involvement
Barium swallow:
Functional and structural assessment
Flexible laryngoscopy:
Assess vocal cord function
McCaffrey Staging System (modified for posterior invasion):
Stage I to II:
Abutment or superficial muscular invasion
Stage III:
Transmural involvement with mucosal breach
Stage IV:
Extensive circumferential or thoracic invasion
Surgical Management:
Shave Excision:
For superficial invasion of muscularis layer only:
Avoids full-thickness resection
Low morbidity, but risk of residual disease if not adequately evaluated
Partial Thickness Resection:
Involves resection of outer muscular layer with cautery or cold dissection
For example radial forearm, pectoralis major, or free jejunal flap
May require temporary nasogastric / PEG feeding or tracheostomy
Cervical Esophagectomy with Reconstruction:
Rare; indicated in extensive disease
High morbidity, reserved for selected cases with curative intent
Postoperative Considerations:
Leak test (methylene blue or contrast swallow) on POD 5 to 7 if full-thickness resection
Monitor for:
Dysphagia
Fistula
Stricture formation
Consider gastrostomy or jejunostomy in high-risk cases
Adjuvant Therapy:
Radioactive Iodine (RAI):
If iodine-avid disease and residual / recurrent disease
External Beam Radiation (EBRT)::
Gross residual disease
Positive margins
Non-RAI-avid disease
Prognosis:
Complete resection (R0) improves local control and survival
Positive margins or incomplete resection associated with:
Higher recurrence rates
Lower disease-specific survival
Five-year survival can still exceed 60% to 70% with aggressive, multidisciplinary management
Key References:
McCaffrey TV.Surgical management of invasion into the aerodigestive tract by well-differentiated thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 1999;125(4):401–405.
Shaha AR.Airway and esophageal involvement in thyroid cancer. World J Surg. 2007;31(5):904–911.
Nixon IJ et al.Locally advanced thyroid cancer: Surgical management. Thyroid. 2016;26(9):1156–1166.
Gaissert HA et al.Surgical treatment of invasive thyroid cancer. Ann Thorac Surg. 2007;83(6):1950–1955.
Haugen BR et al.ATA Guidelines. Thyroid. 2016;26(1):1–133.
Kim JW et al.Optimal surgical approach to locally invasive DTC. J Surg Oncol. 2017;116(2):229–234.
McCaffrey TV.Surgical management of laryngotracheal invasion by well-differentiated thyroid cancer. Arch Otolaryngol Head Neck Surg. 1999;125(4):401–405.
Gaissert HA et al.Segmental tracheal resection for invasive thyroid carcinoma. Ann Thorac Surg. 2007;83(6):1950–1955.
Kim JW et al.Optimal surgical extent for locally invasive thyroid cancer. J Surg Oncol. 2017;116(2):229–234.
Shaha AR.Airway management in thyroid cancer. World J Surg. 2007;31(5): 903–908.
Strap Muscles:
Often resected without morbidity
Invasion here does not necessarily confer worse prognosis
The strap muscles (sternohyoid, sternothyroid, omohyoid, thyrohyoid):
Lie anterior and lateral to the thyroid gland and are often the first structures invaded in locally advanced disease
Seen in up to 40% to 50% of cases with extrathyroidal extension (ETE):
Classified by AJCC 8th edition as:
Minimal ETE:
Invasion into perithyroidal soft tissue:
Not included in T staging
Gross ETE to strap muscles:
T3b disease
According to Nixon IJ et al., strap muscle is the most frequently invaded adjacent structure in locally advanced DTC
Diagnosis:
Clinical and Imaging Features:
May present as firm fixation of the gland to strap muscles
On ultrasound CT:
Loss of fat plane
Muscle effacement
Intraoperative findings often determine true invasion
Surgical Management:
Recommended Approach:
En bloc resection of involved strap muscles with the thyroid gland
Usually limited to sternohyoid and sternothyroid
No need for reconstruction unless deep muscle loss impairs swallowing or airway support
Not Recommended:
Piecemeal shaving or curettage:
May lead to positive margins
Avoid unnecessarily wide resections if invasion is not gross
Pathologic confirmation of muscle invasion is essential for staging (T3b)
Oncologic Impact:
Survival & Recurrence:
Strap muscle invasion alone does not significantly affect disease-specific survival
Prognosis more dependent on:
Nodal status
Margin status
Multifocality or vascular invasion
Kim et al., J Surg Oncol 2017 – strap muscle invasion was not an independent predictor of recurrence or mortality
Adjuvant Therapy:
RAI therapy based on full risk stratification (not just muscle invasion)
No EBRT indicated for strap-only invasion with negative margins
ATA 2015 Guidelines:
Strap invasion alone may not upstage to high-risk unless other features are present
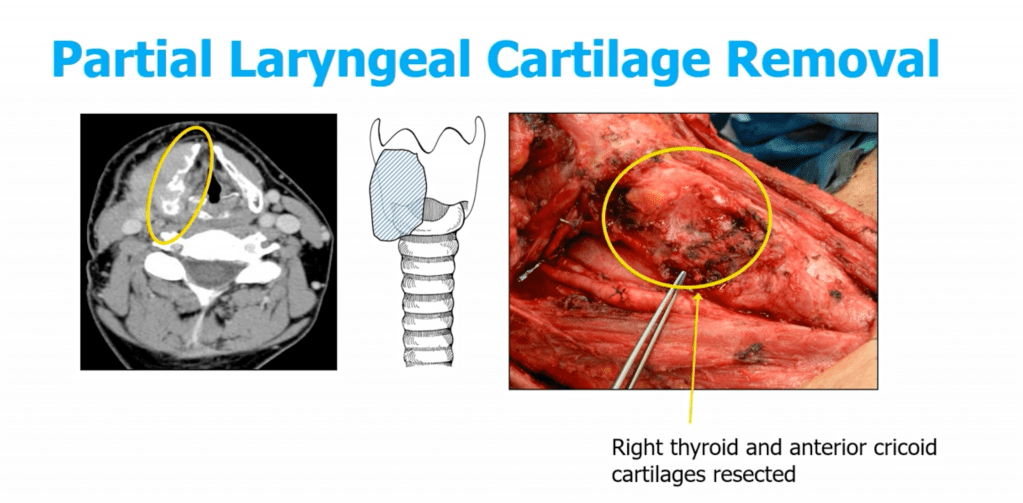
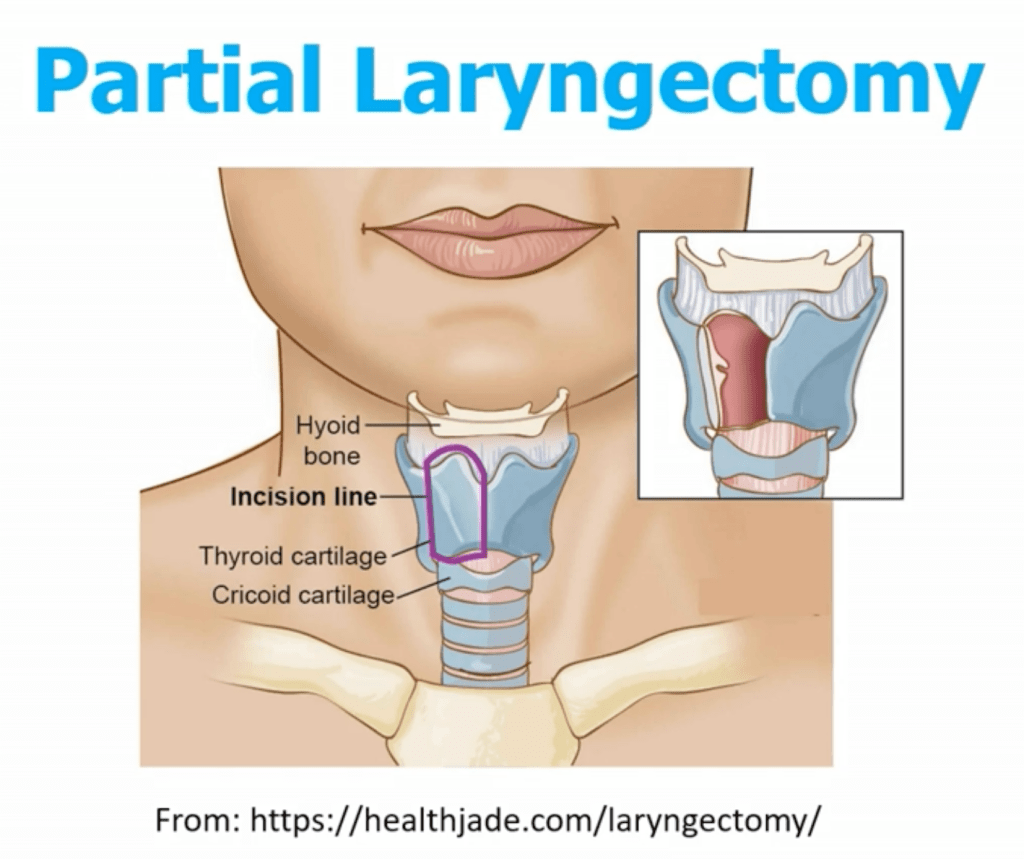
Larynx and Carotid Artery:
Invasion is rare but serious
Laryngectomy or carotid resection is only considered in select patients with curative intent
Prognosis and Outcomes:
Gross extrathyroidal extension (T4 disease) is associated with worse disease-specific survival
However, microscopic invasion alone does not significantly impact survival
Complete surgical resection remains the most important prognostic factor
Conclusions:
Adjacent structure invasion is relatively common in advanced DTC, especially involving the RLN and strap muscles
Tailored surgical approaches balancing oncologic control and functional preservation are critical
Multidisciplinary care and evidence-guided surgical decision-making optimize outcomes.
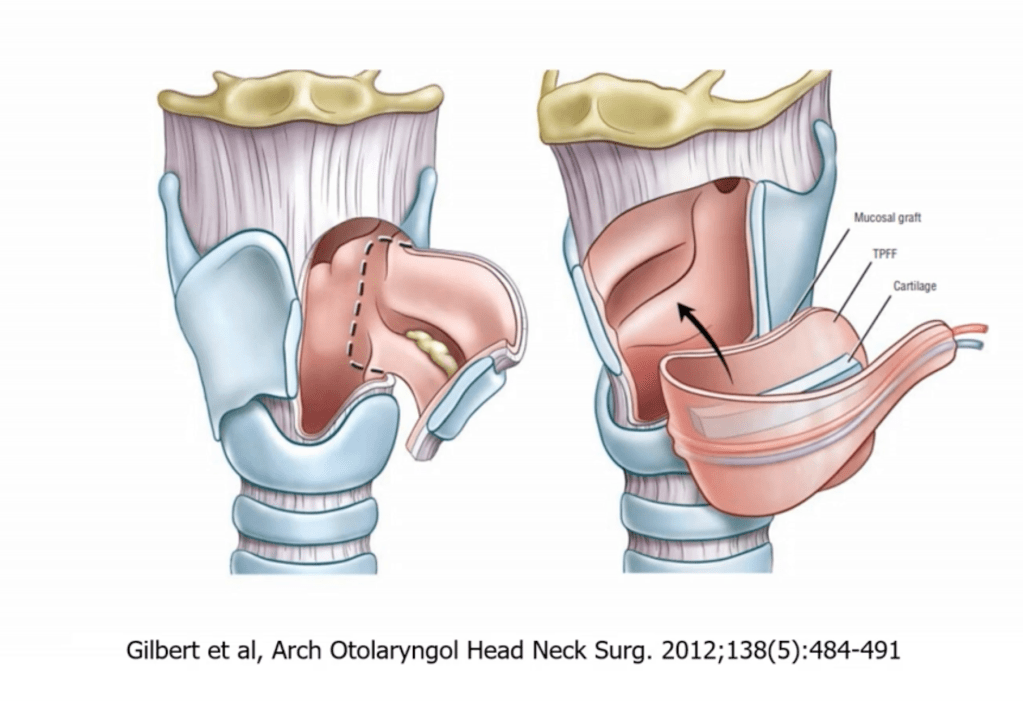
McCaffrey ClassificationWindow Resection of the TracheaSleeve / Segemental ResectionWe use #3-0 Vicryl to bring the segments together. We perform this in conjunction with thoracic surgery.Cricotracheal ResectionCricotracheal ResectionTemporoparietal free flap (TPFF) with buccal mucosa inner graft with thryoid cartilage as a construct. Esphageal Invasion
Conclusion:
Surgery is the KEY component for survival in patients with poorly differentiated / invasive thyroid cancer
The incidence of PHPT has remained relatively stable in the last couple of decades
PHPT is more common in women than in men:
Two to three times higher in incidence rate in women
PHPT is more common in the elderly population:
The incidence increases with age
The incidence starts to increase at age 50:
1 in 500 postmenopausal women will have PHPT
1 in 1000 men over 50 will have PHPT
Incidence rates in the USA:
60 cases per 100, 000 women
20 cases per 100,000 men
Prevalence
In the USA:
1% of the postmenopausal female population will have PHPT
International prevalence rates:
3% of the postmenopausal female population will have PHPT
The prevalence PHPT has risen in the last couple of decades:
From 1995 and 2010 it has tripled:
Women:
76 to 233 cases per 100,000 women
Men:
30 to 85 cases per 100,000 men
Gender:
African Americans have the highest prevalence of PHPT:
Followed by caucasians followed by Asians
Hispanics have a lower prevalence rate
Reason for the higher prevalence compared to incidence in PHPT:
Is that only 20% to 25% of patients with PHPT in the USA will end up having surgery
Only 50% of patients in the USA with nephrolithiasis and PHPT have surgery
Only 20% of patients with osteoporosis and PHPT in the USA go onto have surgery
The probability of having surgery decreases with age:
The older one gets the less likely they will be offered an intervention
Genetics of PHPT:
Six primary conditions associated with an inherited predisposition for the development of PHPT:
MEN Type 1:
Incidence:
The incidence of PHPT has remained relatively stable in the last couple of decades
PHPT is more common in women than in men:
Two to three times higher in incidence rate in women
PHPT is more common in the elderly population:
The incidence increases with age
The incidence starts to increase at age 50:
1 in 500 postmenopausal women will have PHPT
1 in 1000 men over 50 will have PHPT
Incidence rates in the USA:
60 cases per 100, 000 women
20 cases per 100,000 men
Prevalence
In the USA:
1% of the postmenopausal female population will have PHPT
International prevalence rates:
3% of the postmenopausal female population will have PHPT
The prevalence PHPT has risen in the last couple of decades:
From 1995 and 2010 it has tripled:
Women:
76 to 233 cases per 100,000 women
Men:
30 to 85 cases per 100,000 men
Gender:
African Americans have the highest prevalence of PHPT:
Followed by caucasians followed by Asians
Hispanics have a lower prevalence rate
Reason for the higher prevalence compared to incidence in PHPT:
Is that only 20% to 25% of patients with PHPT in the USA will end up having surgery
Only 50% of patients in the USA with nephrolithiasis and PHPT have surgery
Only 20% of patients with osteoporosis and PHPT in the USA go onto have surgery
The probability of having surgery decreases with age:
The older one gets the less likely they will be offered an intervention
Genetics of PHPT:
Only 5% to 10% of patients with PHPT will with have an underlying genetic predisposition
Six primary conditions associated with an inherited predisposition for the development of PHPT:
MEN Type 1:
Pituitary Tumors
PHPT:
Has almost 100% penetrance
It is the first endocrine disease to manifest
It manifests at a young age
Pancreatic neuroendocrine tumors:
Duodenal and gastronomes
Foregut carcinoid tumors:
Lung
Thymus
Adrenal adenomas
MEN Type 2A:
Medullary thyroid carcinoma:
100% penetrance
First endocrinopathy to manifest
Pheochromocytoma
PHPT:
Only 20% to 30% develop PHPT
Will depend on the RET mutation (codon)
They develop mild hypercalcemia
More common to see multi gland disease but you can also get one gland disease
Age of onset is younger:
Two decades earlier than sporadic PTHP
MEN Type IV:
Phenotypically similar to MEN type 1
Mutation CDKNIB gene
Hyperparathyroidism jaw tumor syndrome (rare):
Ossifying fibromas
Mixture of renal tumors, uterine fibroids
Familial hypocalciuric hypercalcemia (FHH – predisposes to hypercalcemia):
FHH is mainly classified into three different types depending on the genetic cause
FHH type 1:
Is the most common type of FHH and is caused by changes (also known as pathogenic variants or mutations) in the CASR gene
The protein made from the CaSR gene:
The calcium-sensing receptor (CaSR protein), monitors and regulates the level of calcium in the blood
FHH type 2:
Is caused by changes in the GNA11 gene
FHH type 3:
Is caused by changes in the AP2S1 gene
All three types of FHH are inherited in:
An autosomal dominant manner
In rare cases, FHH may be caused when a person’s immune system mistakenly makes antibodies that attack the CaSR protein:
The autoimmune form of FHH is not known to be caused by changes in a specific gene
Diagnosis of FHH:
Is suspected by high levels of calcium in the blood:
Especially when there are no other symptoms present
Further blood and urine tests may be used to rule out other possible causes
Genetic testing can confirm the diagnosis of FHH, except in rare autoimmune cases
Treatment:
Is typically considered unnecessary because most people with FHH do not have symptoms
If pancreatitis occurs, removal of the parathyroid gland may be recommended
Isolated familial PHPT
Management of inherited PHPT:
In many cases PHPT is the first manifestation of a hereditary syndromic disease:
Goal of surgery is to normalize PTH and provide best chances for long term disease free outcome
Pitfalls in imaging in patients with MEN type 1:
Present with parathyroid gland asymmetry:
Most of this cases are secondary to hyperplasia not adenoma
The gold standard for the management of MEN type 1 is:
Bilateral neck exploration with a subtotal parathyroidectomy or total parathyoidectomy with autotransplantation (to the sternocleidomastoid muscle of the neck or the brachioradialis muscle of the forearm):
Biochemical cure are very similar between both approaches
With autotransplantation there is a 3% to 10% risk that the autotransplanted gland does not take leading to hypoparathyroidism:
For this reason cryopreservation might be a good option (they can be kept in this state for up to 2 years)
Remember that 3% to 5% of the cases of MEN type 1 might have super numerary glands:
This glands might hide in the thymus / thryothymic ligament or other ectopic locations
Intraoperative PTH measuring:
Allows us to decide how much of a gland remnant can be left behind to achieve longterm cure:
Achieving a intact PTH less that 40 pg/dl supports a longer long term free of recurrence
If the intraoperative PTH is very low it can helps us decide to autotransplant a gland to decrease that incidence of postoperative permanent hypoparathyroidism
Management of MEN type IIa:
All of this patients will have manifested with medullary thyroid cancer (MTC) or will be diagnosed with MTC and PHPT at the same time
The operative report of the thyroid cancer case is required along with the pathology report:
Talking with the surgeon that performed the thyroidectomy will be beneficial
At least two localizing studies that are concordant
Use cryopreservation in re due cases:
Because we might not have the information of how many glands were removed or injured during the thyroid surgery
Autotransplantation might be a good option when managing PHPT because MTC commonly recurs in the neck
If operating for the MTC and PHPT at the same time:
The surgery for PHPT remove the abnormal gland check intraoperative PTH (make sure it is normal) and leave the rest of the normal glands in situ
If subtotal thyroidectomy is performed:
Leave a portion of a gland that is about the same size as a normal gland
Make sure it is well vascularized
If possible leave an inferior gland:
They are easier to localize than a superior gland in re due cases
Prevents deep dissection close to the RLN in re due cases