Neurokinin-1 (NK1) receptor antagonist and a 5-Hydroxytryptamine-3 (5-HT3) receptor antagonist + Dexamethasone with aggressive IV hydration and Mg / K supplementation
Why:
Cisplatin is highly emetogenic:
Triple prophylaxis is standard
Hydration / Mg reduce nephrotoxicity
Pitfalls:
Under-treating weekly dose (still emetogenic)
Missing Mg monitoring
Refs: ASCO / ESMO CINV guidelines; supportive care standards
The editorial conclusion remains that cetuximab-RT is the standard comparator in the cisplatin-ineligible populationThe Lancet
Bottom line:
In a cisplatin-ineligible patient:
Cetuximab-RT is a guideline-accepted radiosensitizing regimen with randomized evidence vs RT alone and remains the standard control in contemporary trials of the ineligible population The Lancet
Why you should not swap cisplatin to cetuximab in an eligible (especially in HPV+) patient:
Two large, definitive, head-to-head trials in HPV-positive oropharyngeal cancer:
RTOG 1016 (Gillison et al., 2019):
RT + cetuximabfailed non-inferiority to RT + cisplatin for:
Overall survival:
OS HR 1.45, one-sided 95% upper CI 1.94
5-yr OS:
77.9% (cetuximab) vs 84.6% (cisplatin)
No clinically meaningful reduction in overall serious toxicity with cetuximab
Conclusion:
Cisplatin-RT is superior:
Do not substitute cetuximab for convenience PubMed
De-ESCALaTE HPV (Mehanna et al., 2019):
2-yr OS: 97.5% with cisplatin vs 89.4% with cetuximab
PFS and recurrence outcomes also favored cisplatin
Main Classes of Active Cytotoxic Chemotherapeutic Agents for Head and Neck Squamous Cell Carcino
After patients with recurrent and / or metastatic squamous cell carcinoma (SCC) of the head and neck have exhausted the options of surgery and / or radiation:
The likelihood of cure diminishes substantially:
With a median survival historically being:
Less than 1 year
In this group, systemic therapy administered with palliative intent is the treatment of choice:
Single agent therapy can produce objective responses in:
10% to 30% of patients
Single agents that typically are used in this setting include:
Cisplatin
Taxanes
Methotrexate
5-FU
Cetuximab
Vinorelbine, bleomycin, ifosfamide, and pemetrexed:
Also have shown clinical activity against advanced head and neck cancers
The durability of response to chemotherapy alone:
Generally is measured in:
Weeks to months, not years
An early, randomized trial reported by Morton:
Provided evidence that cisplatin treatment prolonged survival:
By approximately 10 weeks in patients with advanced head and neck cancer:
Compared with best supportive care
There are no striking efficacy differences:
Among cytotoxic chemotherapy agents in the recurrent disease setting:
Hong and colleagues:
Compared cisplatin versus methotrexate as palliative therapy for 44 patients with head and neck cancer that had recurred after surgery and / or radiation
Patients had not received prior chemotherapy
The median survival was approximately 6 months in both arms:
Although methotrexate seemed to be somewhat better tolerated
Similarly, in a randomized study of 100 patients with advanced inoperable head and neck cancer:
That compared cisplatin versus methotrexate:
Grose and colleagues:
Did not detect any significant differences in survival between the two treatment groups
Taxanes:
Yielded encouraging response rates as:
First-line therapy for patients with recurrent disease
Forastiere’s group:
Observed a response rate of 40% among 34 patients treated with paclitaxel
Dreyfuss and colleagues:
Reported a response rate of 42% among 31 patients treated with docetaxel
In a randomized phase II trial that compared docetaxel versus methotrexate among 57 patients with advanced head and neck cancer:
No difference in overall survival was found between the two groups:
Although the response rate was significantly better for the docetaxel group:
27% versus 15%
Combination chemotherapy regimens:
Appear to be associated with:
Increased response rates and often with increased toxicities:
But generally not with increased survival
In 1985 Vogl reported the results of a prospective study:
In which 163 patients were randomly assigned to receive:
Methotrexate monotherapy or methotrexate plus bleomycin plus cisplatin
Objective responses were more frequent in the combination chemotherapy group:
But median survival was 5.6 months in each group
A three-arm randomized study of 249 patients with advanced head and neck cancer that was reported by Jacobs and colleagues:
Compared the cisplatin plus 5-FU doublet versus cisplatin monotherapy versus 5-FU monotherapy
The objective response rate and hematologic toxicities were highest with the doublet regimen:
But median survival was approximately 5.7 months for all groups
Taken together, these studies suggest that:
Combination chemotherapy regimens may be appropriate for patients with good performance status:
If objective tumor response is believed to be necessary for palliation of advanced head and neck cancer
No combination chemotherapy regimen appears to be superior to another in terms of survival for patients with advanced head and neck cancer:
A Southwest Oncology Group study reported by Forastiere randomly assigned 277 patients with advanced head and neck cancer to:
Treatment with cisplatin plus 5-FU, carboplatin plus 5-FU, or methotrexate monotherapy
In the comparison of the doublet regimens:
Cisplatin plus 5-FU yielded a higher response rate than did carboplatin plus 5-FU:
32% versus 21%, p = .05
However, median survival times were similar in all three treatment groups in the study
Gibson reported a randomized comparison of cisplatin plus 5-FU (CF) versus cisplatin plus paclitaxel (CP) for 218 patients with advanced head and neck cancer:
The response rate:
27% in the CF group and 26% in the CP group
Median survival:
8.7 months in the CF group and 8.1 months in the CP group
The overall results did not differ significantly
These studies highlight the inherent limitations of cytotoxic chemotherapy in the recurrent or metastatic disease setting and set the stage for the development of novel molecularly targeted therapeutic agents for head and neck cancer
Cetuximab represents the first biologic agent to enter routine clinical practice as a palliative agent for patients with advanced head and neck cancer:
In a phase II study of 103 patients with recurrent and / or metastatic head and neck cancer:
With documented disease progression within 30 days after a minimum of two and a maximum of six platinum-based chemotherapy treatments:
Vermorken reported that the:
Response rate was 13% and the median time to progression was 70 days
Treatment was generally well tolerated:
The most common adverse event was a rash
Cetuximab can also be combined with other cytotoxic chemotherapeutic agents to achieve therapeutic advantage for some patients with advanced HNSCC:
In a phase III study by Burtness for patients with recurrent or metastatic disease who had not received any prior palliative chemotherapy:
117 subjects were randomly assigned to receive cisplatin plus cetuximab versus cisplatin plus placebo
The objective response rate was higher for cisplatin plus cetuximab:
26% versus 10%, p = .03:
But no significant difference in survival was found between the two groups
The investigators noted that in the cetuximab plus cisplatin group:
Objective responses were more frequent in patients who experienced skin toxicity:
Although the number of subjects was too small to establish a statistically significant correlation between dermatologic toxicity and response
The EXTREME trial:
Randomized 442 patients with untreated recurrent or metastatic head and neck cancer to platinum (cisplatin or carboplatin) plus infusional 5-FU alone for a maximum of 6 cycles with or without cetuximab
Patients randomized to the experimental arm (with cetuximab) with at least stable disease:
Were continued on cetuximab alone after combination therapy
Results:
Objective response rate:
20% versus 36%, p < .001
Progression-free survival:
3.3 months versus 5.6 months p < .001
Overall survival:
7.4 months versus 10.1 months, p = .04
All favored the experimental group
The lack of crossover in the study design leaves open the question of whether similar improvements in overall survival could be achieved with sequential treatment with the platinum doublet followed by cetuximab, or vice versa:
However, the study does further establish the platinum / 5-FU plus cetuximab as a standard first-line palliative option for patients with advanced head and neck cancer.
One of the most exciting areas of progress for head and neck cancer research is the emergence of immunotherapeutic approaches for this disease:
Led by the integration of therapeutic antibodies targeting the T cell immune checkpoint PD-1 (programmed death 1) into clinical practice (Figure)
The activity observed with these drugs established the critical proof of principle that the immune system can be pharmacologically harnessed to produce clinically significant responses in head and neck cancer patients
PD1 and PDL1 pathway in tumor immune microenvironment.
CHECKMATE-141 was a randomized phase III clinical trial:
Comparing the efficacy of nivolumab:
A monoclonal antibody directed against PD-1;
To investigator’s choice chemotherapy (methotrexate, docetaxel, or cetuximab) in recurrent / metastatic patients with tumor progression or recurrence:
Within 6 months after the last dose of platinum containing chemotherapy (Ferris et al., 2016)
The trial demonstrated a survival benefit with nivolumab over chemotherapy:
With a median overall survival of 7.5 months versus 5.1 months and a 1-year overall survival of 36% versus 16.6%, respectively.
The response rate with nivolumab was 13.3% versus 5.8% with chemotherapy
KEYNOTE-012 was a multicohort phase 1b trial:
Evaluating the efficacy of another PD-1–directed antibody pembrolizumab in a variety of different malignancies, including recurrent / metastatic head and neck cancer
Among 60 head and neck cancer patients whose tumors expressed PD-L1 (the ligand for PD-1):
Pembrolizumab elicited an 18% response rate and a median overall survival of 13 months (in an intent to treat analysis) (Seiwert et al., 2016)
Another expansion cohort in KEYNOTE-012 enrolled 132 recurrent / metastatic head and neck cancer patients regardless of PD-L1 status:
Reporting an 18% response rate and median overall survival of 8 months (Chow et al., 2016)
While KEYNOTE-012–enrolled patients who had received any number of lines of prior chemotherapy for recurrent / metastatic disease (including treatment-naïve patients):
KEYNOTE-055 was a single-arm phase II trial designed to evaluate pembrolizumab in patients who experienced progression of disease within 6 months of platinum and cetuximab therapy (Bauml et al., 2017):
The reported response rate was 16% with a median overall survival of 8 months
Both nivolumab and pembrolizumab have been FDA-approved for the treatment of recurrent / metastatic head and neck cancer patients with disease progression on or after progression with platinum-containing chemotherapy:
Establishing a new standard for second-line treatment
After the approval of pembrolizumab in this setting, the results of a randomized, open-label phase III trial comparing the efficacy of pembrolizumab to investigator’s choice chemotherapy (methotrexate, docetaxel, or cetuximab) in platinum refractory recurrent / metastatic patients, or locally advanced disease patients with recurrence or progression within 3 to 6 months of definitive platinum-based therapy:
Were reported (KEYNOTE 040; Cohen et al., 2018):
For the primary endpoint of overall survival, pembrolizumab was superior compared to standard therapies, but the degree of benefit (hazard ratio [HR] for death 0.80 [95% CI 0.65-0.98; one-sided p = 0.0161] failed to meet the goals pre-specified for the study [HR of 0.70 or better with one-sided a of 0.025]:
The authors speculated that the 13% of standard arm patients who received immune checkpoint inhibitor therapy after trial completion could have confounded this survival analysis
Still, most agree that the observed improvements in survival with pembrolizumab, as well as its superior safety profile compared to standard chemotherapies, justifies its use in this setting
More broadly speaking, the smaller margins of benefit observed for nivolumab or pembrolizumab compared to chemotherapy in unselected head and neck cancer patient populations:
Argues for the need to develop predictive biomarkers that will allow identification of those who are most likely to benefit from PD-1 / PD-L1 pathway targeting
In many scenarios, single-modality radiation therapy:
Is a historical standard intervention after primary surgery for stages III and IV head and neck cancer
Intergroup study 0034 (RTOG 8503):
Which randomly assigned patients with resected head and neck squamous cell carcinoma to receive:
Postoperative radiation therapy alone or postoperative cisplatin (100 mg/m2 once every 3 weeks) plus 5-FU (1000 mg/m2/day in a continuous infusion for 120 hours every 3 weeks) followed by radiotherapy:
Failed to show significant differences in outcomes between the two treatment groups
A retrospective analysis did identify subsets of patients with high-risk features on surgical pathology:
The study suggested that clinical studies of postoperative concurrent chemoradiation should be conducted for patients with high-risk disease
Bachaud and colleagues conducted a randomized trial for patients who had undergone primary surgery for head and neck cancer and had high-risk disease:
Defined as extracapsular spread of malignancy in resected lymph nodes (Figure)
Eighty-three patients were randomly assigned to receive postoperative radiotherapy alone or postoperative radiotherapy with concurrent cisplatin (50 mg administered intravenously once a week in a flat dose):
Overall survival and disease-free survival were significantly better:
In the combined modality group:
OS: 36% vs 13% (p < 0.01)
DFS: 45% vs 23% (p < 0.01)
The improvement in the locoregional control rate approached statistical significance in favor of the combined modality group:
77% vs 59% (p = 0.08)
Design and results of a trial of postoperative concurrent chemoradiation for locally advanced head and neck carcinoma. (Adapted from Bachaud JM, Cohen-Jonathan E, Alzieu C, et al. Combined postoperative radiotherapy and weekly cisplatin infusion for locally advanced head and neck carcinoma: final report of a randomized trial. Int J Radiat Oncol Biol Phys 1996;36:999–1004.)
Cisplatin plus radiotherapy in the postoperative setting was evaluated in the:
EORTC 22931 and RTOG 95–01 randomized clinical trials (Figure)
Design and results of European Organization for Research and Treatment of Cancer trial 22931. HNSCC, Head and neck squamous cell carcinoma. (Adapted from Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004;350:1945–1952.)Design and results of Radiation Therapy Oncology Group trial 95–01. HNSCC, Head and neck squamous cell carcinoma. (Adapted from Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004;350:1937–1944.)
Both studies were limited to patients who had high-risk features in the surgical pathology:
Although the studies differed slightly in the high-risk features that were used for eligibility:
In EORTC 22931:
High risk was defined as:
Positive or close surgical margins (≤ 5 mm)
Extra-capsular extension of nodal disease
Involvement of lymph nodes at level IV or V:
From oral cavity or oropharynx primary sites
Perineural disease
Vascular embolism
RTOG 95–01 defined high risk as:
Positive surgical margins
Extracapsular extension
Involvement of two or more lymph nodes
In both studies:
Patients were randomly assigned to radiation alone or radiation plus concurrent cisplatin (100 mg/m2 on days 1, 22, and 43)
The estimated 5-year overall survival:
From the EORTC 22931 trial was:
53% in the combined modality group and 40% in the radiotherapy group (p < .05)
In the EORTC 22931 trial:
Progression-free survival and locoregional control:
Also were significantly improved in the combined modality group:
Improved 5-year progression-free survival:
47% vs. 36%, p < 0.05
Lower incidence of local region relapse at 5 years:
18% vs. 31%, p < 0.05
With a median follow-up of 45.9 months, RTOG 95–01:
Demonstrated significant improvements in locoregional control and disease-free survival for the cisplatin plus radiation group:
Improved 2-year locoregional control rate:
82% vs. 72%, p < 0.05
Improved disease free survival:
Hazard ratio 0.78, p < 0.05
But the improvement in overall survival for this group did not reach statistical significance:
Hazard ratio 0.84, p 0.19
Bernier and colleagues performed a pooled analysis to compare eligibility criteria and outcomes in the two trials:
When the analysis was restricted to patients with high-risk disease according to criteria that were used in both studies (positive surgical margin and / or extracapsular extension):
A significant improvement in overall survival:
Was seen for the group of patients that received concurrent cisplatin and radiation therapy (Figure)
As such, postoperative radiation plus concurrent administration of high-dose cisplatin:
Is a widely accepted standard of care for fit patients with either of these high-risk features on surgical pathology
Impact of adjuvant chemoradiation on survival in the presence of extracapsular extension and/or positive surgical margins in the European Organization for Research and Treatment of Cancer 22931 and Radiation Therapy Oncology Group trials 95-01. RCT, Radiochemotherapy; RT, radiotherapy. (Adapted from Bernier J, Cooper JS, Pajak TF, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of EORTC (#22931) and RTOG (#9501). #Arrangoiz #CancerSurgeon #HeadandNeckSurgeon #SurgicalOncologist #MountSinaiMedicalCenter #MSMC #Miami #Mexico #ChemoradiationTherapy
Primary treatment with concurrent chemotherapy and radiation therapy has been accepted widely as a standard of care:
Since the publication of the Meta-Analysis of Chemotherapy on Head and Neck Cancer in 2000:
This meta-analysis was later updated in 2009:
Involving an analysis of 50 trials:
That showed an absolute survival benefit of 6.5% at 5 years:
Associated with administering chemotherapy concurrently with radiation
Bolus cisplatin (100 mg/m2 on days 1, 22, and 43) concurrent with radiation therapy:
Has been extensively studied:
May be considered the standard to which other chemotherapy regimens are compared in clinical research
The intergroup trial conducted by Adelstein and colleagues was influential in establishing this regimen (bolus cisplatin 100 mg/m2 on days 1, 22, 43 concurrent with radiation therapy) as a standard of care (Figure)
Design and results of an intergroup trial. (Adapted from Adelstein DJ, Li Y, Adams GL, et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J Clin Oncol 2003;21: 92–98.)
In a three-arm randomized phase III trial of 295 patients with locally advanced (unresectable) stage M0 head and neck squamous cell carcinoma:
The treatment groups were radiation therapy alone (70 Gy) versus identical radiation plus concurrent cisplatin (100 mg / m2 administered intravenously on days 1, 22, and 43) versus a split course of radiation with cisplatin plus 5-FU
With a median follow up of 41 months:
The concurrent cisplatin / radiation arm had a significant advantage in:
Survival at 3 years compared with radiation alone:
37% versus 23%, p = .014
Survival in the split-course concurrent arm:
27% was not significantly better than that in the radiation arm
This improved efficacy comes at the cost of an increased incidence of acute toxicities, including:
Mucositis and nausea / vomiting:
Four toxic deaths occurred among 95 patients enrolled in the cisplatin chemoradiation arm
The intergroup Radiation Therapy Oncology Group (RTOG 91–11) trial for advanced larynx cancer (Figure):
Design and results of Radiation Therapy Oncology Group trial 91–11. (Adapted from Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349:2091–2098.)
Established concurrent bolus cisplatin with radiation as a standard of care
The study was open to patients with:
Squamous cell carcinoma of the glottic or supraglottic larynx
Patients with T1 disease or large-volume T4 disease:
Were excluded
Median follow-up of the study was:
3.8 years
Patients were randomly assigned to one of three larynx preservation strategies:
Induction cisplatin plus 5-FU followed by radiotherapy:
Patients with less then partial response after 2 cycles of PF:
Underwent laryngectomy followed by adjuvant radiotherapy
Radiotherapy with concurrent cisplatin
Radiotherapy alone
The dose of radiotherapy to the primary tumor and clinically positive nodes was:
70 Gy in all treatment groups
Severe or life-threatening mucositis in the radiation field:
Was almost twice as common in the concurrent treatment group compared with either the radiotherapy alone group or the sequential treatment group
The primary endpoint of the study was:
Preservation of the larynx
The rate of laryngeal preservation was:
84% for patients receiving radiotherapy with concurrent cisplatin
72% for patients receiving induction chemotherapy followed by radiation
67% for patients receiving radiation therapy alone
Distant metastases were reduced in patients who received either:
Concurrent chemoradiotherapy or induction chemotherapy followed by radiotherapy:
Compared with patients who received radiotherapy alone
Overall survival was not significantly different among the three treatment groups:
The lack of an overall survival difference between the three groups:
May be due to the contribution of salvage laryngectomy in all groups:
As well as a 2% increase in the incidence of death that may have been related to treatment in the concurrent chemoradiotherapy group compared with the other two treatment groups
It is important to recognize that the primary endpoint of the study was larynx preservation:
Not overall survival
The current standard of care for larynx preservation:
Remains concurrent high-dose cisplatin and radiation for patients who fit the eligibility criteria that were used in RTOG 91–11
Radiation Therapy Oncology Group trial 91–11: Rates of laryngeal preservation according to the treatment group. (Adapted from Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349:2091–2098.)
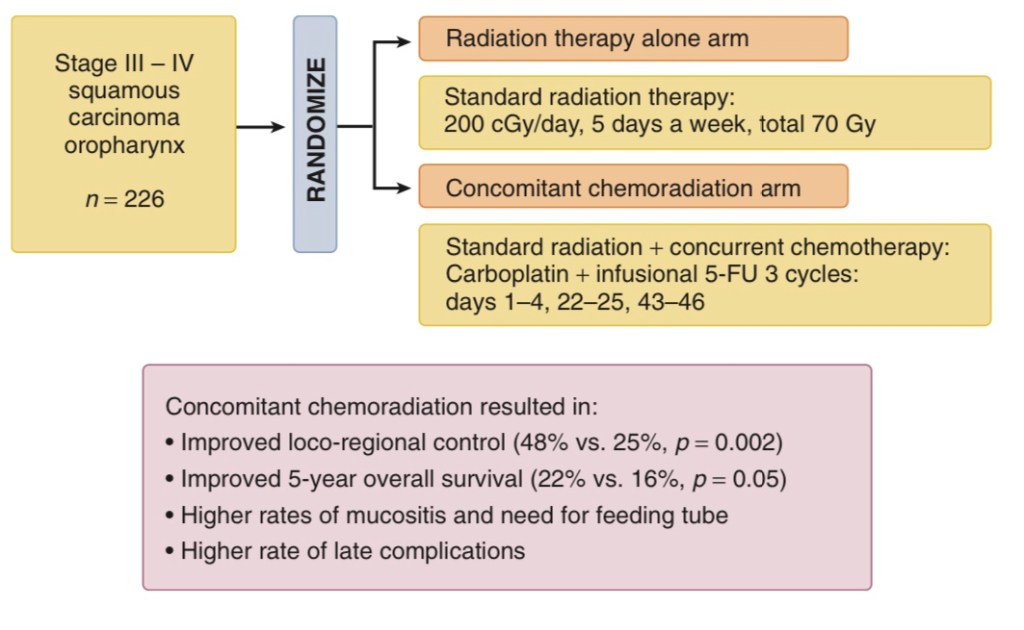
The Groupe d’Oncologie Radiotherapie Tete et Cou trial:
Is important because it evaluated the concomitant approach in patients with:
Oropharynx cancer only (Figure)
A total of 226 patients were randomly assigned to either radiation therapy alone (70 Gy) or radiation therapy (70 Gy) with concurrent carboplatin and infusion 5-FU
Significant benefits in 5-year:
Overall survival:
22% versus 16%, p = .05
Locoregional control:
48% versus 25%, p = .002
Were noted in the combined treatment arm
Complete responses were observed in a significant number of patients:
Thus avoiding the sequelae and short-term morbidity of surgical resection
Design and updated results of the Groupe d’Oncologie Radiotherapie Tete et Cou trial. 5-FU, 5-fluorouracil. (Adapted from Calais G, Alfonsi M, Bardet E, et al. Randomized trial of radiation therapy versus concomitant chemotherapy and radiation therapy for advanced-stage oropharynx carcinoma. J Natl Cancer Inst 1999;91:2081–2086 and Denis F, Garaud P, Bardet E, et al. Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol 2004;22:69–76.)
Phase II trials also support the feasibility of administering other chemotherapy regimens concurrently with radiation therapy for patients with locoregionally advanced head and neck cancer, including but not limited to:
Cisplatin plus paclitaxel
Cisplatin plus infusional 5-FU
5-FU plus hydroxyurea
Carboplatin plus paclitaxel
Paclitaxel, 5-FU, and hydroxyurea
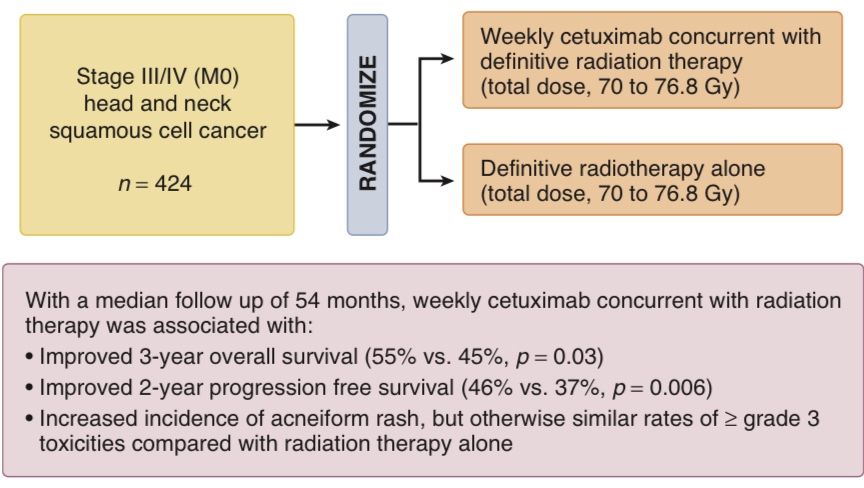
The role for cetuximab in combined modality therapy:
Was established when Bonner and colleagues randomly assigned 424 patients with locoregional advanced head and neck squamous cell cancer to treatment with:
Radiation therapy alone or radiation therapy with concurrent weekly cetuximab (Figure)
Design and results of the Bonner trial. (Adapted from Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med 2006; 354:567–578.)
Investigators were required to choose between one of three radiotherapy fractionation regimens:
With a total dose of 70 to 76.8 Gy
With a median follow-up of 54 months:
The combined treatment group had significantly improved:
3-year locoregional control:
47% versus 34%, p < .01
3-year overall survival:
55% versus 45%, p = .05
Compared with the group that received radiation therapy alone
Cetuximab was associated with an increased risk of:
Severe acneiform rash (17%) and severe infusion reaction (3%)
While cetuximab and radiotherapy is a valid treatment option for this patient population:
Retrospective studies have suggested that cetuximab may be associated with inferior outcomes compared with cisplatin and carboplatin plus infusional 5-FU:
Riaz et al., 2016; Shapiro et al., 2014
Recently, two randomized phase III trials were conducted to test if cetuximab may serve as a non-inferior and less toxic alternative to cisplatin in combination with radiation for patients with localized HPV-positive oropharyngeal carcinomas (which possess superior clinical outcomes with cisplatin chemoradiation compared to HPV-negative patients; Ang et al., 2010):
The De-ESCALaTE HPV trial:
Restricted enrollment to low risk HPV-positive patients (less than 10 pack-year smoking history):
They observed a significantly superior 2-year overall survival with cisplatin over cetuximab:
97.5% versus 89.4%; hazard ratio 5.0 [95% CI 1.7-14.7]; p=0.001; Mehanna et al., 2018
RTOG 1016 also demonstrated that among HPV-positive oropharyngeal cancer patients:
Cetuximab failed to meet the pre-specified non-inferiority criteria for overall survival compared to cisplatin:
Estimated 5-year overall survival of 77.9% [95% CI 73.4-82.5] with cetuximab versus 84.6% [95% CI 80.6-88.6] with cisplatin; Gillison et al., 2018
Both trials also demonstrated that toxicity rates were not significantly lower with cetuximab
Taken together, these prospective data argue strongly for prioritizing the use of cisplatin in these clinical settings and reserving the use of cetuximab with radiation in those who are not cisplatin-candidate