My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
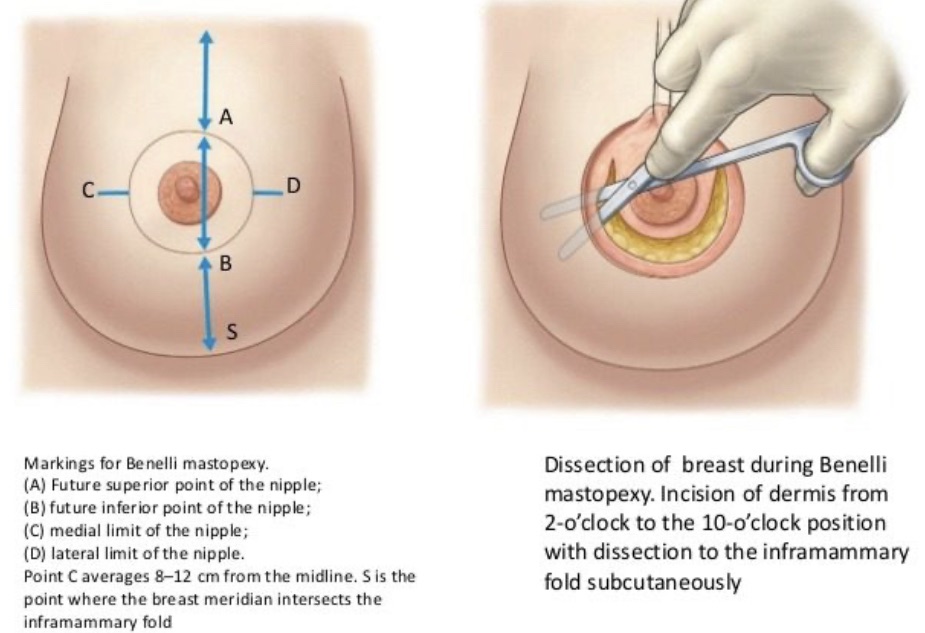
Is best used to address small to medium cancers centrally located in any quadrant
Results are best in patients with:
Grade 1 ptosis with enlarged nipple areola complex
This approach in patients with significant ptosis:
Will result in flattening of the central breast and would be better treated with other onocoplastic techniques
Treatment of triple negative breast cancers:
Should consider neoadjuvant chemotherapy prior to surgical excision
Young patients with triple negative breast cancer:
Also should consider hereditary risk assessment:
As this may alter their decision regarding breast conservation
Patients with a history of prior breast cancer treated with adjuvant radiation therapy:
Should not consider breast conservation unless there are special circumstances
References
Savalia NB, Silverstein MJ. Oncoplastic breast reconstruction: patient selection and surgical techniques. J Surg Oncol. 2016;113(8):875-882.
Piper M, Peled A, Sbitany H. Oncoplastic breast surgery: current strategies. Gland surg. 2015;4(2):154-163.
Clough KB, Kaufman GJ, Nos C, Buccimazza I, Sarfati IM. Improving breast cancer surgery: a classification and quadrant per quadrant atlas for oncoplastic surgery. Ann Surg Oncol 2010;17(5):1375-1391.
Omarini C, Guaitoli G, Pipitone S, Moscetti L, Cortesi L, Cascinu S, et al. Neoadjuvant treatments in triple-negative breast cancer patients: where we are now and where we are going. Cancer Manag Res. 2018;10:91-103.
In general, patients with significant ptosis of the breast:
Obtain better cosmetic results with a reduction mammoplasty compared to donut or Benelli mastopexy
Lesions distant to the nipple areolar complex:
Can be difficult to access through a mastopexy incision
References
Lebovic GS. Oncoplastic surgery: a creative approach to breast cancer management. Surg Oncol Clin N Am. 2010;19(3): 567-580.
Piper M, Peled A, Sbitany H. Oncoplastic breast surgery: current strategies. Gland Surg. 2015;4(2):154-163.
Clough, KB, Kaufman, GJ, Nos, C, Buccimazza, I, Sarfati, IM. Improving breast cancer surgery: a classification and quadrant per quadrant atlas for oncoplastic surgery. Ann Surg Oncol. 2010;17(5):1375-1391.
Clough KB, Benyahi D, Nos C, Charles C, Sarfati I. Oncoplastic surgery: pushing the limits of breast-conserving surgery. BreastJ. 2015;21(2):140-146.
Showed that in patients undergoing contralateral breast procedures at the time of oncoplastic breast-conserving surgery:
16.5% were found to have high-risk pathology in the contralateral breast:
With almost 5% of these being cancer
Larger studies from Europe have shown the contralateral occult malignancy rate:
To be 1% to 5%:
This rate of occult disease is higher than the reported occult malignancy rate in patients who are undergoing cosmetic reduction mammoplasty
Orientation of the specimen(s) from symmetry procedure may be beneficial when performing these operations in the setting of cancer treatment
References
Liang Y, Muse-Fisher C, Rambukwella M, Naber SP, Chatterjee A. Malignant and high-risk lesions in the contralateral breast symmetry mastopexy and reduction specimens when performing large-volume displacement oncoplastic surgery. Ann Plast Surg. 2019;82(4S Suppl 3):S185-S191.
Sorin T, Fyad JP, Pujo J, Colson T, Bordes V, Leroux A, et al. Incidence of occult contralateral carcinomas of the breast following mastoplasty aimed at symmetrization. Ann Chir Plast Esthet. 2014;59(2):e21-e28.
Use of oncoplastic surgery has become more common in the surgical treatment of breast cancer
Multiple studies have compared the surgical complication rates between standard breast-conserving surgery with oncoplastic breast-conserving surgery
A recent systematic review reported overall low rates of perioperative complications in patients who have undergone oncoplastic breast conserving surgery
Studies comparing oncoplastic breast-conserving surgery to standard breast-conserving surgery:
Have reported:
Lower rates of post-operative seroma formation
No difference in surgical site infection
Lower positive margin and re-excision rates
Additional reports have shown this same low risk of perioperative complications in the obese population:
Making oncoplastic surgery an option even in obese women
References
Carter SA, Lyons GR, Kuerer HM, Bassett RL Jr, Oates S, Thompson A, et al. Operative and oncologic outcomes in 9861 patients with operable breast cancer: single-institution analysis of breast conservation with oncoplastic reconstruction. Ann Surg Oncol. 2016;23(10):3190-3198.
De La Cruz L, Blankenship SA, Chatterjee A, Geha R, Nocera N, Czerniecki BJ, et al. Outcomes after oncoplastic breast-conserving surgery in breast cancer patients: a systematic literature review. Ann Surg Oncol. 2016;23(10):3247-3258.
Tong WM, Baumann DP, Villa MT, Mittendorf EA, Liu J, Robb GL, et al. Obese women experience fewer complications after oncoplastic breast repair following partial mastectomy than after immediate total breast reconstruction. Plast Reconstr Surg. 2016;137(3):777-791
Diagnosis of a breast cancer during pregnancy requires a complex treatment plan with multiple multidisciplinary providers:
From both oncology and obstetrics:
Coordinating the timing of cancer treatment and the delivery of a high-risk pregnancy
Gestational or pregnancy-associated breast cancer:
Refers to any breast cancer diagnosed:
During pregnancy or within the first year after childbirth
This is a rare diagnosis:
Yet remains the most common cancer in pregnant women:
Affecting approximately 15 to 35 per 100,000 deliveries:
Approximately 0.05%
The majority of pregnancy-associated breast cancers are:
Ductal in origin, more likely to be poorly-differentiated, ER negative, PR negative and HER2-positive:
Compared to non-pregnant women, and present at advanced stages
Evaluation of a dominant breast mass should include:
Ultrasound and mammogram with fetal shielding, and core biopsy
Interpretation of mammography can be difficult in the highly dense tissue of pregnant women
Use of MRI during pregnancy is both contraindicated and unhelpful:
Gadolinium contrast may cause fetal harm during the first trimester and is typically avoided
Although the majority (approximately 80%) of breast biopsies in pregnant women will be benign:
It is critical that malignancy be ruled out
Fine needle aspiration during pregnancy is associated with a higher rate of false positive and false negative results, without receipt of tumor markers:
Therefore core biopsy is recommended
Staging should be performed in women with advanced disease, and in those with symptoms concerning for metastases:
This should include chest radiograph with fetal shielding, liver ultrasound or MRI without contrast, and “low-dose” radionuclide bone scans
When possible, treatment of pregnancy-associated breast cancers:
Should follow similar guidelines to non-pregnant patients, and if at all possible, the pregnancy should be carried to term
Systemic treatment of breast cancer during pregnancy involves special consideration of both the mother and baby
Surgery is safe at all stages
Chemotherapy:
Can be delivered from 14 weeks of gestation following completion of organogenesis through 35 weeks:
When it should be stopped to avoid leukopenia in preparation for delivery
Data from a single-institution prospective study indicates that:
FAC chemotherapy (5-FU, doxorubicin, and cyclophosphamide) is safe during the second and third trimesters
With fetal malformations approximating 1%
Experience with taxanes remained limited, but National Comprehensive Cancer Network (NCCN) guidelines:
Recommend weekly paclitaxel if warranted
Methotrexates:
Are contraindicated due to teratogenic side effects
Although 20% of pregnancy-associated breast cancers are HER2-positive:
Anti-HER2 therapy including trastuzumab has not been proven safe during pregnancy and is best delivered in the adjuvant setting:
MotHER a prospective U.S. registry, is evaluating women exposed to trastuzumab +/- pertuzumab during pregnancy or within 6 months of conception and following pregnancy outcomes and infants for the first month of life
Current recommendations suggest that targeted anti-HER2 therapy be delayed until after delivery
Breast conservation:
Is not recommended if radiation would be timed during pregnancy because this is contraindicated:
However, it can be performed if radiation falls after delivery
Axillary lymph node dissection was previously recommended:
But sentinel lymph node biopsy is feasible and should be offered
Hormone therapy should be postponed until after childbirth
Chemotherapy during pregnancy can cause concerns for the fetus which depend on the timing of drug administration:
Congenital malformations can occur in the first trimester
In the second and third trimesters prematurity, low birth weight and myelosuppression are the greatest concerns
Among approved chemotherapy agents, long-term outcomes of children with in-utero exposure demonstrate normal development, cognition, and school performance when prematurity is controlled for
References
Macdonald HR Pregnancy associated breast cancer. Breast J. 2020 Jan 14. doi: 10.1111/tbj.13714. [Epub ahead of print]
Goidescu I, Nemeti G, Caracostea G, Eniu DT, Chiorean A, Pintican R, Cruciat G, Muresan D. The role of imaging techniques in the diagnosis, staging and choice of therapeutic conduct in pregnancy associated breast cancer. Med Ultrason. 2019 Aug 31;21(3):336-343. doi: 10.11152/mu-1958. Review.
Alfasi A, et al. Breast Cancer During Pregnancy- Current Paradigms, Paths to Explore. Cancers. 2019; 11: 1669
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Breast Cancer. Available with login at: https://subscriptions.nccn.org.
Gooch JC1,2, Chun J1, Kaplowitz E1, Guth A1, Axelrod D1, Shapiro R1, Roses D1, Schnabel F1. Pregnancy-associated breast cancer in a contemporary cohort of newly diagnosed women Breast J. 2019 Aug 25. doi: 10.1111/tbj.13510. [Epub ahead of print]
Chemotherapy is typically recommended to improve breast cancer operability or downstage the axilla among medically fit patients
Neoadjuvant endocrine therapy (NET) is a good option for post-menopausal women with ER+ breast cancers:
When aiming for improved candidacy for breast conservationor in patients in whom chemotherapy will not be safely tolerated
Studies evaluating NET have demonstrated similar rates of clinical and radiographic response and breast conservation therapy (BCT) to those reported from studies using neoadjuvant chemotherapy
When neoadjuvant chemotherapy (4 cycles of doxorubicin and paclitaxel) was compared directly to NET (12 weeks of aromatase inhibitors; exemestane or anastrozole):
NET was associated with comparable clinical response, higher rates of breast conservation (33% vs. 24%), and no difference in local recurrence at approximately 3 years
Meta-analysis and clinical trial data support use of aromatase inhibitors (letrozole or anastrozole) over tamoxifen, including:
Higher clinical and radiographic response rates (55% vs. 36%)
Improved rates of BCT (45% versus 35%)
The ACOSOG Z1031 trial demonstrated comparable effectiveness of exemestane, letrozole and anastrozole for 16 to 18 weeks before surgery
NET requires a longer duration of treatment than preoperative chemotherapy and depends on the patient’s individual eligibility for breast conservation
NET is typically recommended for 3 to 6 months prior to surgery; however, extended treatment for up to 12 months has been safe and is associated with a greater response to treatment
Although tumor progression is rare on NET, continued surveillance is important for women with an intact primary breast tumor taking endocrine therapy, and cancer growth would be an indication for surgery
The majority of clinical trials for NET have focused on postmenopausal women, in that younger patients often have higher-risk tumor biology and are likely candidates for chemotherapy:
Thus, data on the use of NET in premenopausal patients are limited to phase II trials and include ovarian suppression plus aromatase-inhibitors (i.e., exemestane+goserelin).
References
Semiglazov VF, Semiglazov VV, Dashyan GA, Ziltsova EK, Ivanov VG, Bozhok AA, et al. Phase 2 randomized trial of primary endocrine therapy versus chemotherapy in postmenopausal patients with estrogen receptor-positive breast cancer. Cancer. 2007;110(2):244-254.
Ellis MJ, Ma C. Letrozole in the neoadjuvant setting: the P024 trial. Breast Cancer Res Treat. 2007;105(suppl 1):133-143.
Eiermann W, Paepke S, Appfelstaedt J, Llombart-Cussac A, Eremin J, Vinholes J, et al. Preoperative treatment of postmenopausal breast cancer patients with letrozole: a randomized double-blind multicenter trial. Ann Oncol. 2001;12(11):1527-1532.
Smith IE, Dowsett M, Ebbs SR, Dixon JM, Skene A, Blohmer JU, et al. Neoadjuvant treatment of postmenopausal breast cancer with anastrozole, tamoxifen, or both in combination: The Immediate Preoperative Anastrozole, Tamoxifen, or Combined with Tamoxifen (IMPACT) multicenter double-blind randomized trial. J Clin Oncol. 2005;23(22):5108-5116.
Cataliotti L, Buzdar AU, Noguchi S, Bines J, Takatsuka Y, Petrakova K, et al. Comparison of Anastrozole versus tamoxifen as preoperative therapy in postmenopausal women with hormone receptor-positive breast cancer: the pre-operative “arimidex” compared to tamoxifen (PROACT) trial. Cancer. 2006;106(10):2095-2103.
Ellis MJ, Suman VJ, Hoog J, Lin L, Snider J, Prat A, et al. Randomized phase II neoadjuvant comparison between letrozole, anastrozole, and exemestane for postmenopausal women with estrogen receptor-rich stage 2 to 3 breast cancer: clinical and biomarker outcomes and predictive value of the baseline PAM5-based intrinsic subtype—ACOSOG Z1031. J Clin Oncol. 2011;29(17):2342-2349.
Anthracycline-based drugs including doxorubicin and cyclophosphamide followed by a taxane
Higher risk HER2-negative breast cancers (node-positive hormone-receptor positive patients and triple-negative patients) typically receive anthracycline and taxane-based regimens with or without carboplatin
Notably, results from the CALGB40603 trial suggested that for triple-negative breast cancer:
The addition of carboplatin to NAC resulted in a 14% increase in eligibility for breast conservation
References:
Fayanju OM, et al. The Clinical Significance of Breast-only and Node-only Pathologic Complete Response After Neoadjuvant Chemotherapy. Annals of Surgery. 2018; 268(4): 591-601.
von Minckwitz, G et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. NEJM. 2018; 380(7): 617-628.
Masuda N, et al. Adjuvant Capecitabine for Breast Cancer After Preoperative Chemotherapy. NEJM. 2017; 376:2147-59.
Golshan M, et al. Impact of neoadjuvant chemotherapy in stage II-III triple negative breast cancer on eligibility for breast-conserving surgery and breast conservation rates: surgical results from CALGB 40603 (Alliance). Annals of Surgery. 2015; Sep; 262(3):434-9.
The brain is frequently reported as the first site of relapse:
In women with HER2-positive breast cancer treated with trastuzumab
It is known that up to 50% of patients with HER2 positive metastatic breast cancer:
Will develop brain metastasis
References
Pestalozzi BC, Zahrieh D, Price KN, et al. Identifying breast cancer patients at risk for Central Nervous System metastases in trials of the International Breast Cancer Study Group (IBCSG). Annals of oncology : official journal of the European Society for Medical Oncology. 2006;17(6):935-944.
Pestalozzi BC, Holmes E, de Azambuja E, Metzger-Filho O, Hogge L, Scullion M, et al. CNS relapses in patients with HER2-positive early breast cancer who have and have not received adjuvant trastuzumab: a retrospective substudy of the HERA trial (BIG 1-01). Lancet Oncol. 2013;14(3):244-248.
The CDK 4/6 inhibitors are a class of oral drugs that have been approved for HR+, HER2-negative metastatic breast cancer in the first-line setting or after progression on prior aromatase inhibitor
In the MONALEESA-3 trial:
Ribociclib in combination with fulvestrant:
Showed progression-free survival (20.5 months vs. 12.8 months) and overall survival benefit over fulvestrant alone in HR+, HER2-negative metastatic breast cancer that was either treatment naïve or had up to one prior line of endocrine therapy
Everolimus is an mTOR inhibitor with evidence of benefit in the metastatic setting after prior aromatase inhibitor:
However it is FDA-approved in combination with exemestane per the BOLERO-2 trial
In the metastatic setting:
Radiation is generally pursued to palliate symptoms or control isolated disease that is not responding to systemic therapy
References
Slamon DJ, Neven P, Chia S, Fasching PA1, De Laurentiis M1, Im SA, et al. Phase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J Clin Oncol. 2018;36(24):2465-2472.
Slamon DJ NP, Chia S, et al. Overall survival (OS) results of the phase III MONALEESA-3 trial of postmenopausal patients (pts) with hormone receptor-positive (HR+), human epidermal growth factor 2-negative (HER2-) advanced breast cancer (ABC) treated with fulvestrant (FUL) + ribociclib (rib). Paper presented at: ESMO; September 27 to October 1, 2019, 2019; Barcelona, Spain.
Baselga J, Campone M, Piccart M, Burris HA 3rd, Rugo HS, Sahmoud T, et al. Everolimus in postmenopausal hormone-receptor–positive advanced breast cancer. N Engl Med. 2011;366(6):520-529
Premenopausal women were given ovarian function suppression with adjuvant aromatase inhibitor or tamoxifen:
Outcomes were compared to tamoxifen alone for 5 years
The SOFT / TEXT trials showed a:
Disease-free survival benefit of 2.1%
Overall survival benefit of 4.3%:
At 8 years with GnRH agonist and tamoxifen over tamoxifen alone in the cohort of women who had prior chemotherapy
Premenopausal patients with high-risk disease and who received prior chemotherapy:
The most effective adjuvant endocrine therapy would include ovarian function suppression with a GnRH agonist per the SOFT / TEXT trials
Tamoxifen alone:
Is still an effective endocrine therapy and would be appropriate if the patient chooses not to use ovarian function suppression
In premenopausal patients an aromatase inhibitor would be ineffective unless she was rendered post-menopausal
Raloxifene is a selective ER modulator similar to tamoxifen:
It is FDA-approved only for breast cancer risk reduction in post-menopausal women
Oophorectomy alone is not as effective without additional endocrine therapy
References
Francis PA, Regan MM, Fleming GF, Lang I, Ciruelos E, Bellet M, et al. Adjuvant ovarian suppression in premenopausal breast cancer. New Engl J Med. 2015;372(5):436-446.
Francis PA, Pagani O, Fleming GF, Walley BA, Colleoni M, Lang I, et al. Tailoring adjuvant endocrine therapy for premenopausal breast cancer. N Engl J Med. 2018;379(2):122-137.
Vogel VG. The NSABP Study of Tamoxifen and Raloxifene (STAR) trial. Expert review of anticancer therapy. 2009;9(1):51-60.