My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Management of euthyroid patients with positive thyroid antibody titers:
Can typically be monitored without the institution of thyroid hormone replacement therapy:
However, there are some data that pregnant patients with positive thyroid antibody titers may have improved pregnancy outcomes and reduced complications with the institution of LT4 replacement therapy
In non-pregnant patients with hypothyroidism:
There are standard recommendations for treatment and monitoring:
This usually consist of LT4 therapy and TSH and FT4 monitoring every 6 weeks with adjustments in LT4 dosing until the TSH is within the goal range (typically 1 to 3 uIU/mL) although a higher target range is considered acceptable in the elderly patients
Stavros has proposed the following BIRADS categories for breast ultrasound (see Table)
Proposed BIRADS categories for breast ultrasound.
The American College of Radiology classification:
Subdivides category 4 into:
BIRADS 4a:
Which has a 2% to 10 % risk of malignancy
BIRADS 4b:
Which has a 10% to 50 % risk of malignancy
BIRADS 4c:
Which has a 50% to 95% risk malignancy
BIRADS 5:
Has 95% or greater chance of malignancy
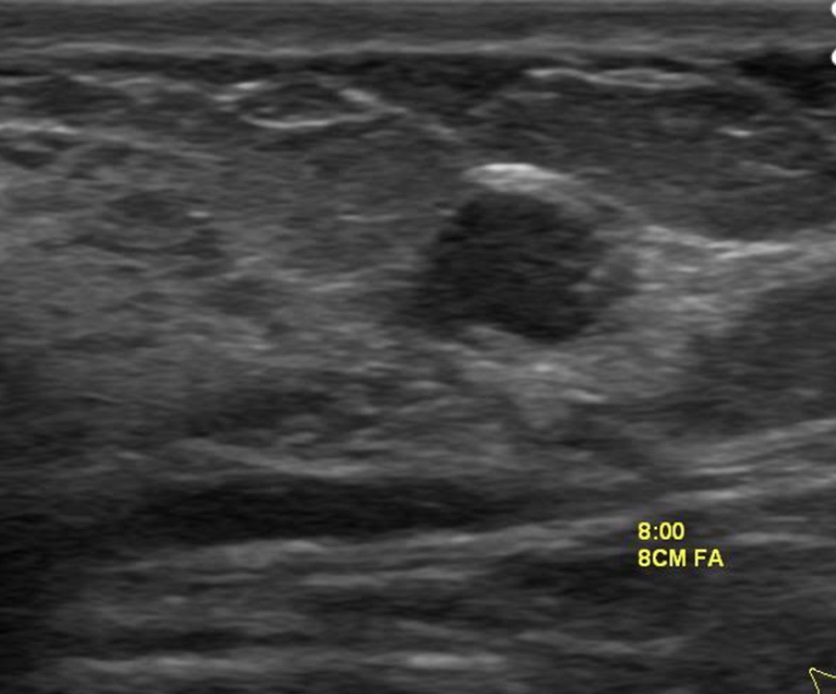
In evaluating a solid sonographic nodule:
One should first look for any of the 10 signs of malignancy, and if even 1 of them is present:
The lesion cannot be considered BIRADS 3
The signs of malignancy are:
Shadowing
Hypoechoic echotexture
Spiculation
Angular margins
Thick echogenic halo
Microlobulation
Taller than wide
Duct extension
Branching pattern
Calcifications
Note that Stavros compares the echogenicity of lesions to that of breast fat, not breast parenchyma:
Therefore, a lesion with hypoechoic echotexture would be very hypoechoic if breast parenchyma is used as the reference
The hypoechoic lesion in the image does not have smooth margins but appears microlobulated
Regardless of whether the classification of Stavros or the American College of Radiology is used:
The risk of the lesion in this patient is not low enough to be considered BIRADS 3 nor high enough risk to warrant BIRADS 5:
Thus, it falls somewhere in the BIRADS 4 range:
Biopsy is required
References:
D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. 5th ed. Reston, VA: American College of Radiology; 2013
Jales RM, Sarian LO, Torresan R, Marussi EF, Alvares BR, Derchain S. Simple rules for ultrasonographic subcategorization of BI-RADS®-US 4 breast masses. Eur J Radiol. 2013;82(8):1231-1235.
Stavros AT. Breast Ultrasound. Philadelphia, PA: Lippincott Williams & Wilkins; 2004.
• General Surgery • Michigan State University: • 2005 to 2010• Complex Surgical Oncology / Head and Neck Surgery / Endocrine Surgery: • Fox Chase Cancer Center (Filadelfia): • 2010 to 2012• Masters in Science (Clinical research for health care professionals): • Drexel University (Filadelfia): • 2010 to 2012• Head and Neck Surgery and Oncology • IFHNOS / Memorial Sloan Kettering Cancer Center: • 2014 to 2016
With normal thyroid-stimulating hormone (TSH) and free thyroxine (FT4) levels
Subclinical hypothyroidism:
With mild TSH elevations (5 to 10 uIU/ mL), and a paucity of symptoms
Significant / overt hypothyroidism:
With TSH > 10 uIU/mL
Although a goiter may be noted during a physical examination:
Thyroid morphology associated with HT varies widely and ranges from:
Atrophic, barely palpable glands to slightly enlarged glands to very large goiters
The gland texture:
May be smooth as in“simple” goiters or contain numerous nodules as seen with multinodular goiters
Although the euthyroid state may persist for many years:
About 4% to 5% of initially euthyroid patients with HT will develop hypothyroidism each year:
The rate of progression is somewhat dependent on the intensity of the inflammatory reaction and the concomitant rate of induced thyroid follicle destruction
HT is usually not associated with any neck discomfort:
But there are instances where individuals will present with anterior neck pain or tenderness:
So HT should be considered in the differential diagnosis of patients with neck discomfort
Episodes of more acute thyroiditis:
With the development of transient thyrotoxicosis have been reported and been referred to as Hashitoxicosis
Changes from HT noted by thyroid ultrasound, such as:
Heterogeneous parenchyma:
May become evident before the ability to measure thyroid antibody titers in the patient’s serum
Although thyroid nodules certainly can be present in the context of HT:
Focal inflammatory changes due to HT may give the false impression of thyroid nodules:
The term pseudonodule refers to instances where there is the appearance of a thyroid nodule in at least one ultrasound view, but it cannot be reproduced on the additional complementary views:
Such lesions may not be evident upon future imaging at a later point in time
Therefore in patients with HT, the possibility of a pseudonodule should be considered before proceeding with FNA sampling
Thyroid enlargement associated with HT:
May regress with LT4 therapy:
Particularly if TSH elevation is present at the time of diagnosis:
However, some goiters associated with HT will persist or even grow whether or not LT4 suppression is used:
If such patients exhibit progressive goiter growth or develop compressive type symptoms thyroidectomy may need to be considered
If the goiter is large and especially if tracheal deviation or substernal extension is present:
Then preoperative imaging with computed tomography (CT) of the neck is warranted to better define the anatomy and help plan the surgical approach
Histopathology is typically notable for:
Prominent lymphocytic infiltration, foci of lymphoid germinal centers, and follicle destruction.
Controversy exists if HT patients have an increased risk for thyroid cancer and, if so, whether or not HT is associated with a more aggressive disease pattern
The recommended workup and staging of DCIS includes:
History and physical examination
Bilateral diagnostic mammography
Pathology review
Determination of tumor estrogen receptor (ER) status
MRI as indicated is special situations
For pathology reporting:
The NCCN panel endorses the College of American Pathologists Protocol:
For both invasive and noninvasive carcinomas of the breast
The NCCN panel recommends testing for ER status:
In order to determine the benefit of adjuvant endocrine therapy or risk reduction
Although the tumor HER2 status is of prognostic significance in invasive cancer, its importance in DCIS has not been elucidated:
To date, studies have either found unclear or weak evidence of HER2 status as a prognostic indicator in DCIS
The NCCN Panel has concluded that knowing the HER2 status of DCIS does not alter the management strategy and is not required DCIS
The role of MRI in management of DCIS remains unclear:
MRI has been prospectively shown to have a sensitivity of up to 98% for high-grade DCIS
In a prospective, observational study of 193 women with pure DCIS who underwent both mammography and MRI imaging preoperatively:
93 (56%) women were diagnosed by mammography and 153 (92%) were diagnosed by MRI (P < .0001)
Of the 89 women with high-grade DCIS:
43 (48%) who were not diagnosed by mammography:
Were diagnosed by MRI alone
However, other studies suggest that MRI can overestimate the extent of disease:
Therefore, surgical decisions should not be not be solely based on MRI results especially when mastectomy is being contemplated
If MRI findings suggest more extensive disease than is seen on mammography such that a markedly larger resection is required for complete excision:
The findings should be verified histologically through MRI-guided biopsy of the more extensive enhancement
Studies have also been performed to determine whether the use of MRI reduces re-excision rates and decreases local recurrence in women with DCIS:
No reduction in re-excision rates was seen in women undergoing lumpectomy following MRI compared with those who did not undergo preoperative MRI
The NCCN Panel recommends only performing breast MRI for DCIS in select circumstances where additional information is warranted during the initial workup, noting that the use of MRI has not been shown to increase likelihood of negative margins or decrease conversion to mastectomy for DCIS
Primary Treatment for DCIS:
The goal of primary therapy for DCIS:
Is to prevent progression to invasive breast carcinoma
Management strategies for DCIS treatment include:
Surgery:
Mastectomy or lumpectomy
Radiation therapy
Adjuvant endocrine therapy:
To reduce risk of recurrence
Surgery:
Excision of DCIS using a breast-conserving approach (lumpectomy) with or without whole breast radiation therapy (WBRT) or alternatively, mastectomy:
Are the primary treatment options for individuals with DCIS:
The choice of local treatment does not impact overall disease-related survival:
Therefore, the individual patient’s acceptance of the potential for an increased risk of local recurrence must be considered
Post-excision mammography:
Is valuable in confirming that an adequate excision of DCIS has been performed particularly for DCIS patients who initially present with microcalcifications
Mastectomy:
Patients with DCIS and evidence of widespread disease (ie, disease involving two or more quadrants) on diagnostic mammography or other imaging, physical examination, or biopsy:
May require mastectomy
Mastectomy permanently alters the lymphatic drainage pattern to the axilla:
So that future performance of a sentinel lymph node biopsy (SLNB) is not technically feasible
Therefore, for DCIS patients who intend on treatment with mastectomy, or alternatively, for local excision in an anatomic location that could compromise the lymphatic drainage pattern to the axilla (eg, tail of the breast):
A SLNB procedure should strongly be considered at the time of definitive surgery to avoid necessitating a full axillary lymph node dissection for evaluation of the axilla
Complete axillary lymph node dissection (ALND):
Is not recommended unless there is pathologically documented invasive cancer or axillary lymph node metastatic disease in patients (by either biopsy or SNLB)
However, a small proportion of women (about 25%) with seemingly pure DCIS on initial biopsy:
Will have invasive breast cancer at the time of the definitive surgical procedure and thus will ultimately require ALN staging
Lumpectomy plus Whole Breast Radiation Therapy (WBRT):
Breast conserving therapy (BCT) includes lumpectomy to remove the tumor with negative surgical margins followed by WBRT to eradicate any residual microscopic disease
Several prospective randomized trials of pure DCIS have shown that the addition of WBRT after lumpectomy:
Decreases the rate of in-breast disease recurrence, or distant metastasis-free survival
In the long term follow-up of the RTOG 9804 trial, at 7 years:
The local recurrence rate was:
0.9% (95% CI, 0.0%–2.2%) in the radiation therapy arm versus 6.7% (95% CI, 3.2%–9.6%) in the observation arm (HR, 0.11; 95% CI, 0.03– 0.47; P < .001)
In the subset of patients with good-risk disease features:
The local recurrence rate was low with observation but was decreased significantly with the addition of radiation therapy
A meta-analysis of four large multicenter randomized trials:
Confirms the results of the individual trials, demonstrating that the addition of WBRT after lumpectomy for DCIS:
Provides a statistically and clinically significant reduction in ipsilateral breast events (HR [hazard ratio], 0.49; 95% CI; 0.41–0.58, P < .00001)
However, these trials did not show that the addition of RT has an overall survival benefit
The long-term follow-up of the NSABP B-17 showed that at 15 years:
Radiation therapy resulted in a 52% reduction of ipsilateral invasive recurrence compared with excision alone (HR, 0.48; 95% CI, 0.33–0.69, P < .001)
However, overall survival (OS) and cumulative all-cause mortality rates through 15 years were similar between the two groups (HR for death, 1.08; 95% CI, 0.79–1.48)
Similar findings were reported by a large observational study of the SEER database that included 108,196 patients with DCIS:
In a subgroup analysis at 10 years, of 60,000 women treated with breast-conserving therapy, with or without radiation therapy:
Radiation therapy was associated with a 50% reduction in the risk of ipsilateral recurrence (adjusted HR, 0.47 [95% CI, 0.42–0.53]; P < .001), however, breast cancer-specific mortality was found to be similar (HR, 0.86 [95% CI, 0.67–1.10]; P = .22)
More recently, in a population-based study, the use of WBRT in patients with higher-risk DCIS:
Higher nuclear grade, younger age, and larger tumor size:
Was demonstrated to be associated with a:
Modest, but statistically significant improvement in survival
RT Boost:
The use of RT boost has been demonstrated to provide a small but statistically significant reduction in IBTR risk (4% at 20 years):
In all age groups for invasive breast cancer
Recently, a pooled analysis of patient-level data from ten academic institutions evaluated outcomes of pure DCIS patients:
All treated with lumpectomy and WBRT (n = 4131) who either received RT boost with a median dose of 14 Gy (n = 2661) or received no boost (n = 1470):
The median follow-up of patients was nine years
A decrease in IBTR was seen in patients who received boost compared with those who did not at:
5 years (97.1% vs 96.3%)
10 years (94.1% vs 92.5%)
15 years (91.6% vs 88.0%)
P = .0389 for all
The use of RT boost was associated with significantly decreased IBTR across the entire cohort of patients (hazard ratio [HR], 0.73; 95% CI, 0.57-0.94; P = .01)
In a multivariate analysis that took into account factors associated with lower IBTR, including grade, ER positive status, use of adjuvant tamoxifen, margin status, and age:
The benefit of RT boost still remained statistically significant (hazard ratio, 0.69; 95% confidence interval [CI], 0.53 – 0.91; P < .010)
Even in patients considered very low risk based on negative margins status (defined as no ink on tumor as per National Surgical Adjuvant Breast and Bowel Project definition, or margins 10 mm or no tumor on re-excision in 48 % of patients)
Although the rate of IBTR were acceptably low for the low-/intermediate grade group at the 5 years, at a median follow-up time of 12.3 years, the rates of developing an IBTR were 14.4% for low/intermediate-grade and 24.6% for high grade DCIS (P = .003)
This suggests that IBTR events may be delayed but not prevented in the seemingly low-risk population
Therefore, the NCCN panel concluded that for DCIS patients treated with lumpectomy alone (without radiation), irrespective of margin width:
The risk of IBTR is substantially higher than treatment with excision followed by whole breast radiation therapy (even for predefined low-risk subsets of DCIS patients)
Therefore, historically management was a mastectomy without nodal assessment
Recently, more patients are undergoing lumpectomy for this lesion
Researchers believe that local recurrence rates are similar for borderline and malignant phyllodes tumors
Local recurrence is lower with negative margins:
Historically, 1 cm margins have been recommended for malignant and borderline phyllodes tumors and continue to be recommended in the current 2024 NCCN guidelines:
The guidelines however note that while narrow margins are associated with an increased risk for local recurrence they are not an absolute indication for mastectomy
Newer data may suggest a smaller margin is adequate:
Spanheimer et al identified local recurrences in 16% of 71 patients with borderline or malignant phyllodes tumors undergoing breast-conserving surgery
Some of these patients had a positive or close (< 1 mm) margin
When the subset of patients with a margin > 1 mm was considered, the local recurrence rate was 12%
In addition, radiation may play a role in decreasing the risk of local recurrence:
In a prospective, multi-institutional study, 46 patients (30 with malignant phyllodes tumors and 16 with borderline phyllodes tumors) underwent margin-negative resections followed by radiation therapy:
Eight of these patients had margins < 2 mm
After 10 years of observation for all patients, none had developed a local recurrence
In another study using data from the National Cancer Database, Gnerlich et al. showed that adjuvant radiation therapy decreased the risk of local recurrence after resection of phyllodes tumors by more than half (hazard ratio [HR] 0.43, 95% confidence interval [CI] 0.19–0.95)
References:
Tan, BY, Acs, G, Apple, SK, et al. Phyllodes tumor of the breast: a consensus review. Histopathology. 2016;68(1):5-21.
Spanheimer P, Murray M, Zabor E, et al. Long term outcomes after surgical treatment of malignant/borderline phyllodes tumors of the breast. Ann Surg Oncol.2019;26(7):2136-2143.
Barth R, Wells W, Mitchell S, Cole B. A prospective, multi-institutional study of adjuvant radiation therapy after resection of malignant phyllodes tumors. Ann Surg Oncol. 2009;16(8):2288-2294.
Gnerlich J, Williams R, Yao K, Jaskowiak N, Kulkarni S. Utilization of radiotherapy for malignant phyllodes tumors: analysis of the National Cancer Database 1998–2009. Ann Surg Oncol. 2014;21(4):1222-1230
The Society of Surgical Oncology / American Society for Radiation Oncology (SSO / ASTRO) 2014 Consensus Guidelines:
Regarding margins of resection for invasive carcinoma of the breast:
Recommend the use of “no ink on tumor” as the standard
Patients with invasive cancer:
Even with associated ductal carcinoma in situ (DCIS), are treated according to these guidelines
In a meta-analysis of 33 studies including 32,363 patients:
Odds of local recurrence were associated with margin status of positive vs. negative:
But not decreased with increasing margin distance for patients with invasive carcinoma
The study reported that rates of in-breast tumor recurrence are twice as high with positive margins:
Regardless of tumor biology, radiation boost, or endocrine therapy:
There was no evidence that wide margins reduce recurrence, even in patients with extensive intraductal component
However, the American Society of Clinical Oncology (ASCO) guidelines recommend consideration of post-excision mammography to document adequate resection in patients with microcalcifications
References:
Moran MS, Schnitt SJ, Giuliano AE, et al. SSO-ASTRO consensus guideline on margins for breast-conserving surgery with whole breast irradiation in stage I and II invasive breast cancer. Int J Radiat Oncol Biol Phys. 2014;88(3):553-564.
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21(3):717-730.
Buchholz TA, Somerfield MR, Griggs JJ, et al. Margins for breast-conserving surgery with whole-breast irradiation in stage I and II invasive breast cancer: American Society of Clinical Oncology endorsement of the Society of Surgical Oncology/American Society for Radiation Oncology consensus guideline. J Clin Oncol.2014;32(14):1502-1506.
Sentinel Lymph Node Surgery After Neoadjuvant Chemotherapy in Patients With Node-Positive Breast Cancer / The ACOSOG Z1071 (Alliance) Clinical Trial
According to the ACOSOG Z1071 study for patients who had positive nodes pre-chemotherapy and then had a sentinel node biopsy the false-positive rate was less than 10%:
If dual tracer was used
Greater than two sentinel nodes were removed
Any clipped nodes were included
If only one lymph node was removed:
The false-negative rate was unacceptably high and further axillary surgery was needed
Until the Alliance 11202 trial is completed:
The standard treatment remains an axillary dissection for positive nodes after chemotherapy
References
Boughey JC, Suman VJ, Mittendorf EA, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) Clinical Trial. JAMA. 2013; 310(14): 1455-1461. doi: 10.1001/jama.2013.278932.