My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
A tumor bed boost has consistently been shown to reduce rates of local recurrence in patients undergoing breast-conserving surgery:
However, limited data have been available for patients with ductal carcinoma in situ (DCIS)
Moran et al. retrospectively evaluated 4,131 patients with DCIS:
Finding that the addition of a tumor bed boost:
Reduced ipsilateral breast tumor recurrences, with the benefit being:
0.8% at 5 years
1.6% at 10 years
3.6% at 15 years
The American Society for Radiation Oncology (ASTRO) has published guidelines on the use of a tumor bed boost following whole-breast irradiation:
It is important to note that the range of boost doses depend on surgical margins following lumpectomy
References
Bartelink H, Maingon P, Poortmans PM, et al. Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. Lancet Oncol. 2015;16(1):47-56.
Romestaing P, Lehingue Y, Carrie C, et al. Role of a 10-Gy boost in the conservative treatment of early breast cancer: results of a randomized clinical trial in Lyon, France. J Clin Oncol. 1997;15(3):963-968.
Moran MS, Zhao Y, Ma S, et al. Association of radiotherapy boost for ductal carcinoma in situ with local control after whole-breast radiotherapy. JAMA Oncol.2017;3(8):1060-1068.
Smith BD, Bellon JR, Blitzblau R, et al. Radiation therapy for the whole breast: Executive summary of an American Society for Radiation Oncology (ASTRO) evidence-based guideline. Pract Radiat Oncol. 2018;8(3):145-152.
Morrow M, Van Zee KJ, Solin LJ, et al. Society of Surgical Oncology-American Society for Radiation Oncology-American Society of Clinical Oncology consensus guideline on margins for breast-conserving surgery with whole breast irradiation in ductal carcinoma in situ. Pract Radiat Oncol. 2016;6(5):287-295.
An experienced dermatopathologist is an important member of the multidisciplinary melanoma team:
That contributes to the accurate diagnosis and staging of patients with melanoma
It is my practice to have outside biopsies reviewed by our pathology staff upon referral to confirm diagnosis
Although the pathologic analysis primarily consists of microscopic examination of hematoxylin- and eosin-stained tumor:
Several melanocytic cell markers may also be useful to confirm the diagnosis
Two antibodies that have been widely used in immunohistochemical evaluations are:
S-100 and HMB-45:
S-100 is expressed not only by more than 90% of melanomas:
But also by several other tumors and some normal tissues, including dendritic cells
In contrast, the monoclonal antibody HMB-45:
Is relatively specific (yet not as sensitive) for proliferative melanocytic cells and melanoma
It is therefore often used as a confirmatory stain when the diagnosis of melanoma is being considered
Anti–MART-1 staining has also been shown to be very useful in the diagnosis of melanoma:
Antityrosinase and Sox10 may also be used
The major histomorphologic components that should be included in a primary melanoma pathology report include:
Breslow thickness
Ulceration status
Peripheral and deep margin status
Mitotic rate:
Using the dermal hot spot approach with units of mitoses per mm2
Other features that are often also recorded include:
Presence of microsatellites
Histologic subtype
Lymphovascular invasion
Tumor-infiltrating lymphocytes (TIL)
Regression
Neurotropism
Growth phase
The absence of epidermal component:
As the latter may represent an uncommon dermal primary or a metastatic deposit
The major histomorphologic types of melanoma:
Superficial spreading melanomas:
Constitute the majority of melanomas:
Approximately 70% of melanomas
Generally arise in a pre-existing nevus
Nodular melanomas:
Are the second most common type:
15% to 30% of melanoma
Nodular melanomas progress to invasiveness more quickly than other types:
However, when depth of the melanoma is controlled for:
Nodular melanomas are generally associated with the same prognosis as other lesions:
Although at least one recent study suggests that a thin (T1) nodular melanoma may be associated with worse prognosis than T1 superficial spreading-type melanoma
Lentigo maligna melanomas:
Constitute a small percentage of melanomas:
4% to 10%
These lesions occur in sun-exposed areas
Lentigo maligna melanomas are classically located on:
The faces of older white women
In general, lentigo maligna melanomas are:
Large (> 3 cm at diagnosis)
Flat lesions
Are uncommon in individuals younger than 50 years
Given their often-ill-defined appearance:
Margin control can sometimes be challenging at the time of wide excision
Acral lentiginous melanomas:
Occur on the palms (palmar), soles (plantar), or beneath the nail beds (subungual):
Although not all palmar, plantar, and subungual melanomas:
Are acral lentiginous melanomas
These melanomas account for only 2% to 8% of melanomas in white patients:
But for a substantially higher proportion of melanomas (35% to 60%) in darker-skinned patients
They are often large:
With an average diameter of approximately 3 cm
Their clinical extent at the primary site may be difficult to define, and scouting biopsies are sometimes employed to facilitate clinical assessment of the extent of disease
Amelanotic melanomas:
Are relatively uncommon melanomas that occur without pigmentation changes
They are often more difficult to diagnose because of their lack of pigmentation
Factors such as:
Change in size
Asymmetry
Irregular borders may suggest malignancy and prompt a biopsy, but delays in diagnosis may sometimes be observed
While melanoma has been traditionally described using these categories:
Prognosis is more dependent upon staging than by these histomorphologic types
Boost radiation therapy is an additional dose of radiation delivered to the tumor bed after whole-breast irradiation (WBI) in patients who undergo breast-conserving surgery (BCS). The goal is to reduce local recurrence rates. The decision to give a boost is typically based on patient-specific risk factors.
Indications for Boost Radiation after BCS
1. Age < 50 years (especially < 40 years)
Data: The EORTC 22881–10882 trial (Bartelink et al., 2001; 2007 update) Population: 5,318 women with stage I/II breast cancer who received BCS + WBI (50 Gy) ± boost (16 Gy). Results: 10-year local recurrence (LR): Without boost: 10.2% With boost: 6.2% (Absolute reduction: 4%, p < 0.0001) Age stratification: < 40 years: LR reduced from 24% to 14% with boost (10% absolute benefit) 41–50 years: LR reduced from 11.7% to 6.4% (5.3% absolute benefit) 50 years: Less pronounced benefit
2. Positive or Close Surgical Margins
Rationale: Tumor cells may remain near the excision cavity, increasing recurrence risk. Guideline Support: NCCN recommends a boost for positive margins (even if re-excised) or if final margins are close, particularly in young patients.
3. High-Grade Tumors (Grade 3)
Data: High-grade tumors are more biologically aggressive and associated with higher LR rates. Boost helps reduce recurrence in these patients, especially when combined with other risk factors (young age, close margins).
4. Lymphovascular Invasion (LVI)
LVI is a marker for higher local and regional recurrence risk. While not an absolute indication, it adds weight to the decision in a patient with other risk factors.
5. Extensive Intraductal Component (EIC)
Especially in younger patients, an EIC increases the risk of residual disease and LR.
6. Triple-negative or HER2-positive subtypes (in younger patients)
While molecular subtype alone isn’t a formal indication for boost, aggressive biology may influence the decision when combined with other features (e.g., young age, LVI, close margins).
Guidelines
ASTRO 2016: Endorses boost in patients <50 years or with high-risk features. NCCN 2024: Recommends consideration of boost based on age, margin status, histology, grade, and LVI.
Clinical Takeaway
Boost radiation significantly reduces local recurrence in high-risk patients following breast-conserving surgery. The greatest benefit is seen in younger women and those with adverse pathological features.
Let me know if you’d like a one-slide summary for a presentation.
Varies according to the anatomical site as well as the size and shape of the lesion
Particular attention should be placed on the impact of the biopsy:
On definitive surgical treatment
Either an excisional biopsy or an incisional biopsy using a scalpel or punch is acceptable
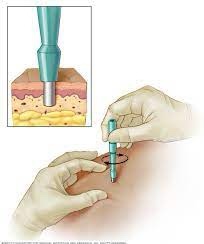
Punch biopsies can be performed for most lesions:
They should generally be performed at the most raised or darkest area of the lesion to sample the most aggressive area of the potential melanoma
Full-thickness biopsy into the subcutaneous tissue:
Should be performed to ensure accurate staging of the lesion
An excisional biopsy allows the pathologist to accurately determine the thickness of the lesion, since the entire lesion is available for evaluation:
Excisional biopsies should be performed when the lesion is too large for a punch:
But still can be removed without excessive surgical intervention
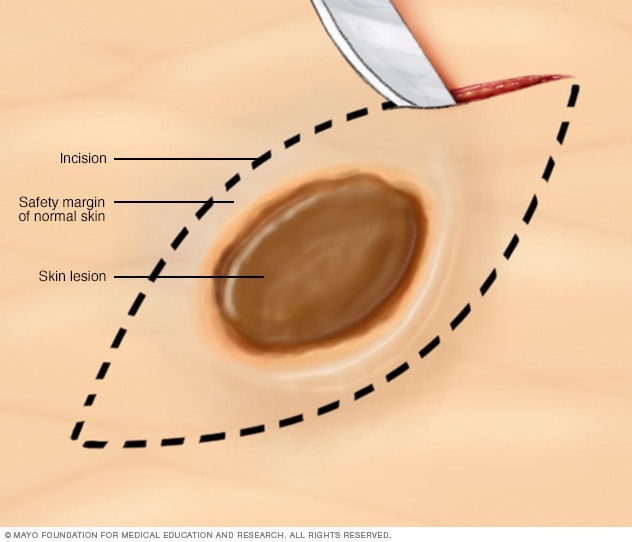
For excisional biopsies, a narrow margin of normal-appearing skin (1 to 2 mm) is generally taken with the specimen:
An elliptical incision is often used to facilitate closure
The biopsy incision should be oriented to facilitate later wide excision (e.g., axially on extremities) and minimize the need for a skin graft to provide wound closure at the time of wide excision
Shave biopsy:
Is generally discouraged if a diagnosis of melanoma is being considered since incomplete assessment of tumor thickness may result if the deep margin is not cleared
If a shave biopsy is performed, a deep shave /saucerization is preferable to obtain full-thickness biopsy of the suspect lesion
In general, I submit all pigmented lesions for permanent section examination and perform definitive surgery later
I generally prefer image-guided fine-needle aspiration or core biopsy as an initial diagnostic maneuver to document nodal or other melanoma metastases, but not to diagnose primary melanomas
Varies according to the anatomical site as well as the size and shape of the lesion
Particular attention should be placed on the impact of the biopsy on definitive surgical treatment
Either an excisional biopsy or an incisional biopsy using a scalpel or punch is acceptable
Entire removal of the lesion is generally preferred to allow for accurate pathologic evaluation
Punch biopsies:
Can be performed for most lesions:
Generally, they can be performed when lesions are located on areas where maximum preservation of surrounding skin is important, or can be completely excised with a punch
Punch biopsies:
Should be performed at the most raised or darkest area of the lesion to sample the most aggressive area of the potential melanoma
Full-thickness biopsy:
Into the subcutaneous tissue should be performed to ensure accurate staging of the lesion
An excisional biopsy:
Allows the pathologist to accurately determine the thickness of the lesion, since the entire lesion is available for evaluation
Excisional biopsies:
Should be performed when the lesion is too large for a punch but still can be removed without excessive surgical intervention
For excisional biopsies:
A narrow margin of normal-appearing skin (1 to 3 mm) is taken with the specimen
An elliptical incision:
Is often used to facilitate closure
The biopsy incision should be oriented to facilitate later wide excision (e.g., axially on extremities) and minimize the need for a skin graft to provide wound closure at the time of wide excision
Shave biopsy:
Is generally discouraged if a diagnosis of melanoma is being considered since incomplete assessment of tumor thickness may result if the deep margin is not cleared
If a shave biopsy is performed:
A deep shave is preferable
In general, I submit all pigmented lesions for permanent section examination and perform definitive surgery at a later time
I generally prefer image-guided fine-needle aspiration biopsy as an initial diagnostic maneuver to document nodal or other melanoma metastases:
Melanoma Epidemiology and Sun Exposure. Raimondi S, Suppa M, Gandini S. Acta Dermato-Venereologica. 2020;100(11):adv00136. doi:10.2340/00015555-3491. Melanoma. National Library of Medicine (MedlinePlus).
Is a pivotal phase III, multicenter, randomized controlled trial:
Designed to evaluate the safety and efficacy of narrower surgical margins:
For primary cutaneous melanomas that are stage T2b or higher
This trial specifically compares 1-cm margins with the standard 2-cm margins:
To determine if the narrower margin can provide equivalent outcomes in terms of local control and survival
The trial includes patients with primary melanomas thicker than 2 mm (T2b or higher):
It aims to assess whether a 1-cm margin can achieve similar rates of local recurrence, disease-free survival, and overall survival compared to the traditional 2-cm margin
The rationale for this study:
Is based on the hypothesis that narrower margins may reduce surgical morbidity and improve cosmetic outcomes without compromising oncologic safety
The MelMarT-II trial:
Is significant because it addresses the ongoing debate about the optimal surgical margin for thicker melanomas
Previous studies have established that a 2-cm margin is safe for melanomas thicker than 2 mm:
But the potential benefits of a 1-cm margin in terms of reduced morbidity and improved quality of life warrant further investigation
In addition to the classical descriptions of melanomas:
The ability to perform molecular profiling on tumors has added to our understanding of this complex and often heterogeneous disease
Although currently not generally reported as part of the primary staging of melanoma:
Genetic profiling has been widely employed in advanced disease:
With advances in technology, mutational analysis is routinely performed from formalin-fixed paraffin-embedded archival tissue
This has led to new insights into the pathogenesis of this disease as well as actionable treatment strategies against specific molecular aberrations:
Especially in the setting of unresectable and advanced disease
Recent studies demonstrate that most melanomas have one or more mutations in essential kinase signaling pathways
Important in melanoma is the:
RAS-RAF-MEK-ERK kinase-signaling pathway
Studies have consistently found that 40% to 50% of cutaneous melanomas (particularly superficial spreading melanoma):
Harbor mutations in a particular member of the RAF family known as BRAF
Although multiple BRAF mutations have been identified:
Approximately 90% consist of a point mutation at V600E:
That leads to an approximately 400-fold increase in the activity of the BRAF protein
Interestingly, 70% to 80% of benign nevi also harbor BRAF mutations:
Suggesting that genetic alterations alone cannot fully explain the aggressive biology of melanoma
In the same kinase pathway, approximately 15% to 26% of melanomas:
Are found to have an activating NRAS mutation
A comprehensive molecular analysis of cutaneous melanoma by The Cancer Genome Atlas (TCGA) melanoma project has provided new insights into the roles and frequency of mutated cancer genes and other genomic signatures
These findings helped to establish that cutaneous melanoma can be grouped into one of four subtypes:
BRAF mutant (most common)
RAS mutant
NF1 mutant
Triple-WT (wild type)
Interestingly, BRAF and NRAS mutations:
Are rarely identified simultaneously in the same melanoma tumor
The phosphatase and tensin homolog (PTEN) protein is widely expressed throughout the human body:
PTEN acts as a phosphatase to dephosphorylate phosphatidylinositol (3,4,5)-trisphosphate
The PI3 kinase-AKT pathway:
Is the most common kinase pathway mutated in cancer
PTEN inhibits the activation of AKT:
Therefore, loss of PTEN results:
In the constitutive activation of the AKT pathway
Often, PTEN loss is found concurrently with NRAS mutations
Mutations in AKT have also been identified in melanoma
While MAP kinase signaling pathway mutations:
Have been commonly found in cutaneous melanomas:
Arising in sun-exposed areas:
They are infrequent in mucosal and acral lentiginous melanomas
A missense mutation in the c-KIT gene:
Has been found in more than 20% of mucosal melanomas and more than 10% of acral lentiginous melanomas
The increasing incidence rates of cutaneous melanoma in the United States projected for 2025 are influenced by several key risk factors:
With ultraviolet (UV) exposure and demographic changes playing significant roles
Ultraviolet (UV) Exposure:
UV radiation from sunlight and artificial sources like tanning beds is the primary risk factor for melanoma
Both intermittent intense exposure (e.g., sunburns) and chronic cumulative exposure contribute to melanoma risk
The American Cancer Society emphasizes that reducing UV exposure through protective measures such as:
Sunscreen use, wearing protective clothing, and avoiding tanning beds can mitigate this risk
Demographic Factors:
Skin Type:
Individuals with fair skin, light hair, and light eye color are at higher risk:
Due to lower melanin levels:
Which provide less natural protection against UV radiation
Age:
Melanoma incidence increases with age, particularly in older adults:
Due to cumulative UV exposure over a lifetime
However, it is also common in younger adults, especially women:
Likely due to higher use of tanning beds and intentional sun exposure
Gender:
Men have higher melanoma incidence rates than women, particularly after age 40:
This may be due to differences in sun exposure behaviors and lower rates of skin self-examination among men
Genetic Factors:
A family history of melanoma increases risk, as does the presence of numerous or atypical nevi (moles)
Genetic predispositions, such as mutations in the CDKN2A gene:
Also contribute to higher melanoma risk
Other Factors:
Immunosuppression, whether due to medical conditions like HIV or medications post-organ transplantation:
Increases melanoma risk
Additionally, socioeconomic factors, such as higher income and access to dermatologic care, can lead to higher diagnosis rates due to increased diagnostic scrutiny
In summary, the rising incidence of cutaneous melanoma in the United States is driven by UV exposure, demographic changes, genetic predispositions, and other factors:
Effective prevention strategies focusing on reducing UV exposure and early detection are crucial to managing this growing public health concern
References:
Cutaneous Melanoma. Long GV, Swetter SM, Menzies AM, Gershenwald JE, Scolyer RA. Lancet (London, England). 2023;402(10400):485-502. doi:10.1016/S0140-6736(23)00821-8.
Epidemiology of Skin Cancer: Update 2019. Leiter U, Keim U, Garbe C. Advances in Experimental Medicine and Biology. 2020;1268:123-139. doi:10.1007/978-3-030-46227-7_6.