- The KEYNOTE-716 trial:
- Was a randomized, double-blind, phase 3 study:
- Evaluating adjuvant pembrolizumab (200 mg IV every 3 weeks for up to 1 year) versus placebo:
- In patients aged ≥ 12 years with completely resected, high-risk stage IIB or IIC cutaneous melanoma (T3b / T4, node-negative)
- The primary endpoint was:
- Recurrence-free survival (RFS)
- Secondary endpoints:
- Distant metastasis-free survival (DMFS)
- Safety
- Evaluating adjuvant pembrolizumab (200 mg IV every 3 weeks for up to 1 year) versus placebo:
- Patients with recurrence after placebo could cross over to pembrolizumab
- Was a randomized, double-blind, phase 3 study:
- Key findings:
- Pembrolizumab significantly reduced the risk of recurrence or death compared to placebo
- At a median follow-up of 39.4 months, the hazard ratio for RFS was:
- 0.62 (95% CI, 0.49–0.79)
- The estimated 36-month RFS was 76.2% for pembrolizumab vs 63.4% for placebo
- DMFS was also improved:
- 36-month DMFS:
- 84.4% vs 74.7%; HR 0.59, 95% CI 0.44–0.79
- 36-month DMFS:
- The benefit was consistent across subgroups:
- Including tumor location and histopathologic features
- Grade ≥ 3 treatment-related adverse events occurred in 16% of pembrolizumab-treated patients, with no new safety signals on long-term follow-up
- Overall survival data remain immature, and immune-related toxicity remains a consideration
- Clinical implications:
- The KEYNOTE-716 trial established adjuvant pembrolizumab as a standard of care for resected stage IIB / IIC melanoma:
- Extending the benefit of immune checkpoint blockade to node-negative, high-risk stage II disease
- The American Society of Clinical Oncology now recommends:
- Adjuvant pembrolizumab for these patients, with the caveat that the risk of immune-related toxicity must be weighed against the lack of mature overall survival data
- Adjuvant pembrolizumab for these patients, with the caveat that the risk of immune-related toxicity must be weighed against the lack of mature overall survival data
- The KEYNOTE-716 trial established adjuvant pembrolizumab as a standard of care for resected stage IIB / IIC melanoma:
- In context, KEYNOTE-716 complements prior major adjuvant trials:
- EORTC 18071:
- Ipilimumab vs placebo, stage III:
- Improved RFS / OS but high toxicity
- Ipilimumab vs placebo, stage III:
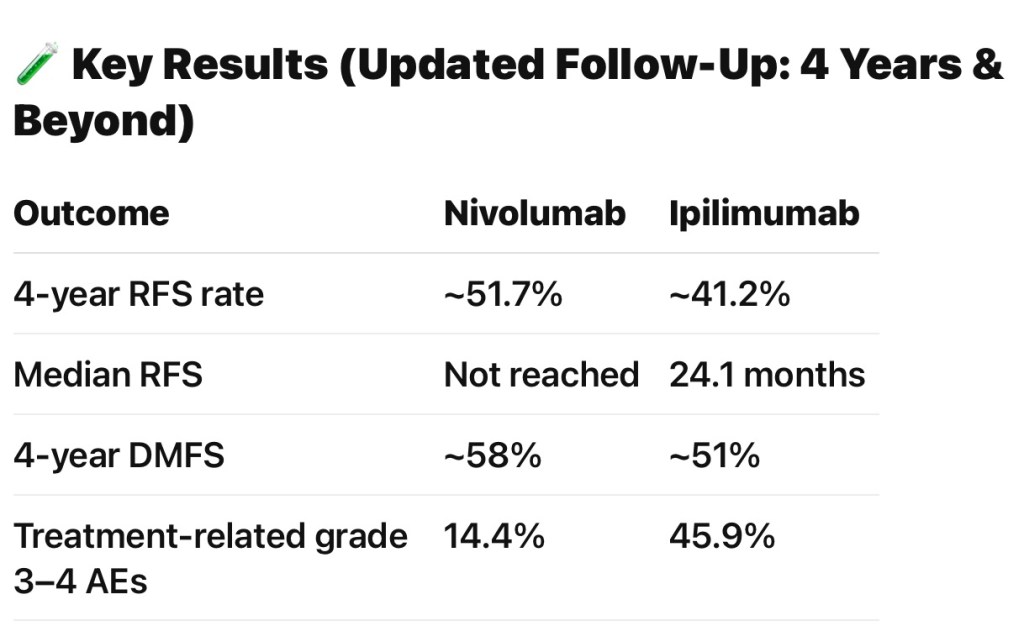
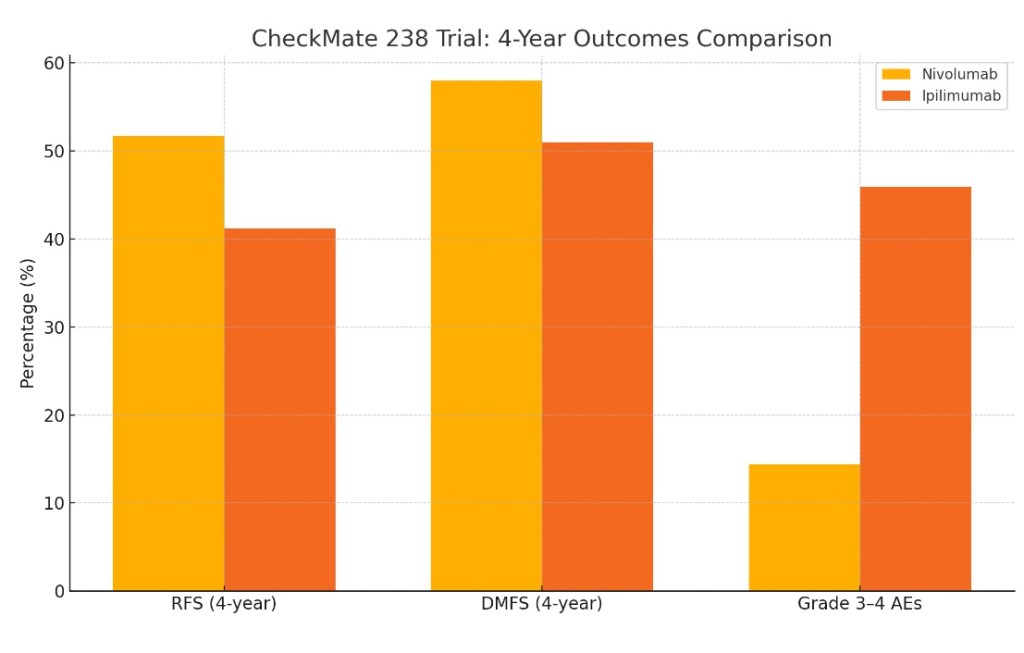
- CheckMate 238:
- Nivolumab vs ipilimumab, stage III / IV):
- Superior RFS and safety for nivolumab
- Nivolumab vs ipilimumab, stage III / IV):
- KEYNOTE-054:
- Pembrolizumab vs placebo, stage III:
- improved RFS / DMFS with favorable safety
- Pembrolizumab vs placebo, stage III:
- KEYNOTE-716:
- Is the first to show a significant benefit for adjuvant anti–PD-1 therapy in stage II melanoma:
- Expanding the population eligible for effective adjuvant immunotherapy
- Is the first to show a significant benefit for adjuvant anti–PD-1 therapy in stage II melanoma:
- EORTC 18071:
- References:
- Pembrolizumab Versus Placebo as Adjuvant Therapy in Completely Resected Stage IIB or IIC Melanoma (KEYNOTE-716): A Randomised, Double-Blind, Phase 3 Trial. Luke JJ, Rutkowski P, Queirolo P, et al. Lancet (London, England). 2022;399(10336):1718-1729. doi:10.1016/S0140-6736(22)00562-1.
- Pembrolizumab Versus Placebo as Adjuvant Therapy in Resected Stage IIB or IIC Melanoma (KEYNOTE-716): Distant Metastasis-Free Survival Results of a Multicentre, Double-Blind, Randomised, Phase 3 Trial. Long GV, Luke JJ, Khattak MA, et al. The Lancet. Oncology. 2022;23(11):1378-1388. doi:10.1016/S1470-2045(22)00559-9.
- Pembrolizumab Versus Placebo as Adjuvant Therapy in Resected Stage IIB or IIC Melanoma: Final Analysis of Distant Metastasis-Free Survival in the Phase III KEYNOTE-716 Study. Luke JJ, Ascierto PA, Khattak MA, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2024;42(14):1619-1624. doi:10.1200/JCO.23.02355.
- Pembrolizumab Versus Placebo as Adjuvant Therapy in Resected Stage IIB or IIC Melanoma: Long-Term Follow-Up, Crossover, and Rechallenge With Pembrolizumab in the Phase III KEYNOTE-716 Study. Luke JJ, Ascierto PA, Khattak MA, et al. European Journal of Cancer (Oxford, England : 1990). 2025;220:115381. doi:10.1016/j.ejca.2025.115381.
- Systemic Therapy for Melanoma: ASCO Guideline Update. Seth R, Agarwala SS, Messersmith H, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2023;41(30):4794-4820. doi:10.1200/JCO.23.01136.
- Adjuvant Pembrolizumab in Stage II Melanoma: Outcomes by Primary Tumor Location in the Randomized, Double-Blind, Phase III KEYNOTE-716 Trial. Yoon CH, Ross MI, Gastman BR, et al. Annals of Surgical Oncology. 2025;32(4):2756-2764. doi:10.1245/s10434-024-16642-6.
- Pembrolizumab Versus Placebo as Adjuvant Therapy in Resected Stage IIB or IIC Melanoma: Outcomes in Histopathologic Subgroups From the Randomized, Double-Blind, Phase 3 KEYNOTE-716 Trial. Schadendorf D, Luke JJ, Ascierto PA, et al. Journal for Immunotherapy of Cancer. 2024;12(3):e007501. doi:10.1136/jitc-2023-007501.