My name is Rodrigo Arrangoiz I am a breast surgeon/ thyroid surgeon / parathyroid surgeon / head and neck surgeon / surgical oncologist that works at Center for Advanced Surgical Oncology in Miami, Florida.
I was trained as a surgeon at Michigan State University from (2005 to 2010) where I was a chief resident in 2010. My surgical oncology and head and neck training was performed at the Fox Chase Cancer Center in Philadelphia from 2010 to 2012. At the same time I underwent a masters in science (Clinical research for health professionals) at the University of Drexel. Through the International Federation of Head and Neck Societies / Memorial Sloan Kettering Cancer Center I performed a two year head and neck surgery and oncology / endocrine fellowship that ended in 2016.
Mi nombre es Rodrigo Arrangoiz, soy cirujano oncólogo / cirujano de tumores de cabeza y cuello / cirujano endocrino que trabaja Center for Advanced Surgical Oncology en Miami, Florida.
Fui entrenado como cirujano en Michigan State University (2005 a 2010 ) donde fui jefe de residentes en 2010. Mi formación en oncología quirúrgica y e n tumores de cabeza y cuello se realizó en el Fox Chase Cancer Center en Filadelfia de 2010 a 2012. Al mismo tiempo, me sometí a una maestría en ciencias (investigación clínica para profesionales de la salud) en la Universidad de Drexel. A través de la Federación Internacional de Sociedades de Cabeza y Cuello / Memorial Sloan Kettering Cancer Center realicé una sub especialidad en cirugía de cabeza y cuello / cirugia endocrina de dos años que terminó en 2016.
Is recommended for most ADH lesions diagnosed on core needle breast biopsy (CNB)
The chance of upgrade at excision to ductal carcinoma in situ (DCIS) or invasive carcinoma:
Is generally in the 12% to 22% range in the literature
The need for routine excision of pure flat epithelial atypia (FEA) has been less clear:
Some authors have reported an upgrade rate of 9.6% following excision of lesions that show pure FEA without ADH when the vast majority of biopsies were done with a 14-gauge spring-loaded core biopsy device
It is not clear that biopsy with a vacuum-assisted device would yield the same results
In fact, in one study reporting biopsy of low-risk calcifications with a vacuum-assisted device, pure FEA never resulted in an upgrade to malignancy
An article from the Mayo Clinic showed that FEA does not seem to convey an independent risk of breast cancer beyond that of associated proliferative disease without atypia or associated ADH
The risk of upgrade at surgical excision for ADH:
Has been reported to correlate with the number of ducts or terminal duct lobular units involved on vacuum-assisted core biopsy;
With 2 or fewer foci of involvement:
There was no upgrade on excision
With 4 or more foci of involvement:
There was a strong probability of upgrade to ductal carcinoma in situ or invasive carcinoma at excision
Work continues to try to define a low-risk group who could potentially avoid excisional biopsy:
Particularly those with small areas of calcifications completely removed with core needle biopsy and only focal ADH on pathology
Apocrine metaplasia, florid epithelial hyperplasia of the usual variety, and columnar cell change without atypia:
Do not confer a significant risk of upgrade and do not require excision
References
Eby PR, Ochsner JE, DeMartini WB, Allison KH, Peacock S, Lehman CD. Is surgical excision necessary for focal atypical ductal hyperplasia found at stereotactic vacuum-assisted breast biopsy? Ann Surg Oncol. 2008;15(11):3232-3238.
Ely KA, Carter BA, Jensen RA, Simpson JF, Page DL. Core biopsy of the breast with atypical ductal hyperplasia: a probabilistic approach to reporting. Am J Surg Pathol. 2001;25(8):1017-1021.
Khoumais NA, Scaranelo AM, Moshonov H, Kulkarni SR, Miller N, McCready DR, et al. Incidence of breast cancer in patients with pure flat epithelial atypia diagnosed at core-needle biopsy of the breast. Ann Surg Oncol. 2013;20(1):133-138.
Said SM, Visscher DW, Nassar A, Frank RD, Vierkant RA, Frost MH, et al. Flat epithelial atypia and risk of breast cancer: a Mayo cohort study. Cancer. 2015;121(10):1548-1555.
McGhan LJ, Pockaj BA, Wasif N, Giurescu ME, McCullough AE, Gray RJ. Atypical ductal hyperplasia on core biopsy: an automatic trigger for excisional biopsy? Ann Surg Oncol. 2012;19(10):3264-3269.
Mitochondrial DNA mutations described (consistent with oncocytic phenotype)
Increasing evidence suggests WT may represent a tumor-like reactive process rather than a true neoplasm
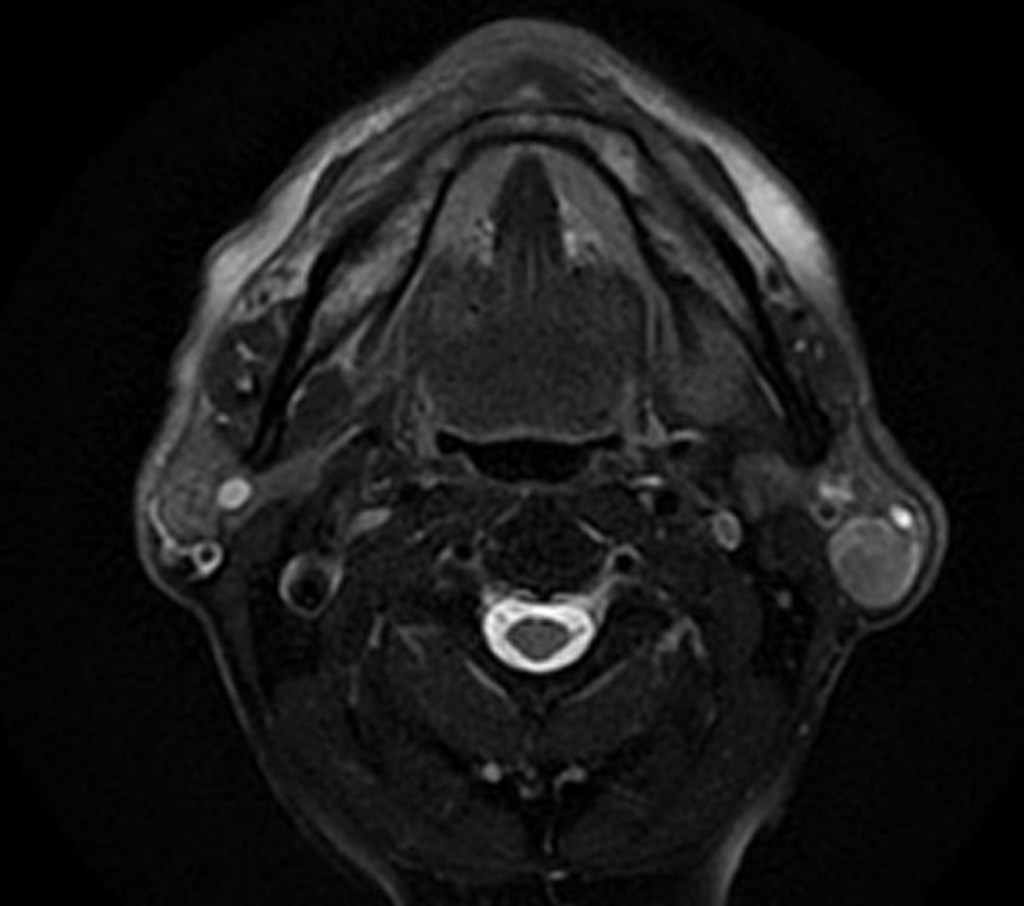
Clinical Presentation:
Painless, slow-growing preauricular or infra-auricular mass
Often fluctuant due to cystic nature
Facial nerve dysfunction is exceptional and should raise concern for alternative diagnoses
Bilateral or synchronous contralateral lesions strongly suggest WT
Imaging Characteristics (supportive, not diagnostic):
Ultrasound:
Well-defined, hypoechoic, often cystic with internal septations
CT:
Well-circumscribed, cystic or cystic-solid lesion, tail of parotid
MRI:
T1: low–intermediate signal
T2: heterogeneous, often high signal
Characteristically shows high uptake on Tc-99m pertechnetate scans (classic but rarely used today)
Diagnosis:
Fine-needle aspiration (FNA) is usually sufficient:
Typical findings:
Oncocytic epithelial cells + lymphoid background
Diagnostic accuracy is high when classic features are present
Core needle biopsy rarely needed
Important to correlate with imaging and clinical setting (older smoker, tail of parotid)
Management:
Observation:
Appropriate in selected patients when:
Diagnosis is secure:
Concordant clinical + imaging + FNA
Asymptomatic or minimally symptomatic
No cosmetic concern
No facial nerve dysfunction
Patient preference supports surveillance
Rationale:
Benign behavior
Very low malignant transformation risk
Many tumors grow minimally or plateau
Surgical Management:
Indications:
Diagnostic uncertainty
Symptomatic tumor:
Pain, rapid growth, infection
Cosmetic deformity
Patient anxiety or preference
Very large lesions
Surgical options:
Partial superficial parotidectomy
Extracapsular dissection (ECD) in well-selected cases
Facial nerve preservation is standard
Total parotidectomy rarely required
Neck dissection:
Not indicated
Adjuvant therapy:
None
Prognosis:
Excellent
Recurrence is uncommon and usually reflects:
Multifocal disease
Development of a new metachronous WT
Long-term survival equivalent to general population
Key Teaching Points for Surgeons:
Tail of parotid + smoker + cystic mass = think Warthin
Bilaterality strongly favors WT
Observation is acceptable and evidence-based in selected patients
Avoid overtreatment:
Facial nerve morbidity must be weighed against benign biology
Key References:
Barnes L, Eveson JW, Reichart P, Sidransky D. WHO Classification of Tumours of the Head and Neck. IARC Press; 2017 / 2022 (5th ed.).
Ellis GL, Auclair PL. Tumors of the Salivary Glands. AFIP Atlas of Tumor Pathology. Seifert G, Donath K. The Warthin tumor: a multifocal disease. Virchows Arch A Pathol Anat Histopathol. 1996.
Eveson JW, Cawson RA. Warthin’s tumour (cystadenolymphoma) of salivary glands: a study of 78 cases. Oral Surg Oral Med Oral Pathol.
Schwalje AT, Uzelac A, Ryan WR. Growth rate characteristics of Warthin tumors. Otolaryngol Head Neck Surg. 2015.
Quer M, et al. ESMO–EURACAN Clinical Practice Guidelines for salivary gland cancer. Ann Oncol. 2022.
Witt RL, et al. Observation of Warthin tumors: a safe alternative to surgery. Otolaryngol Head Neck Surg.
Comprising multiple biological entities, each with distinct pathology, features, and clinical implications
Gene expression profiling in breast cancer has identified four or five main molecular subtypes of breast cancer recognized as distinct biological entities:
Luminal A subtype:
ER positive [ER], progesterone receptor [PR] positive and HER-2 negative with low Ki-67 [< 14%]
Luminal B subtype:
ER positive, PR positive, and HER-2 negative with high Ki-67 [> 14%]
Basal-like / triple-negative subtype:
ER negative, PR negative, and HER-2 negative
HER-2-amplified subtype:
Which can be further divided by ER status into:
ER negative, HER-2 positive
ER positive, HER-2 positive
Classifying breast cancer into these subtypes has led to a paradigm shift in how patients are currently stratified and treated
Arterial Anatomy of the Breast – A Practical Summary for Breast Surgeons
Understanding the arterial supply of the breast is essential for:
Oncologic resections
Reconstructive planning
Oncoplastic surgery
Complication avoidance
The breast receives a rich, redundant blood supply primarily from branches of the:
Subclavian and axillary arterial systems:
Which explains its generally good healing capacity:
But also the risk of bleeding if anatomy is not respected
Primary Arterial Sources:
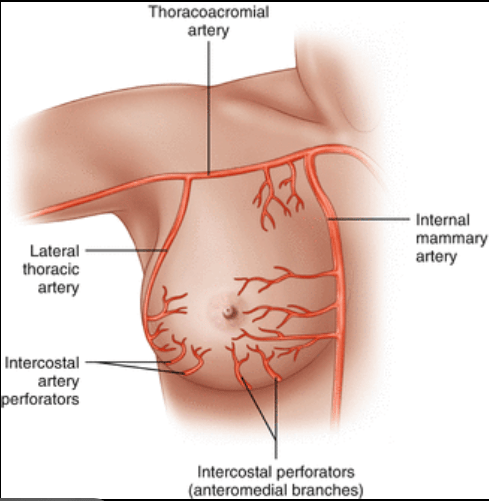
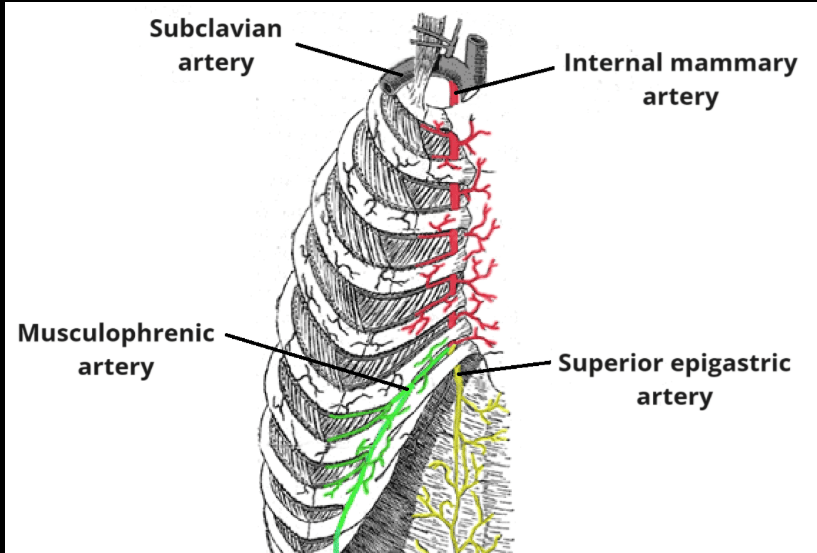
Internal Mammary (Internal Thoracic) Artery:
Most important medial blood supply to the breast
Arises from the:
Subclavian artery
Gives rise to anterior intercostal perforators, especially:
2nd to 4th intercostal perforators:
Dominant contributors
Supplies:
Medial breast
Retroareolar complex
Key surgical relevance:
Critical during medial lumpectomies
Important for nipple-areolar complex (NAC) viability
Used as recipient vessels in free flap breast reconstruction
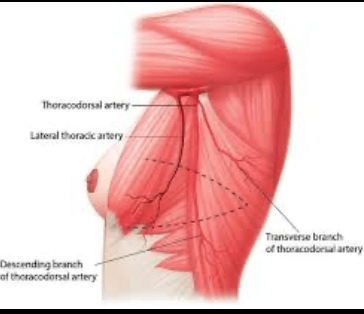
Lateral Thoracic Artery:
Branch of the axillary artery
Runs along the lateral chest wall
Supplies:
Lateral breast
Skin and glandular tissue
Key surgical relevance:
At risk during axillary dissection
Important contributor in lateral oncoplastic flaps
Thoracoacromial Artery (Pectoral Branch):
Branch of the axillary artery Supplies:
Upper outer quadrant
Pectoralis major muscle
Key surgical relevance:
Important during subpectoral dissection:
Preservation helps reduce skin flap ischemia
Posterior Intercostal Arteries:
Arise directly from the thoracic aorta
Provide deep perforating branches
Supply:
Deep parenchyma
Chest wall interface
Key surgical relevance:
Contribute to deep tissue perfusion
Source of bleeding during deep resections
Perforator System and Anastomoses:
The breast has an extensive subdermal and intraparenchymal anastomotic network
Major perforators:
Medial (internal mammary)
Lateral (lateral thoracic)
Clinical implications:
Explains tolerance of wide local excisions
Allows for oncoplastic rearrangements
Supports skin- and nipple-sparing mastectomy when flaps are well designed
Surgical Implications for Breast Surgeons:
Breast-Conserving Surgery:
Medial tumors:
Respect internal mammary perforators
Lateral tumors:
Anticipate supply from lateral thoracic artery
Mastectomy (Skin- or Nipple-Sparing):
Preserve:
Subdermal plexus
Medial perforators
Excessive cautery near the NAC increases ischemia risk
Oncoplastic Surgery:
Knowledge of arterial territories guides:
Pedicle choice
Flap orientation
Central and medial pedicles rely heavily on internal mammary perforators
Reconstruction:
Internal mammary vessels are preferred recipient vessels for free flaps
Axillary system preservation is important in implant-based reconstruction
Key Take-Home Points:
Breast arterial supply is dual and redundant, centered on:
Internal mammary system (medial dominance)
Axillary system (lateral dominance)
2nd to 4th internal mammary perforators are the most critical vessels
Surgical planning should always consider vascular territories, especially in:
Re-operations
Radiation-treated breasts
Large resections or complex oncoplastic cases
References:
Arterial Anatomy of the Breast
Cunningham L.The anatomy of the arteries and veins of the breast. J Surg Oncol. 1977;9(1):71–85. → Classic anatomic description of breast vascular supply.
Salmon RJ. Vascularization of the breast and implications for surgery. Surg Clin North Am. 1990;70(4):877–885. → Foundational surgical anatomy review.
Hall-Findlay EJ. Breast anatomy and vascular supply. Clin Plast Surg. 2002;29(3):371–384. → Highly cited reference for oncoplastic and reconstructive surgery.
Sappey M.Traité d’Anatomie Descriptive. Paris: Delahaye; 1874. → Early detailed descriptions of breast perforators (historical reference).
Taylor GI, Palmer JH. The vascular territories (angiosomes) of the body. Br J Plast Surg. 1987;40(2):113–141. → Angiosome concept applied to breast perfusion and flap design.
Internal Mammary & Perforator Anatomy:
Cormack GC, Lamberty BG. The arterial anatomy of skin flaps. Edinburgh: Churchill Livingstone; 1994. → Describes internal mammary perforators relevant to breast surgery.
Saint-Cyr M, Wong C, Schaverien M, et al. Perforator flaps: anatomy, technique, and clinical applications. Plast Reconstr Surg. 2009;124(1 Suppl):e1–e17. → Detailed perforator anatomy with relevance to NAC perfusion.
Hamdi M, Van Landuyt K, Monstrey S, Blondeel P. Pedicled perforator flaps in breast reconstruction. Semin Plast Surg. 2006;20(2):73–83.
Surgical & Oncoplastic Relevance:
Losken A, Hamdi M. Partial breast reconstruction: current perspectives. Plast Reconstr Surg. 2009;124(3):722–736. → Links vascular anatomy to oncoplastic pedicle choice.
Clough KB, Kaufman GJ, Nos C, Buccimazza I, Sarfati IM. Improving breast cancer surgery: a classification and quadrant-based approach. Plast Reconstr Surg. 2010;125(2):418–428.
Mast BA. Breast reduction and mastopexy: pedicle selection and vascular considerations. Clin Plast Surg. 1996;23(3):567–576.
Nipple–Areolar Complex (NAC) Perfusion
van Deventer PV, Graewe FR. Blood supply of the nipple–areolar complex. Plast Reconstr Surg. 1984;74(4):499–504.
Russo V, Della Corte A, et al. Nipple–areola complex vascular anatomy and surgical implications. Aesthetic Plast Surg. 2017;41(2):267–274.
Reconstruction-Focused References:
Blondeel PN, Morris SF, Hallock GG, Neligan PC.Perforator Flaps: Anatomy, Technique, and Clinical Applications. St. Louis: Quality Medical Publishing; 2006.
Nahabedian MY. Breast reconstruction and internal mammary vessels. Plast Reconstr Surg. 2012;130(4):883–891.
Is a proliferative epithelial lesion of the terminal ductal lobular unit:
That typically demonstrates low-grade cytologic atypia and monomorphism combined with epithelial architectural complexity (i.e., cribriforming)
Histologically:
ADH and low-grade DCIS are virtually identical:
The distinction between them is based primarily on:
The quantity of atypia present
Currently, the consensus criteria recommend that a diagnosis of DCIS be reserved for:
Lesions that circumferentially involve two or more membrane-bound spaces (typically ducts) or that measure more than 2 mm in linear extent
A diagnosis of ADH is rendered for:
Morphologically identical lesions that fall short of these quantitative criteria
Atypical ductal hyperplasia (ADH):
Is identified in:
8% to 17% of all core needle breast biopsy specimens
Because the distinction between ADH and DCIS relies on the quantity of atypia:
Sampling is an important concern for ADH diagnosed on CNB
Multiple studies of upgrade rates for excision of ADH on CNB, including recent studies with primarily large core biopsy techniques:
Show persistent upgrade rates of 10% to 30%:
Leading to a recommendation for excision as the standard of care
Surgical excision remains the standard of care after a core biopsy diagnosis of ADH:
However, given that the majority of ADH cases diagnosed by percutaneous biopsy are not upgraded to cancer:
Routine excision may represent overtreatment
Therefore, as has been done for other high- risk lesions identified on CNB, recent research efforts have attempted to identify factors associated with a low risk of cancer upgrade in order to define a favorable subgroup of women who may avoid surgical excision with minimal risk of a missed invasive carcinoma
Several groups have worked to identify features of women with ADH on CNB who have a very low risk (5%) of upgrade to cancer:
Nguyen et al. previously published criteria by which ADH lesions found on core biopsy could be triaged according to the risk of upgrade to an associated carcinoma:
In their series of 140 patients, a number of factors were significantly correlated with the rate of upgrade to carcinoma including:
Removal of less than 95% of calcifications in the absence of an associated mass
Involvement of two or more terminal duct-lobular units
The presence of significant cytologic atypia
The presence of necrosis
Use of these combined criteria led to:
An upgrade rate of 3% for the subset of women with low-risk features
Ko et al, also developed a scoring system to predict malignancy in patients with a diagnosis of ADH on CNB:
They found that age older than 50 year, micro-calcification on mammography, size on imaging greater than 15 mm, and a palpable lesion were independent predictors of malignancy
The presence of focal ADH was a negative predictor
Similar criteria also have been reported by Pena et al. from the Mayo Clinic:
In this series of 399 patients, the overall upgrade rate was:
16.1%
The features on core biopsy most strongly associated with upgrade were:
Percentage of the lesion removed
Individual cell necrosis
Number of ADH foci in the core biopsy specimen
A low-risk subgroup was identified by:
The absence of individual cell necrosis
Either one focus of ADH with 50% removal or more / or more than one focus with 90% removal of the sample
Using these criteria, approximately one third of women were identified as low risk for upgrade, and the actual upgrade rate in this group was 4.9%
Individual cell necrosis:
Also has been suggested by prior studies showing its association with cancer upgrade
Pena et al. also evaluated the performance of the Ko et al. and Nguyen et al. criteria and found that both models successfully identified women with a low risk of upgrade:
However the proportion of women assessed to be at low risk was substantially smaller than with the Pena model
The long-term safety of prospectively omitting surgical excision was recently reported by Menen et al. for the low-risk subgroup of women defined by the criteria of Nguyen et al:
In this series of 175 patients, all meeting the low-risk criteria, 125 were observed, and 50 underwent excision
During a median follow-up period of 3 years, 14 breast cancer events were noted:
In the surgery group, breast cancer developed in six women (12%), compared with seven cancers (5.6%) in the observed group
Notably, approximately 75% of the cancer events occurred in the ipsilateral breast, and the majority were outside the index site
These data suggest that observation rather than surgical excision after a core biopsy diagnosis of ADH may be a safe option for a select subgroup of patients meeting the low-risk radiologic and histologic criteria:
However, close monitoring and the use of chemoprevention still are indicated because ADH is a marker of increased risk for breast carcinoma
Caution with omitting surgical excision is further highlighted by the results reported by Deshaies et al:
In their large retrospective study of 422 ADH cases, the following six factors independently associated with cancer upgrade were identified:
Severe ADH
Mammography for ipsilateral symptoms
Mammographic lesions other than microcalcifications alone
Co-diagnosis of papilloma
Use of a 14-gauge needle
ADH diagnosis performed by pathologists with low volume
Of the 422 biopsies, 128 were judged to be low risk because they did not present any of these six characteristics, yet the upgrade frequency at surgery was substantial (17.2 vs 31.3% for the whole group):
Thus, these authors were unable to identify a subgroup of patients for whom excision could confidently be omitted with a low risk of upgrade
Notably, this study did not include the proportion of the lesion removed with needle biopsy, which appeared to be a key factor in the other aforementioned models that succeeded in identifying a low-risk subgroup
Despite recent research efforts to identify a low-risks group:
Surgical excision remains the standard of care after a CNB diagnosis of ADH:
Particularly in the presence of an associated mass lesion and radiologic-pathologic discordance
Although promising, the vast majority of these data have been in retrospective studies, with only one single-institution prospective study investigating a limited number of women:
Therefore, the standard approach remains surgical excision until further prospective studies confirm the validity of these criteria
For women with ADH diagnosed by CNB, surgical excision is not the only relevant clinical decision in patient management:
For these women, estimation of their long- term breast cancer risk is important so they can be advised on surveillance and prevention strategies
Unfortunately, commonly used breast cancer risk models, such as the Gail model and the Tyrer-Cuzick model:
Do not predict risk very accurately for individual women with atypical hyperplasia
For this reason, absolute risk estimation is recommended:
Based on data from the Mayo Clinic and Nashville Cohorts:
The risk is approximately 1% per year for women with ADH
The Partners Cohort has found a somewhat higher risk:
Approximately 1.7% per year, for women with ADH
In contrast, recent data from the Breast Cancer Surveillance Consortium found a lower annual average risk of breast cancer for women with ADH:
Only 0.6% per year, although these data included only invasive breast cancer events and excluded DCIS
Further work is ongoing to optimize accurate risk assessment for women with ADH
Another factor shown to stratify long-term risk for women with ADH is the number of ADH foci present within the benign breast biopsy specimen:
With increasing risk related to increasing foci of atypia, observed in both the Mayo Clinic and the Nashville Cohorts
This finding was challenged by the Nurses’ Health Study, in which the number of ADH foci did not have a significant impact later on breast cancer risk
Risk estimation is relevant because a lifetime risk greater than 25% would indicate use of magnetic resonance imaging (MRI) for breast cancer screening, whereas risk below that threshold would not
Regardless of the means used to estimate long-term breast cancer risk for women with ADH, prevention therapy should be discussed:
For younger women with an anticipated long life expectancy and a long at-risk period for breast cancer:
Prevention therapy should be strongly recommended because their cumulative risk probably exceeds 25%
For older women with competing morbidity, prevention therapy is unlikely to have any impact on survival and minimal benefit for quality of life because most breast cancers that would develop are likely to be hormonally sensitive:
However, prevention therapy should be recommended for the majority of women with ADH because their long-term risk is substantial, and prevention medications result in a 70% reduction in breast cancer risk
Long-term counseling of women with ADH should include some discussion of long-term breast cancer risk, surveillance strategies, and options for prevention therapy
How Common Is Thyroid Cancer? (Putting Risk in Perspective)
Hearing the word cancer is frightening—but it’s important to understand the actual risk.
📊 How common is thyroid cancer?
Thyroid cancer accounts for ~1–2% of all cancers Although diagnoses have increased (largely due to better imaging), most thyroid cancers are low-risk Survival rates are excellent, especially when detected early
🧠 What does this mean for patients?
Only 5–10% of thyroid nodules are cancer The most common type, papillary thyroid cancer, has a >95% long-term survival Many patients can be treated with limited surgery or even active surveillance
🔍 Why are we diagnosing more thyroid cancer?
Widespread use of high-resolution ultrasound Detection of small, clinically indolent tumors ➡️ This is why risk stratification and thoughtful management are critical—to avoid overtreatment.
🦋 The big picture
Thyroid cancer is:
✔️ Commonly curable
✔️ Often slow-growing
✔️ Best managed with individualized, evidence-based care
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
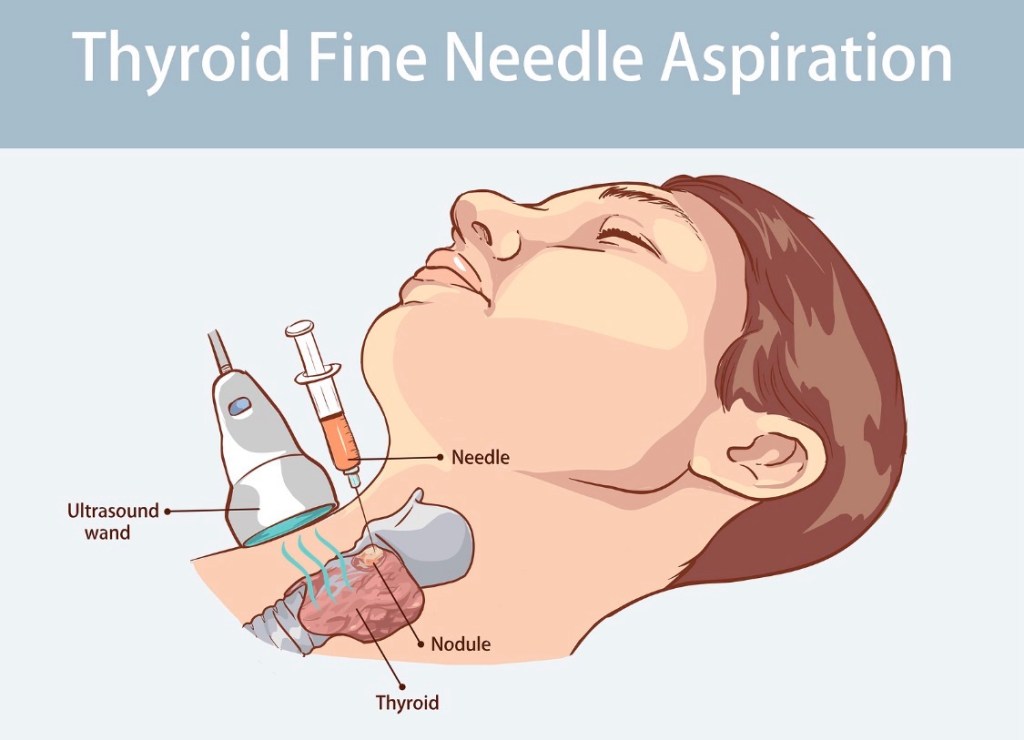
What Is a Thyroid Fine-Needle Aspiration (FNA) Biopsy?
A thyroid FNA biopsy is the standard, evidence-based test used to determine whether a thyroid nodule is benign or malignant—and it is far simpler than most patients expect.
🧪 How is the biopsy performed? (Step-by-step)
Ultrasound guidance precisely targets the nodule A very thin needle is used to collect cells Multiple passes may be taken to ensure accuracy The procedure takes 5–10 minutes You go home the same day and resume normal activities
✔️ No general anesthesia
✔️ Minimal discomfort
✔️ Very low risk of complications
🔬 What happens to the sample?
The cells are analyzed by an experienced cytopathologist and reported using the Bethesda System, which helps guide:
Observation Repeat biopsy Molecular testing (when appropriate) Surgery (only when necessary)
📊 Key facts for patients
Most biopsies come back benign FNA prevents unnecessary thyroid surgery Results allow for personalized, evidence-based care
🦋 Why this matters
A properly performed, ultrasound-guided FNA is:
Accurate Safe Essential for making the right treatment decision
👨⚕️ Dr. Rodrigo Arrangoiz, MD
Surgical Oncologist – Thyroid, Head & Neck, Breast
it is a tool that helps ensure you get the right care and avoid unnecessary treatment.
📚 References
Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid Haugen BR et al. ATA Guidelines for Thyroid Nodules. Thyroid Gharib H et al. Fine-Needle Aspiration of Thyroid Nodules. Endocrine Practice
Is recommended for most ADH lesions diagnosed on core needle breast biopsy (CNB)
The chance of upgrade at excision to:
Ductal carcinoma in situ (DCIS) or invasive carcinoma is generally in the:
12% to 22% range in the literature
The need for routine excision of pure flat epithelial atypia (FEA) has been less clear:
Some authors have reported an upgrade rate of 9.6% following excision of lesions that show pure FEA without ADH when the vast majority of biopsies were done with a 14-gauge spring-loaded core biopsy device:
It is not clear that biopsy with a vacuum-assisted device would yield the same results:
In fact, in one study reporting biopsy of low-risk calcifications with a vacuum-assisted device, pure FEA never resulted in an upgrade to malignancy
An article from the Mayo Clinic:
Showed that FEA does not seem to convey an independent risk of breast cancer beyond that of associated proliferative disease without atypia or associated ADH
The risk of upgrade at surgical excision for ADH:
Has been reported to correlate with the number of ducts or terminal duct lobular units involved on vacuum-assisted core biopsy:
With two or fewer foci of involvement:
There was no upgrade on excision
With four or more foci of involvement:
There was a strong probability of upgrade to ductal carcinoma in situ or invasive carcinoma at excision
Work continues to try to define a low-risk group who could potentially avoid excisional biopsy:
Particularly those with small areas of calcifications completely removed with core needle biopsy and only focal ADH on pathology
Apocrine metaplasia, florid epithelial hyperplasia of the usual variety, and columnar cell change without atypia:
Do not confer a significant risk of upgrade and do not require excision
References
Eby PR, Ochsner JE, DeMartini WB, Allison KH, Peacock S, Lehman CD. Is surgical excision necessary for focal atypical ductal hyperplasia found at stereotactic vacuum-assisted breast biopsy? Ann Surg Oncol. 2008;15(11):3232-3238.
Ely KA, Carter BA, Jensen RA, Simpson JF, Page DL. Core biopsy of the breast with atypical ductal hyperplasia: a probabilistic approach to reporting. Am J Surg Pathol. 2001;25(8):1017-1021.
Khoumais NA, Scaranelo AM, Moshonov H, Kulkarni SR, Miller N, McCready DR, et al. Incidence of breast cancer in patients with pure flat epithelial atypia diagnosed at core-needle biopsy of the breast. Ann Surg Oncol. 2013;20(1):133-138.
Said SM, Visscher DW, Nassar A, Frank RD, Vierkant RA, Frost MH, et al. Flat epithelial atypia and risk of breast cancer: a Mayo cohort study. Cancer. 2015;121(10):1548-1555.
McGhan LJ, Pockaj BA, Wasif N, Giurescu ME, McCullough AE, Gray RJ. Atypical ductal hyperplasia on core biopsy: an automatic trigger for excisional biopsy? Ann Surg Oncol. 2012;19(10):3264-3269.
it’s to biopsy the right nodule at the right time.
📚 References
Haugen BR et al. ATA Guidelines for Thyroid Nodules. Thyroid Tessler FN et al. ACR TI-RADS. Radiology Gharib H et al. Fine-Needle Aspiration of Thyroid Nodules. Endocrine Practice
Not all thyroid nodules are the same. Ultrasound risk stratification helps determine which nodules need biopsy and which can be safely observed.
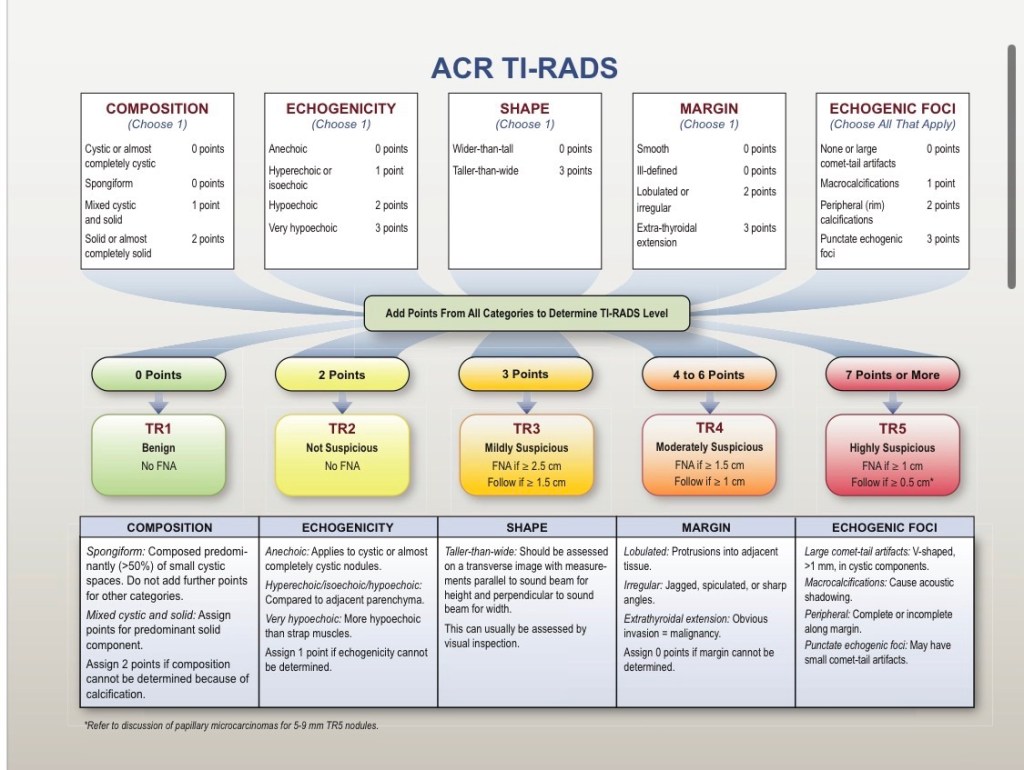
🔍 What are TI-RADS and ATA?
ACR TI-RADS and ATA ultrasound patterns are validated systems that estimate cancer risk based on ultrasound features—not symptoms. They standardize care and reduce unnecessary biopsies and surgeries.
📊 How do these systems work?
Ultrasound evaluates:
Composition (solid vs cystic) Echogenicity Margins Calcifications Shape (taller-than-wide)
Each feature contributes to a risk category, which guides:
✔️ Whether to biopsy
✔️ When to follow up
✔️ How closely to monitor
🧪 Key patient takeaway
Low-risk nodules → observation with periodic ultrasound Intermediate/high-risk nodules → biopsy at size thresholds ➡️ This approach is safe, evidence-based, and personalized.
🦋 Why this matters
Risk stratification:
Avoids overdiagnosis Focuses treatment on clinically meaningful disease Improves patient reassurance and outcomes